Bacterial Capsule: Importance, Capsulated Bacteria
Bacterial capsule — structure, composition (homo/heteropolysaccharide, polypeptide), anti-phagocytic function, vaccine development, and clinically important capsulated bacteria. With mnemonics and clinical stories on why encapsulated organisms are so dangerous.
Some bacterial cells are surrounded by a viscous substance forming a covering layer or envelope around the cell wall, called a capsule. Bacterial capsules can be visualized by light microscopy using special staining methods. If the layer is too thin to be seen by light microscopy, it is termed a microcapsule. It is called the slime layer if it is so abundant that many cells are embedded in a common matrix.
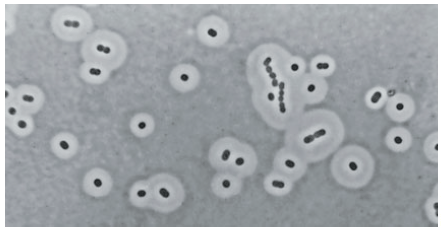 Figure: Capsules of Acinetobacter species as seen under phase-contrast microscopy after negative staining (Image source: Elliot Juni)
Figure: Capsules of Acinetobacter species as seen under phase-contrast microscopy after negative staining (Image source: Elliot Juni)
Capsule (also known as K antigen) is a major virulence factor of bacteria. The principal pathogens that cause pneumonia and meningitis include Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis, Klebsiella pneumoniae, Escherichia coli, and group B streptococci have polysaccharide capsules on their surface. Nonencapsulated mutants of these organisms are avirulent.
Structure and Composition
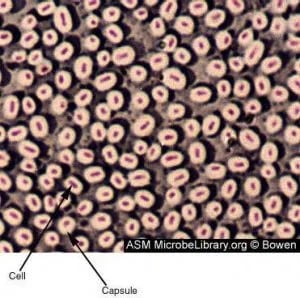 Figure: Bacterial Capsule
Figure: Bacterial Capsule
Capsule is a gelatinous layer covering the entire bacterium. In light microscopy, capsules appear to be amorphous gelatinous areas surrounding the cell. Capsule is located immediately exterior to the murein (peptidoglycan) layer of gram-positive bacteria and the outer membrane (Lipopolysaccharide layer) of gram-negative bacteria. In electron microscopy, the capsule appears like a mesh or network of fine strands.
Most bacterial capsules are polysaccharides (i.e. poly: many, saccharide: sugar). These polymers are composed of repeating oligosaccharide units of two to four monosaccharides. Capsules composed of single kinds of sugars are termed homopolysaccharides. For example, the capsule of Streptococcus mutans is made up of glucose polymers. If several kinds of sugars are present in a capsule, then it is called heteropolysaccharides, eg., the capsule of Klebsiella pneumoniae. The capsule of Bacillus anthracis is an exception; this polypeptide capsule is composed of polymerized D-glutamic acid.
The sugar components of polysaccharides vary within the species of bacteria, which determines their serologic types. Example: Streptococcus pneumoniae has 84 different serotypes discovered so far.
Why the capsule is one of the most important virulence factors you will study
Here is the single fact that makes capsule biology unforgettable: the difference between a harmless bacterium living quietly in your nose and a life-threatening invader causing meningitis can be a single gene controlling capsule production.
This is not an exaggeration. Streptococcus pneumoniae and Neisseria meningitidis both colonise the human nasopharynx asymptomatically in large numbers of healthy people. The vast majority of the time, nothing happens. But when an encapsulated strain breaches local defences and enters the bloodstream, the capsule becomes the single factor that determines whether the host's immune system can clear the infection in hours — or whether the bacteria multiply unchecked, causing sepsis and death within a day.
This single virulence factor is so important that three of the world's most successful vaccines were developed by directly targeting bacterial capsules: the pneumococcal vaccine (PCV13/PPSV23), the meningococcal vaccine (MenACWY/MenB), and the Haemophilus influenzae type b vaccine (Hib). Understanding capsule biology is understanding why these vaccines work — and why unvaccinated children remain at devastating risk from these organisms.
Based on their composition, capsules are of three types: homopolysaccharides, heteropolysaccharides, and polypeptides.
- Homopolysaccharides: Capsules made up of a single kind of sugar. E.g., Streptococcus mutans
- Heteropolysaccharides: Capsules are made up of several types of sugars. E.g., Klebsiella pneumoniae
- Polypeptides: Capsules are made up of a long chain of amino acids. E.g., Bacillus anthracis
Capsule Vs. Slime Layers
Slime is a loose network of polymers extending outward from a cell, whereas a capsule is a dense and well-defined polymer layer surrounding the cell. Both capsules and slime layers are essential for the adherence of microorganisms and subsequent colonization, but they differ in some of their properties.
Difference between capsule and slime layers
Properties | Capsule | Slime Layer |
Organization | In capsule, polysaccharide layer is organized in a tight matrix that excludes small particles, such as India ink; it is called a capsule | In slime layer, polysaccharide layer is more easily deformed, do not exclude particles and is more difficult to see. |
Adherence | Capsules typically adhere firmly to the cell wall, and some are even covalently linked to peptidoglycan | Slime layers, by contrast, are loosely attached and can be lost from the cell surface. |
Role in pathogenesis | Capsule of pathogenic Escherichia coli promotes adherence to the brush border of intestinal microvilli. | Dextran slime layer of Streptococcus mutans promotes binding to tooth surfaces. |
Importance of Bacterial Capsule
- Virulence determinants
Capsules are anti-phagocytic. They limit the ability of phagocytes to engulf the bacteria. The capsule’s smooth nature and negative charge prevent the phagocyte from adhering to and engulfing the bacterial cell. If pathogenic bacteria lose capsules (by mutation), they won’t be able to cause disease (i.e. loses disease-causing capacity). Polysaccharide capsule is the major virulence factor for Streptococcus pneumoniae. Encapsulated strains of S. pneumoniae grow in lung tissues in enormous numbers, where they initiate host responses that lead to pneumonia. Nonencapsulated strains are less pathogenic; they are quickly and efficiently ingested and destroyed by phagocytes via phagocytosis.
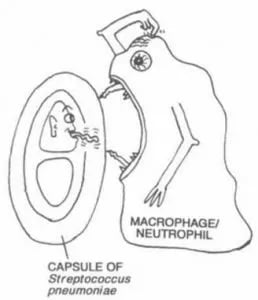 Figure: Anti-phagocytic nature of Bacterial capsule
Figure: Anti-phagocytic nature of Bacterial capsule
- Saving engulfed bacteria from the action of neutrophil
Bacterial capsule prevents the direct access of lysosome contents with the bacterial cell, preventing their killing.
- Prevention of complement-mediated bacterial cell lysis
Capsule of gram-positive bacteria such as S. pneumoniae prevents interaction between C3b deposited on the bacterial membrane and the CR1 on phagocytic cells.
- Protection of anaerobes from oxygen toxicity
- Identification of bacteria
- Using specific antiserum against capsular polysaccharide. E.g. Quellung reaction.
- Colony characteristics in culture media: Bacteria with capsules form smooth (S) colonies while those without capsules form rough (R) colonies. A given bacterial species may undergo a phenomenon called S-R variation, whereby the cell loses the ability to form a capsule. Some capsules are very large and absorb water; bacteria with this type of capsule (e.g., Klebsiella pneumoniae) form mucoid (M) colonies.
 Figure: Mixed growth of mucoid Lactose fermenting colonies and NLF colonies in MacConkey Agar
Figure: Mixed growth of mucoid Lactose fermenting colonies and NLF colonies in MacConkey Agar
- Development of Vaccines
Capsular polysaccharides are used as antigens in certain vaccines. For examples:
- Polyvalent (23 serotypes) polysaccharide vaccine of Streptococcus pneumoniae.
- Polyvalent (4 serotypes) vaccine of Neisseria meningitidis.
- A monovalent vaccine made up of capsular material from Haemophilus influenzae.
- Initiation of infection
Capsules help the organism adhere to host cells. The capsule also facilitates and maintains bacterial colonization of biological (e.g. teeth) and inanimate (e.g. prosthetic heart valves) surfaces through the formation of biofilms.
- Capsule also acts as receptors for bacteriophages
The analogy that makes anti-phagocytic function unforgettable
Think of a neutrophil as a person trying to grab a slippery, soap-coated ball.
A non-encapsulated bacterium is like a dry, textured ball — easy to grip, easy to engulf. A neutrophil's surface receptors can latch onto the bacterial cell wall directly, triggering phagocytosis within seconds.
An encapsulated bacterium is like that same ball coated in slippery soap — the neutrophil's receptors simply cannot get a grip. The smooth, hydrated, negatively-charged capsule physically and electrostatically repels the phagocyte's attempts at adhesion. No adhesion means no engulfment, no engulfment means the bacterium survives and multiplies freely in the bloodstream.
This is why "losing the capsule equals losing virulence" is such a clean, testable biological principle. Laboratory strains of S. pneumoniae that spontaneously lose capsule production through mutation become "rough" colonies (instead of smooth, mucoid colonies) and lose almost all their ability to cause invasive disease — even though every other gene in the bacterium is identical. This single observation, made decades ago by Griffith and later mechanistically explained by Avery, MacLeod, and McCarty, was actually the foundational experiment that proved DNA is the genetic material — one of the most important discoveries in the history of biology, made possible by studying pneumococcal capsules.
How the Immune System Eventually Overcomes the Capsule — Opsonization
If capsules are so effective at blocking phagocytosis, how does the immune system ever clear an encapsulated infection? The answer is opsonization — coating the bacterium with proteins that phagocytes can recognize even through the capsule.
Two opsonins matter most:
1. Complement (C3b) — the complement system can deposit C3b molecules onto the bacterial surface even underneath a capsule, in small amounts, through the alternative pathway. Phagocytes have specific C3b receptors (CR1) that can grip the C3b "handle" sticking through or around the capsule, even when they cannot grip the bacterium directly.
2. Specific antibody (opsonizing antibody) — antibodies directed against capsular polysaccharide bind directly to the capsule surface. Once bound, the antibody's Fc region is recognized by Fc receptors on phagocytes, allowing efficient engulfment despite the capsule. This is precisely how capsular polysaccharide vaccines work — they stimulate the production of anticapsular antibodies before natural infection occurs, so that when the bacterium is encountered, opsonizing antibody is already present and phagocytosis proceeds efficiently.
Why this matters clinically — the splenectomy connection: The spleen is the primary site where poorly opsonized encapsulated bacteria are cleared from the blood, through a slow filtration process distinct from conventional phagocytosis. Patients who have had a splenectomy (surgical spleen removal) lose this clearance mechanism and become dramatically more susceptible to fulminant, rapidly fatal infections with encapsulated bacteria — a phenomenon called overwhelming post-splenectomy infection (OPSI). This is why all splenectomy patients require vaccination against S. pneumoniae, N. meningitidis, and H. influenzae type b — the three organisms whose capsules the spleen would normally help clear.
Clinically Important Encapsulated Organisms
| Organism | Capsule type | Composition | Disease | Detection method | Vaccine |
|---|---|---|---|---|---|
| Streptococcus pneumoniae | Heteropolysaccharide | 84+ distinct serotypes | Pneumonia, meningitis, otitis media, sepsis | Quellung reaction; optochin sensitivity | PCV13/PCV15/PCV20, PPSV23 |
| Klebsiella pneumoniae | Heteropolysaccharide | Very thick — gives mucoid "string test" positive colonies | Pneumonia, UTI, liver abscess, bacteraemia | Mucoid colony morphology; string test | None routinely available |
| Haemophilus influenzae type b | Heteropolysaccharide | Polyribosylribitol phosphate (PRP) | Meningitis, epiglottitis, septic arthritis (pre-vaccine era) | Quellung reaction; PRP antigen detection | Hib vaccine |
| Neisseria meningitidis | Heteropolysaccharide | 13 serogroups; A, B, C, W, Y, X clinically important | Bacterial meningitis, meningococcaemia, Waterhouse-Friderichsen syndrome | Latex agglutination; PCR | MenACWY, MenB |
| Bacillus anthracis | Polypeptide (exception) | Poly-D-glutamic acid | Anthrax (cutaneous, inhalation, GI) | Direct fluorescent antibody; PCR | Limited availability (military/high-risk) |
| Streptococcus pyogenes | Homopolysaccharide | Hyaluronic acid (identical to human connective tissue — molecular mimicry) | Pharyngitis, cellulitis, necrotising fasciitis, rheumatic fever | Not routinely visualised | None (capsule-based) |
| Streptococcus mutans | Homopolysaccharide | Glucose polymers (dextran) | Dental caries (not invasive disease) | Not clinically tested | None |
| Cryptococcus neoformans (fungus) | Polysaccharide | Glucuronoxylomannan (GXM) | Cryptococcal meningitis (especially in HIV/AIDS) | India ink preparation; cryptococcal antigen (CrAg) test | None |
| Pseudomonas aeruginosa (mucoid strains) | Exopolysaccharide | Alginate | Chronic lung infection in cystic fibrosis | Mucoid colony morphology on culture | None |
| Bacteroides fragilis | Polysaccharide | Capsular polysaccharide complex (CPC) | Intra-abdominal abscess | Not routinely visualised | None |
The unforgettable exception: Bacillus anthracis is the only clinically important bacterium with a polypeptide (not polysaccharide) capsule — made of poly-D-glutamic acid. This is genuinely unusual: D-amino acids are rarely used in biology (most proteins use L-amino acids), and this D-configuration makes the anthrax capsule resistant to host proteases that would normally degrade a peptide structure.
Histoplasma capsulatum is not a capsulated fungi.
How to Learn and Remember Bacterial Capsules
The mnemonic for major encapsulated bacteria — "**Some Killers Have Pretty Nasty Capsules**"
| Letter | Organism |
|---|---|
| S | Streptococcus pneumoniae |
| K | Klebsiella pneumoniae |
| H | Haemophilus influenzae type b |
| P | Pseudomonas aeruginosa (mucoid CF strains) |
| N | Neisseria meningitidis |
| C | Cryptococcus neoformans (the fungal exception) |
These six organisms account for the overwhelming majority of clinically significant capsule-related disease you will be tested on.
One sentence that captures the entire clinical relevance
"The capsule is a soap coating that blocks the immune system's grip — vaccines work by giving the immune system soap-resistant gloves (antibodies) in advance."
Three clinical stories that make capsules unforgettable
Story 1 — Griffith's mice and the birth of molecular biology In 1928, Frederick Griffith injected mice with heat-killed encapsulated (virulent) S. pneumoniae mixed with live non-encapsulated (avirulent) bacteria. Neither alone killed the mice — but the combination did. Something from the dead encapsulated bacteria had transformed the living non-encapsulated bacteria into deadly encapsulated ones. This single experiment, driven entirely by capsule biology, eventually led Avery, MacLeod, and McCarty to identify that "something" as DNA — proving DNA was the molecule of heredity, the foundational discovery of molecular genetics.
Story 2 — The post-splenectomy emergency A trauma patient has an emergency splenectomy after a car accident. Years later, they develop a mild fever and within 12 hours are in septic shock from pneumococcal sepsis — a presentation so rapid and severe it is specifically named "overwhelming post-splenectomy infection" (OPSI), with mortality rates of 50–70% even with treatment. The spleen they lost was their primary mechanism for clearing poorly opsonized encapsulated bacteria. This is precisely why every splenectomy patient must receive pneumococcal, meningococcal, and Hib vaccination — ideally before the splenectomy, or as soon as possible afterward.
Story 3 — The string test in the urine lab A junior lab technician touches an inoculation loop to a large, glistening, mucoid colony on a MacConkey plate and lifts — the colony stretches into a long string, several centimetres, before breaking. This "string test" is a simple bedside indicator of a thick polysaccharide capsule, and it is virtually diagnostic for Klebsiella pneumoniae among the lactose-fermenting Enterobacteriaceae. A confident technician can call this presumptive identification before any biochemical test is run.
Key exam facts in one table
| Question | Answer |
|---|---|
| What is the main function of the capsule? | Anti-phagocytic — prevents engulfment by neutrophils/macrophages |
| What two opsonins overcome capsule resistance? | C3b (complement) and specific antibody |
| Which organism has a polypeptide (not polysaccharide) capsule? | Bacillus anthracis (poly-D-glutamic acid) |
| What stain is used to visualise capsule? | Negative/capsule staining (India ink for Cryptococcus) |
| What test detects pneumococcal capsular swelling? | Quellung reaction |
| Why are splenectomy patients at risk from encapsulated bacteria? | Spleen normally clears poorly opsonized encapsulated organisms |
| What experiment first linked capsule loss to virulence loss? | Griffith's transformation experiment (1928) |
| What three vaccines directly target bacterial capsules? | Pneumococcal (PCV/PPSV), meningococcal (MenACWY/MenB), Hib |
| What does "string test positive" suggest? | Klebsiella pneumoniae (thick capsule) |
| Why is S. pyogenes capsule poorly immunogenic? | Made of hyaluronic acid — identical to human connective tissue (molecular mimicry avoids immune recognition) |
References and further reading
- Madigan, M. T., Bender, K. S., Buckley, D. H., Sattley, W. M., & Stahl, D. A. (2018). Brock Biology of Microorganisms (15th ed.). Pearson.
- Tille, P. M. (2017). Bailey & Scott's Diagnostic Microbiology (14th ed.). Mosby Elsevier.
- Murray, P. R., Rosenthal, K. S., & Pfaller, M. A. (2020). Medical Microbiology (9th ed.). Elsevier.
- Avery, O. T., MacLeod, C. M., & McCarty, M. (1944). Studies on the chemical nature of the substance inducing transformation of pneumococcal types. Journal of Experimental Medicine, 79(2), 137–158. https://doi.org/10.1084/jem.79.2.137
Frequently Asked Questions
Why does the bacterial capsule prevent phagocytosis?
How does the immune system eventually clear capsulated bacterial infections?
Why are splenectomy patients at increased risk from encapsulated bacteria?
What is the difference between homopolysaccharide, heteropolysaccharide, and polypeptide capsules?
How was the bacterial capsule connected to the discovery that DNA is the genetic material?
Why is the Streptococcus pyogenes capsule poorly recognized by the immune system?
What is the string test and which organism does it identify?
Why does Cryptococcus neoformans appear differently from bacterial capsules under the microscope?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.