Streptococcus pneumoniae: Properties, Pathogenesis, and Diagnosis
Streptococcus pneumoniae morphology, virulence factors like pneumolysin and capsule, and the optochin and bile solubility tests used for lab diagnosis.
Streptococcus pneumoniae (pneumococci) is a part of the normal nasopharyngeal and oropharyngeal flora. It is an important etiological agent of upper and lower respiratory tract infections (URTI and LRTI), bacteremia, and septicemia. Streptococcus pneumoniae is also associated with otitis media, sinusitis, meningitis, and endocarditis.
Streptococcus pneumoniae is a Gram-positive cocci, typically lancet-shaped, and occurs singly, in pairs (diplococci), or short chains. They are non-motile and encapsulated. S. pneumoniae is a fastidious bacterium that grows best at 35-37°C with ~5% CO2 (or in a candle jar).
Diseases caused by Streptococcus pneumoniae
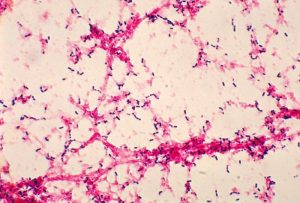 Figure: Streptococcus pneumoniae in Gram Staining
Figure: Streptococcus pneumoniae in Gram Staining
- Bacterial pneumonia: Most common bacterial cause, especially in infants and the elderly. Pneumococci in alveoli stimulate the release of fluid, red and white cells producing “rusty sputum.”
- Meningitis: one of the most common causes of meningitis (Others are Haemophilus influenzae, and Neisseria meningitidis). CSF generally has very high WBC and low glucose.
- Otitis media: common in children.
- Sinusitis: common in children.
- Bronchitis
- Bacteremia and other infectious processes
Virulence factors of Streptococcus pneumoniae and How They Cause Disease
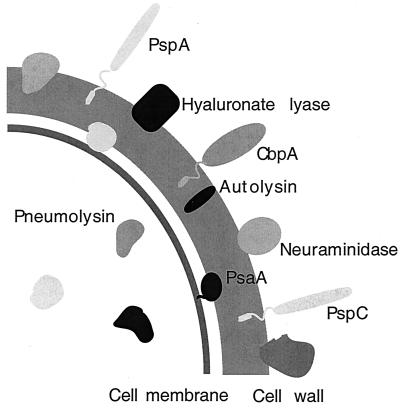 Figure: Schematic diagram of the virulence factors of Streptococcus pneumoniae
Figure: Schematic diagram of the virulence factors of Streptococcus pneumoniae
Four things have to happen, in roughly this order, for pneumococcus to go from harmless nasal colonizer to the organism causing meningitis: it sticks, it sneaks past the mucosal guard, it hides, and when conditions are right, it self-destructs to attack.
- Teichoic acid anchors the organism to respiratory and endothelial epithelium. Clinical link: this is the first step in colonization, no adherence, no infection.
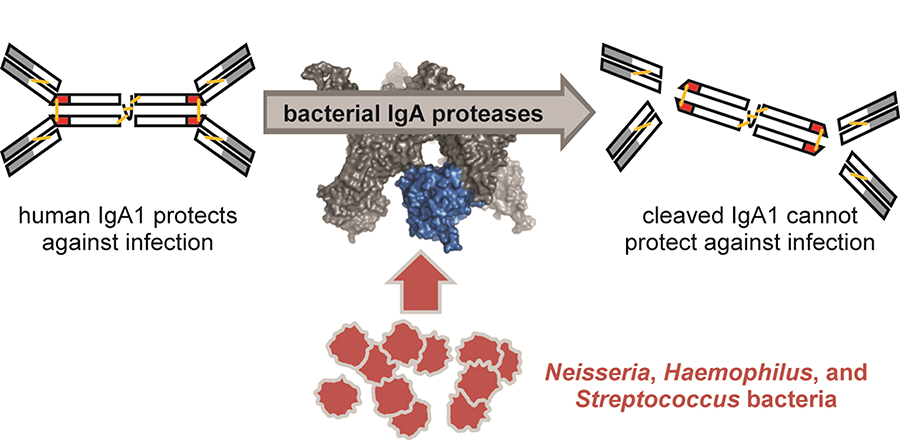
- IgA1 protease cleaves IgA1, the antibody that normally patrols and protects mucosal surfaces. Clinical link: this is specifically why pneumococcus, along with H. influenzae and N. meningitidis, can establish itself on a mucosal surface that should otherwise be defended.
 - Polysaccharide capsule, the single most important virulence factor here. It blocks complement-mediated opsonization and phagocytosis, and physically resists mechanical clearance by mucus. Non-encapsulated mutants lose virulence almost entirely in animal models. Clinical link: more than 93 capsular serotypes exist, and the pneumococcal vaccines are built directly around this capsule, immunity is type-specific because the capsule itself is the target.
- Polysaccharide capsule, the single most important virulence factor here. It blocks complement-mediated opsonization and phagocytosis, and physically resists mechanical clearance by mucus. Non-encapsulated mutants lose virulence almost entirely in animal models. Clinical link: more than 93 capsular serotypes exist, and the pneumococcal vaccines are built directly around this capsule, immunity is type-specific because the capsule itself is the target.
- Autolysin (LytA), a peptidoglycan-degrading enzyme that triggers the bacterium's own stationary-phase lysis. Clinical link: this is the mechanism, not a side effect, autolysin is what releases pneumolysin into surrounding tissue. It's also why old cultures show collapsed, flattened colonies (draughtsman colonies) by 24-48 hours.
- Pneumolysin, a pore-forming toxin that targets any host cell membrane containing cholesterol, essentially all human cells. It damages respiratory epithelium, inhibits the neutrophil respiratory burst, and interferes with classical complement fixation. Clinical link: this is the direct cause of tissue damage in pneumonia and meningitis, and the reason damage isn't confined to one tissue type.
- Other contributors: pneumococcal surface protein A (PspA, blocks complement), neuraminidase (aids colonization by acting on host glycans), peptidoglycan/teichoic acid fragments (highly inflammatory in the CNS, contributing to the damage seen in meningitis even after bacteria are cleared).
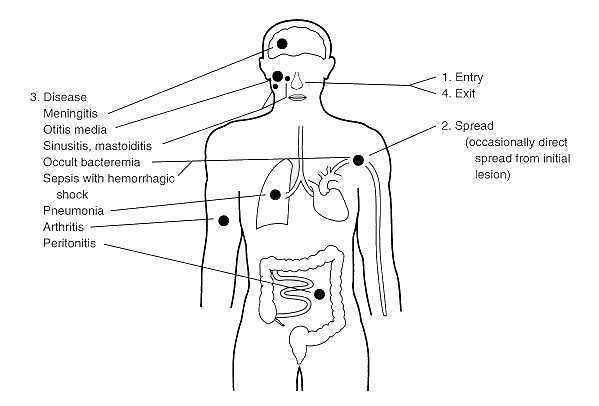 Figure: Types of disease caused by Streptococcus pneumoniae
Figure: Types of disease caused by Streptococcus pneumoniae
How to Remember the Virulence Factors
Think of it as four steps: Stick, Sneak, Hide, Self-destruct.
Stick. Teichoic acid is Velcro, it gets the organism attached to the respiratory lining before anything else can happen.
Sneak. IgA1 protease is a key cut specifically for one lock. IgA1 is the guard posted at every mucosal surface in your body, and this enzyme is shaped to disable exactly that guard and no other antibody class. That specificity is the giveaway that this is a deliberately evolved mechanism, not incidental damage.
Hide. The capsule is an invisibility cloak. Strip it off in the lab and the organism becomes almost harmless, which tells you the capsule isn't just one feature among many, it's the main reason this organism survives contact with your immune system at all.
Self-destruct. This is the one students remember once they hear it right: autolysin is a soldier pulling the pin on a grenade. The bacterium triggers its own cell wall breakdown, and the explosion releases pneumolysin into the surrounding tissue. The bacterium doesn't survive that moment, but the toxin it released does the damage. This single mechanism explains two separate observations in the lab and the clinic at once: why old pneumococcal colonies collapse into a flattened "draughtsman" shape (the autolysin has fired), and why pneumonia and meningitis both involve direct tissue destruction rather than just inflammation (the pneumolysin that autolysin released is doing it).
One more hook that costs nothing: pneumolysin needs cholesterol to punch its pore. Nearly every human cell membrane has cholesterol. That's the whole reason this one toxin causes damage in lung, meninges, and elsewhere rather than being tissue-specific.
Reservoirs: Harmlessly inhabit the upper respiratory tract of humans.
Transmission: Respiratory droplets are not considered highly communicable. Often colonizes without causing infection.
Laboratory diagnosis
Laboratory diagnosis of Streptococcus pneumoniae infection is based on finding characteristics shape of the organism in the sample, characteristic colony morphology, biochemical reactions, susceptibility to certain diagnostic discs, and latex agglutination test.
Sample
Specimens used for the laboratory diagnosis of Streptococcus pneumoniae maybe one or more of the followings depending on the clinical case
- Specimens from respiratory tract: Sputum, lung aspirate, pleural fluid
- Body fluids, e.g., Blood/ cerebrospinal fluid
- Exudates from the joint, middle ear, and other sites
Sample Collection
- Sputum
Collect > 1.0 ml expectorated sputum in a sterile screw-capped container. - Lung aspirate/ pleural fluid
Collect > 1.0 ml by percutaneous needle aspiration in a sterile screw-capped tube. - Blood
Clean the venipuncture site with 70% alcohol and iodine, allow it to evaporate, and collect blood aseptically in a culture broth with an anticoagulant. In case of adults, collect 5-10 ml of blood in culture bottle. For children < 12-year-old, collect 1.5-2.0 ml of blood. Mix the blood and broth by rotating gently to avoid clotting. - Cerebrospinal fluid (CSF)
Clean the skin over L3-L4 inter-space with 70% alcohol and iodine. Collect > 1.0 ml CSF in a sterile screw-capped tube. Keep the CSF in an incubator at 35-37 degree centigrade, if not processed immediately. - Exudates from joints/middle ear
Collect > 1.0 ml by aspiration in a sterile screw-capped tube or add directly to a culture broth used for blood culture.
Note: DO NOT REFRIGERATE THE SAMPLE
Sample Transport
Streptococcus pneumoniae is a fastidious bacteria. Care must be taken during the transport of specimens. Specimens must be transported promptly to the laboratory within 1-2 hours.
Blood can only be transported after collecting in a culture broth containing appropriate anticoagulant. The inoculated medium can be held at room temperature (20°C– 25°C) for 4 – 6 hours before incubation at 37°C. The samples during transportation should be protected from extremes of temperature (less than 18°C, more than 30°C) and direct sunlight.
Culture and Identification
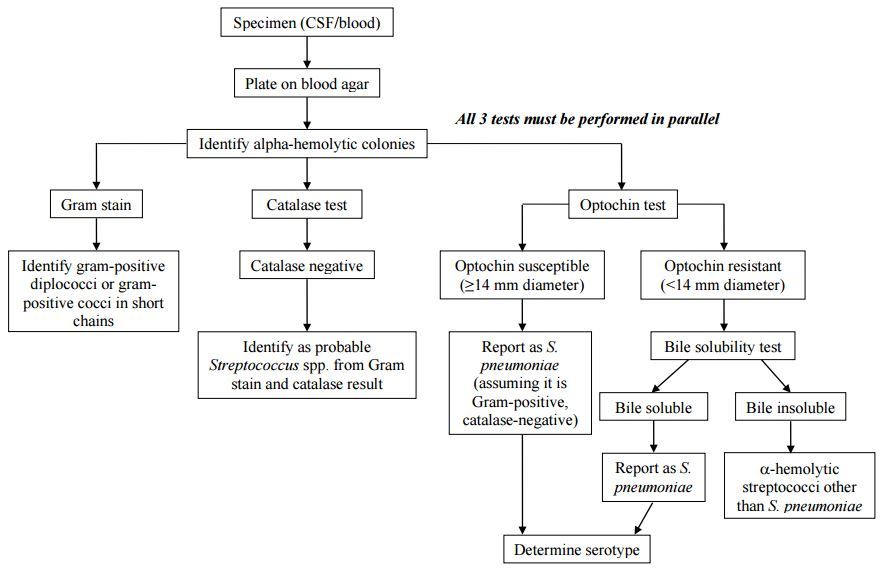 Figure: Flow chart for identification and characterization of a S. pneumoniae isolate
Figure: Flow chart for identification and characterization of a S. pneumoniae isolate
- Perform Gram staining of the sample (sputum/CSF)
- Gram staining shows Gram-positive lanceolate-shaped diplococci
 Figure: Gram positive diplococci: Streptococcus spp
Figure: Gram positive diplococci: Streptococcus spp
Culture and Sensitivity
- Inoculate sample onto blood agar and chocolate agar plate.
- Incubate at 37°C with 5-10% CO2 for 24 – 48 hours.
Colony morphology
- Colonies on blood agar plate are small (0.5 mm), round, translucent, or mucoid with alpha-hemolysis (A green discoloration of the agar around the colonies). Alpha-hemolytic property differentiates S. pneumoniae from many species, but not from the commensal alpha-hemolytic viridans streptococci.
- Young alpha-hemolytic colonies appear raised, and in 24 – 48 hours, colonies are flattened with a depressed center called the draughtsman colony. It is due to partial autolysis (these colonies are tentatively identified as Pneumococci).
- Streptococcus viridans also produces alpha-hemolytic colonies but does not produce draughtsman colony.
Colony characteristics: Alpha hemolytic (partial discoloration around the bacterial colony in blood agar), mucoid colony (if organism possesses polysaccharide capsule).
 Figure: Draughtsman colonies of S.pneumoniae
Figure: Draughtsman colonies of S.pneumoniae
The following confirmatory tests further identify alpha-hemolytic colonies.
Rapid test: Catalase test: negative (no gas bubble formed when colonies of Streptococcus pneumoniae are emulsified in hydrogen peroxide solution).
Optochin test
Optochin (ethylhydrocupreine hydrochloride) selectively disrupts the S. pneumoniae cell membrane at concentrations that don't affect related alpha-hemolytic streptococci.
Interpretation for identifying S. pneumoniae:
- Zone ≥14mm: susceptible, diagnostic of S. pneumoniae
- Zone <14mm, including no zone at all: equivocal, must be confirmed with bile solubility before ruling pneumococcus out
Read more: Optochin Sensitivity Test
 Figure: Alpha hemolysis in Blood Agar by Streptococcus pneumoniae, Observe the zone of inhibition around Optochin disk.
Figure: Alpha hemolysis in Blood Agar by Streptococcus pneumoniae, Observe the zone of inhibition around Optochin disk.
Bile solubility test
Bile salts (sodium deoxycholate) activate the pneumococcus's own autolysin, the same self-destruct enzyme described in the Virulence section above. This test doesn't use some separate lab trick, it simply triggers the organism's own lysis mechanism directly in a tube.
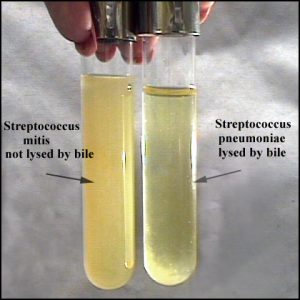 Figure: Bile solubility test: Streptococcus pneumoniae colonies are lysed by bile
Figure: Bile solubility test: Streptococcus pneumoniae colonies are lysed by bile
Interpretation: clearing or loss of turbidity = soluble = positive = confirms S. pneumoniae. Persistent turbidity = insoluble = negative, organism is not S. pneumoniae, most likely viridans streptococci.
Read more: Full procedure: Bile Solubility Test
Biochemical Tests for *S. pneumoniae*
Name of the test | Result |
Catalase Test | Negative |
Optochin sensitivity test | Sensitive |
Bile solubility test | Soluble |
Hemolysis | Alpha-hemolysis |
Oxidase Test | Negative |
O/F Test | Fermentative |
Motility | Non-motile |
Detection of the antigen
C-carbohydrate antigen of the Streptococcus pneumoniae can be detected in the urine for the diagnosis of pneumonia and in CSF for the diagnosis of pneumococcal meningitis.
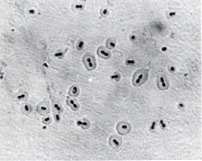 Figure: Streptococcus pneumoniae shows a quellung positive reaction.
Figure: Streptococcus pneumoniae shows a quellung positive reaction.
Quellung Reaction: Positive
When Streptococcus pneumoniae of certain types are mixed with specific antipolysaccharide serum of the same type or with polyvalent antiserum on a microscope slide, the capsule swells markedly, and the organism agglutinates by cross-linking of the antibodies.
Where students actually get confused
- Any optochin zone under 14mm is not a negative result, it's an unfinished test. This is the single most common error. Whether the zone is 10mm, 5mm, or completely absent, the next step is identical: bile solubility. Don't try to read meaning into the exact sub-14mm size, treat all of them the same way until bile solubility settles it.
- Viridans streptococci will trip up an optochin-only workflow. Both are alpha-hemolytic on Blood Agar, and both can look superficially similar on Gram stain. The real differentiators are the draughtsman colony (pneumococcus only), capsule presence, optochin sensitivity, and bile solubility, not hemolysis pattern alone, since viridans is also alpha-hemolytic.
- Bile solubility and bile esculin are not the same test. Bile solubility lyses pneumococcus colonies in the presence of bile salts and confirms S. pneumoniae. Bile esculin tests for esculin hydrolysis in the presence of bile and is used for Enterococcus and Group D Streptococcus. Same word "bile," completely different organisms and completely different mechanisms.
- Catalase negative only rules out Staphylococcus, it doesn't confirm pneumococcus. All streptococci, including the harmless viridans group, are catalase-negative. Catalase tells you "not Staph," nothing more.
Antimicrobial susceptibility
- Perform antimicrobial susceptibility test against a selected group of antimicrobials by a disk-diffusion method
- Reporting of results: Streptococcus pneumoniae isolated and resistance patterns with tested antibiotics
Antimicrobial Resistance
Initially, penicillin was the drug of choice to treat S. pneumoniae infections as all S. pneumoniae isolates were exquisitely susceptible to penicillin. Still, now drug-resistant S.pneumoniae (DRSP) poses a serious threat to global health as we are observing an alarming worldwide increase in the incidence.
 Figure: Antimicrobial sensitivity testing of Streptococcus pneumoniae
Figure: Antimicrobial sensitivity testing of Streptococcus pneumoniae
Key exam facts in one table
Remember this mnemonic: Streptococcus pneumoniae is the BOSS of community-acquired pneumonia: alpha-hemolytic on Blood Agar, Bile Soluble, Optochin Sensitive. But even a BOSS doesn't show up unprotected, it wears a sugar-coated capsule as armor against your immune system, the reason it has 90-plus serotypes and the reason the vaccine targets exactly that coat."
| Feature | S. pneumoniae | Memory hook |
|---|---|---|
| Gram stain | Lancet-shaped diplococci | Two flames pointed at each other, the "lancet" shape |
| Catalase | Negative | Rules out Staph, nothing more |
| Optochin | Sensitive | The "O" in BOSS |
| Bile solubility | Soluble | The "B" in BOSS |
| Hemolysis | Alpha | Same as viridans, not a differentiator alone |
| Colony at 24-48h | Draughtsman (flattened, depressed center) | Autolysin has fired, the soldier pulled the pin |
| Main virulence factor | Polysaccharide capsule | Remove it, virulence collapses |
| Tissue-damage toxin | Pneumolysin | Needs cholesterol, hits nearly any human cell |
| CSF findings in meningitis | High WBC, low glucose | Bacteria are eating the glucose and drawing in white cells |
Self-check questions
- Why doesn't a small or absent optochin zone alone rule out S. pneumoniae?
- What does the draughtsman colony appearance tell you about which virulence factor has just activated?
- Why does pneumolysin damage tissue as different as lung epithelium and meninges, rather than acting on just one tissue type?
- A catalase-negative, alpha-hemolytic, optochin-resistant organism is isolated from a throat swab. What is your leading differential, and what confirms it?
- Why is the pneumococcal vaccine built around the capsule specifically, rather than another virulence factor?
References
- Bogaert, D., De Groot, R., & Hermans, P. W. (2004). Streptococcus pneumoniae colonisation: the key to pneumococcal disease. The Lancet Infectious Diseases, 4(3), 144-154. https://doi.org/10.1016/S1473-3099(04)00938-7
- Mitchell, A. M., & Mitchell, T. J. (2010). Streptococcus pneumoniae: virulence factors and variation. Clinical Microbiology and Infection, 16(5), 411-418. https://doi.org/10.1111/j.1469-0691.2010.03183.x
- O'Brien, K. L., Wolfson, L. J., Watt, J. P., et al. (2009). Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. The Lancet, 374(9693), 893-902. https://doi.org/10.1016/S0140-6736(09)61204-6
- Jacobs, M. R. (2004). Streptococcus pneumoniae: epidemiology and patterns of resistance. The American Journal of Medicine, 117(Suppl 3A), 3S-15S. https://doi.org/10.1016/j.amjmed.2004.07.003
- Jedrzejas, M. J. (2001). Pneumococcal virulence factors: structure and function. Microbiology and Molecular Biology Reviews, 65(2), 187-207. https://doi.org/10.1128/MMBR.65.2.187-207.2001
- Mellroth, P., Daniels, R., Eberhardt, A., et al. (2012). LytA, major autolysin of Streptococcus pneumoniae, requires access to nascent peptidoglycan. Journal of Biological Chemistry, 287(14), 11018-11029. https://pmc.ncbi.nlm.nih.gov/articles/PMC3322828/
- Hyams, C., Camberlein, E., Cohen, J. M., Bax, K., & Brown, J. S. (2010). The Streptococcus pneumoniae capsule inhibits complement activity and neutrophil phagocytosis by multiple mechanisms. Infection and Immunity, 78(2), 704-715. https://doi.org/10.1128/IAI.00881-09
Frequently Asked Questions
Why is Streptococcus pneumoniae alpha-hemolytic like viridans streptococci, yet far more dangerous?
What is the difference between bile solubility and bile esculin tests?
Why does the pneumococcal vaccine need to cover so many different serotypes?
Can Streptococcus pneumoniae be part of normal flora without causing disease?
Why does CSF show low glucose in pneumococcal meningitis?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.