Vibrio Cholerae: Characteristics, Pathogenesis, and Lab Diagnosis
How to confirm Vibrio cholerae from a diarrheal outbreak: TCBS culture, string test vs Aeromonas, serotyping O1/O139, and ORS-first treatment.
Three patients arrive at a district hospital in southern Nepal within two hours of each other, all presenting with sudden onset of profuse watery diarrhoea, vomiting, and rapidly progressing dehydration. Their stools are pale, watery, and odourless; the rice-water appearance that experienced clinicians immediately recognise as a possible cholera signal. A fourth patient arrives while the first three are being triaged. This is the beginning of an outbreak, and the laboratory is being asked one question right now: is this Vibrio cholerae O1 or O139, or is it something else?
The answer matters because the public health response is entirely different depending on it. Vibrio cholerae O1 and O139 trigger cholera outbreak protocols, contact tracing, water source investigation, and potentially mass ORS distribution. Aeromonas hydrophila; which grows on the same media, is oxidase-positive like Vibrio, and causes clinically similar diarrheal disease. Getting the right answer from a single fresh stool specimen within hours, in a laboratory without advanced molecular equipment, requires knowing the rapid presumptive test pathway: motility (darting movement stopped by antiserum), oxidase, TCBS culture, and the string test.
This article covers that entire diagnostic pathway (from specimen receipt to confirmed serotyping) and includes the string test mechanism and its limitations in full, since this test is both the most commonly misunderstood step in the pathway and the one that most directly separates Vibrio from its clinical mimics.
Cholera is an acute gut infection caused by ingesting food or water contaminated with the bacterium Vibrio choleraeO1 or O139. Other serogroups of Vibrio choleraemay cause diarrheal disease and other infections.
- Vibrio parahaemolyticus is an important cause of enteritis.
- Characterized by copious (voluminous watery stools), painless, watery diarrhea often accompanied by vomiting
- Death occurs by dehydration (hypovolemic shock or acidosis) if left untreated.
- Cholera is preventable; up to 80% of cholera cases can be successfully managed with oral rehydration salts (ORS).
Characteristics of Vibrio cholerae
- Gram-negative curved bacilli (comma-shaped)
- Highly motile (darting type of motility) with a single polar flagellum (monotrichous)
- Oxidase-positive, catalase-positive
- Not a normal human flora
Primary habitat – brackish or marine water Transmitted by the ingestion of seafood, contaminated food, and water
- Ability to cause epidemics and pandemics
- Vibrios are sensitive to low pH and die rapidly in solution below pH 6 and tolerate alkaline media (pH 8.5)
- Antigen
Somatic O (>200 serotypes, agents of cholera O1, O139) Flagellar H
Vibrio cholerae strains
V. cholerae is divided into serogroups according to the nature of its O cell wall antigen. Two serogroups of V. choleraeO1 and O139 cause outbreaks. V. choleraeO1 causes most outbreaks, while O139 is confined to South-East Asia. Non-O1 and non-O139 V. cholerae can cause mild diarrhea but do not cause epidemics.
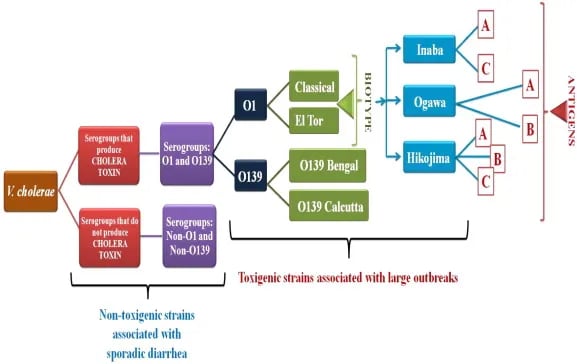 Figure: Vibrio cholerae serogroups and biotypes(source: sciencedirect.com)
Figure: Vibrio cholerae serogroups and biotypes(source: sciencedirect.com)
The O1 organisms have two biotypes, called classic and El Tor, and three serotypes called Ogawa, Inaba, and Hikojima. Biotypes are based on differences in biochemical reactions, whereas serotypes are based on antigenic differences.
People at risk
The risk of cholera is highest in areas where basic infrastructure is unavailable, such as peri-urban slums and refugees with limited access to safe drinking water and proper waste disposal. People with low immunity – such as malnourished children or people living with HIV – are at a greater risk of death if infected.
Mechanism of action of cholera toxin
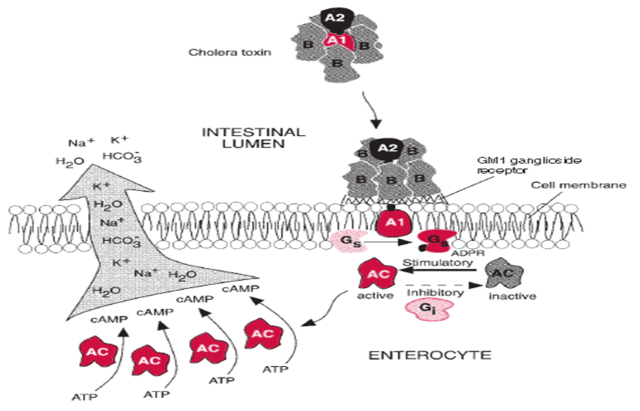 Figure: Mechanism of cholera toxin
Figure: Mechanism of cholera toxin
- V cholerae toxin consists of two subunits, A (A1: the toxic moiety and A2) and B.
- B subunit binds to the receptor GM1 ganglioside in the intestinal cell membrane and internalizes subunit A.
- ADP-ribosylation of the G protein of Adenylate cyclase occurs; it inhibits the action of GTPase and activates the adenylate cyclase.
- Activated adenylate cyclase catalyzes the transformation of ATP to cAMP.
- Increased levels of cAMP stimulate the cells to secrete ions into the intestinal lumen actively.
- To maintain osmotic stabilization, the cells then secrete fluid into the lumen.
- Patients become dehydrated and hypotensive rapidly as fluid is drawn from the intravascular compartment into the intestinal lumen.
Signs and Symptoms of cholera
- According to WHO, up to 75% of people infected with Vibrio choleraeO1 or O139 don’t develop any symptoms. Bacteria may present in their feces for 7–14 days after infection and are shed back into the environment.
- Among people who develop symptoms, 80% have mild or moderate symptoms, while around 20% develop acute watery diarrhea (rice watery stools).
- The incubation period of 6-48 hours
- Begins with the abrupt onset of watery diarrhea which is followed by several diarrheal episodes which may be accompanied by vomiting.
- Muscle cramps may occur as water and electrolytes are lost from body tissues.
- Disease outcome depends upon the extent of water and electrolyte loss and adequacy of water and electrolyte repletion therapy.
- If untreated, death can occur from hypovolemic shock, metabolic acidosis, and uremia.
Laboratory Diagnosis
- Sample: Fresh diarrheal stool or stool collected in Cary Blair transport medium.
- Macroscopic examination: Rice watery stool with mucus flecks
- The laboratory diagnosis of cholera is based on colony morphology, culture characteristics, biochemical reactions, and serological identification by slide agglutination using specific antisera. However, a presumptive diagnosis of cholera can be made by an immobilization test.
 Figure: Bacterium Vibrio cholerae which causes cholera
Figure: Bacterium Vibrio cholerae which causes cholera
I) Immobilization test: A rapid presumptive diagnosis of cholera can be made by observing the wet smear for the distinctive rapid to and fro movement (darting movement) of V. cholerae O1 and O139 due to their single polar flagellum. The movement can be stopped by adding one drop of V. cholerae O1 and O139 antiserum respectively.
Hanging drop method forVibrio cholerae is one of the easy but most popular tests used for the presumptive diagnosis.
II) Oxidase test: on performing an oxidase test from a pure sub-culture on nutrient agar, a positive reaction is observed. Oxidase test should not be performed directly from TCBS or MacConkey agar as acidification of these media may result in false-negative oxidase tests.
Note: Aeromonas spp. is also oxidase positive and can produce clinically similar diarrhoea; oxidase positivity alone does not confirm V. cholerae. The string test (see below) and serotyping are the next differentiation steps.
Cultural characteristics
- Fresh stool can be directly plated on a non-selective medium like MacConkey agar and a selective medium such as Thiosulphate Citrate Bile Salt Sucrose (TCBS) agar.
- However, in the case of a rectal swab, the swab stick should be dipped in 10 ml of alkaline peptone water (APW) and incubate for 6-8 hours. After incubation, inoculation on solid media should be done only from the pellicle formed at the upper layer of the broth. (Note: The broth should not be shaken before plating)
- After 18-24 hrs of incubation at 37°C observe the colony morphology.
MacConkey agar: Appearance of pale, non-lactose fermenting,1-2 mm in diameter, flat with a serrated margin. TCBS: Button-shaped yellow colonies of 1-2 mm diameter.
Biochemical Reactions
| Biochemical Tests | Reactions |
|---|---|
| Gram staining | Gram negative, curved rods |
| Catalase test | Positive |
| Oxidase test | Positive |
| Citrate Utilization test | Positive or Negative |
| Indole test | Positive |
| Urease test | Negative |
| Methyl Red (MR) test | Positive |
| Vogues Proskauer (VP) test | Negative |
| Motility test | Motile |
| String test | Positive (see String Test section below for principle and procedure) |
| TSI Agar test | R/Y (Alkali/Acid) or Y/Y (Acid/Acid) without gas and H2S |
String Test (Bile Salt Test)
The string test is a rapid, inexpensive bench-top procedure that uses the property of Vibrio cholerae's cell wall to help differentiate it from Aeromonas spp; the most clinically important differentiation challenge in diarrheal stool culture.
 Figure: A positive string test with V. cholerae. Image source: CDC
Figure: A positive string test with V. cholerae. Image source: CDC
Principle: When an isolated colony is emulsified in sodium deoxycholate or sodium taurocholate (0.5% bile salt solution), the bile salt lyses the cell wall of Vibrio cholerae, releasing intracellular DNA. The released DNA makes the suspension viscous. When the inoculating loop is slowly drawn upward from the emulsification, a thread-like mucoid "string" forms between the loop and the slide. This is the positive result.
Procedure:
- Take a clean, grease-free glass slide and place one drop of freshly prepared 0.5% bile salt solution
- Emulsify an isolated colony (18–24 hour growth) using an inoculating loop, rubbing vigorously for 2–3 minutes until the suspension becomes visibly viscous
- Slowly draw the loop upward from the slide
- Observe for the formation of a mucoid thread
Result and interpretation:
- Positive (V. cholerae): A mucoid string forms between loop and slide as the loop is drawn up
- Negative (Aeromonas, other non-Vibrio): No string forms; suspension breaks cleanly
Performance characteristics: Sensitivity approximately 86%, specificity approximately 70%. Because specificity is limited, the string test is a screening tool, not a confirmatory test. A positive string test narrows the field toward Vibrio cholerae but must be confirmed by serotyping (see Serological Reactions below). Both positive and negative string test results require further confirmation by other biochemical and serological methods.
Why this matters clinically: Vibrio cholerae and Aeromonas hydrophila produce very similar disease pictures (acute watery diarrhoea, diarrheal stool culture on TCBS), share oxidase positivity, and can appear morphologically similar on culture media. The string test is the single fastest bench-top step that begins to separate them at the colony level — before serology is performed. Aeromonas is string-test negative because its cell wall responds differently to bile salt.
Serological Reactions
- Pick up the colonies resembling V. cholerae and perform a slide agglutination test using polyvalent and serotype-specific antisera for V. cholerae O1; if negative, perform an agglutination test with O139 antiserum.
- Place two drops of normal saline on a slide side by side and emulsify colonies resembling V. cholerae from a nonselective medium on both.
- Add a drop of polyvalent O1 antisera to one of the suspensions and tilt the slide to and fro. Observe for agglutination within a minute.
- If positive, continue the same procedure with monospecific Ogawa and Inaba antisera. If a positive report is seen with Ogawa antisera, report it as Ogawa. Report it as ‘Inaba’ if a positive result is seen with Inaba antisera, but if positive with both antisera, report it as Hikojima.
- If none of the above shows a positive reaction, perform an agglutination test with O139 antiserum.
Biotyping
- V. cholerae O1 can be further differentiated into two biotypes by the following tests.
- Differentiation of the Classical and El Tor biotypes of V. cholerae serogroup O1.
| Test | Classical | E1 Tor | |
|---|---|---|---|
| (1) | Chicken cell Agglutination (2.5% RBC) | __ | + |
| (2) | Polymyxin B sensitivity (50 IU/disc) | S | R |
Key: S = Sensitive, R = Resistant, + = Positive, – = Negative
**Distilled water motility test**
A simple, useful test to differentiate Vibrio species (Gram-negative motile curved rod) from Aeromonas species (Gram-negative motile rod). Aeromonas grows on MacConkey agar and sometimes on TCBS, producing yellow colonies; both are oxidase positive.
Procedure: Mix a loopful of growth from a nutrient agar subculture in a drop of sterile distilled water on one end of a slide. On the other end, mix a loopful in a drop of peptone water. Cover each with a cover glass. Examine using the 40× objective.
Result: All Vibrio species are immobilized in distilled water but remain motile in peptone water. Aeromonas species remain motile in both distilled water and peptone water.
Immobilization confirmation (from bench practice): if a darting-motile hanging-drop preparation stops moving after adding V. cholerae O1/O139 polyvalent antiserum, O1/O139 is confirmed; if movement persists, consider non-O1 Vibrio or Campylobacter.
Treatment and Management of Cholera
The cornerstone of cholera treatment is rapid fluid and electrolyte replacement, not antibiotics. Up to 80% of cholera cases can be managed successfully with oral rehydration salts (ORS) alone, without hospitalisation.
Rehydration (most important step)
Oral Rehydration Salts (ORS): The WHO/UNICEF ORS formula (sodium, potassium, chloride, citrate, glucose in specific concentrations) corrects both fluid loss and the electrolyte imbalance caused by the hypersecretory mechanism of cholera toxin. ORS is effective for mild to moderate dehydration and should be started immediately — do not wait for laboratory confirmation in a suspected cholera case during an outbreak.
Intravenous fluids: Required for severe dehydration with signs of shock (absent radial pulse, sunken eyes, skin pinch test slow to return). Ringer's lactate is preferred over normal saline because it corrects the metabolic acidosis that accompanies severe cholera. Large volumes may be needed rapidly — 100 mL/kg over 3 hours for adults in severe cases.
Zinc supplementation: Recommended for children under 5 as an adjunct — reduces duration and severity of diarrhoea and helps replenish zinc lost in watery stool.
Antibiotics (adjunct, not primary treatment)
Antibiotics shorten the duration of illness and reduce stool output, decreasing fluid requirements. They are recommended for moderate to severe cases but are not a substitute for rehydration.
- Adults: Single-dose doxycycline (300 mg) — first choice where resistance is not documented
- Children and pregnant women: Azithromycin (single dose or 3-day course) — preferred given tetracycline contraindications
- Note: El Tor biotype V. cholerae O1 has shown resistance to tetracyclines and other antibiotics in some regions, particularly South and Southeast Asia. Local resistance patterns should guide empirical antibiotic choice. Ciprofloxacin is an alternative where doxycycline resistance exists.
Prevention
No specific treatment replaces preventing the next case. Key public health responses:
- Safe water: Chlorination of water sources; boiling water in outbreak settings
- ORS distribution: At community level to reach patients before they reach hospital
- Oral cholera vaccine (OCV): Two doses of killed oral vaccine (Shanchol or mORCVAX) now used in pre-epidemic vaccination campaigns in high-risk areas; WHO recommends OCV as a tool for outbreak response in endemic areas, not a replacement for WASH improvements
How to Remember
Comma-shaped bacterium causing a disease that drains the body like an open tap. The morphology (curved, comma-shaped gram-negative bacilli) and the pathophysiology (massive, uncontrolled secretory diarrhoea) are linked by the same image. The cholera toxin turns on the intestinal secretory pump — cAMP-driven, ATP-consuming, irreversible without treatment — and keeps it running until the patient is either resuscitated or dead from dehydration. The comma shape and the "emptying out" of fluid share the same curve.
Cholera toxin mechanism in one sentence: B binds, A acts. B subunit binds the GM1 ganglioside receptor on the intestinal cell. Once inside, the A subunit ADP-ribosylates the G-protein of adenylate cyclase, locking the enzyme permanently "on." Adenylate cyclase converts ATP to cAMP continuously. High cAMP drives active chloride (and water) secretion into the intestinal lumen — rice-water stool is the physical manifestation of this biochemical cascade. Each step is a one-way ratchet; nothing physiological can turn it off, which is why ORS replacement (not turning off the pump) is the treatment strategy.
TCBS: yellow colony = sucrose fermenter = V. cholerae. On TCBS (Thiosulfate Citrate Bile Salt Sucrose) agar, V. cholerae ferments sucrose and produces yellow colonies. V. parahaemolyticus does not ferment sucrose — its colonies are blue-green. The yellow/blue distinction on TCBS is one of the fastest visual differentiation steps in the lab. Yellow = sucrose fermenting = V. cholerae (and some other sucrose fermenters, hence further confirmation needed).
Oxidase positive + string test positive + O1 or O139 agglutination = confirmed V. cholerae. This three-step sequence is the lab pathway: oxidase tells you it's a Vibrio-type organism (Aeromonas is also oxidase positive — one more reason the string test is needed next), string test narrows further (Aeromonas is string-test negative), and serology confirms which serogroup. No single step is sufficient; the sequence is the confirmation.
El Tor vs. Classical: El Tor is the survivor. The El Tor biotype has virtually replaced Classical biotype worldwide because it survives longer in aquatic environments, colonises asymptomatically more often, and spreads more efficiently. The 7th pandemic (ongoing) is caused entirely by El Tor. Distinguishing them (chicken RBC agglutination positive for El Tor, negative for Classical; polymyxin B resistant El Tor vs. sensitive Classical) is an exam point because it tests the biotype concept — but clinically, El Tor is what you'll encounter.
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Family / Genus | Vibrionaceae / Vibrio |
| Gram stain | Gram-negative curved (comma-shaped) bacilli |
| Motility | Highly motile; darting (to-and-fro) movement; single polar flagellum (monotrichous) |
| Key biochemical properties | Oxidase positive, catalase positive, indole positive, urease negative |
| Selective medium | TCBS agar — V. cholerae produces yellow colonies (sucrose fermenter) |
| Enrichment medium | Alkaline peptone water (APW), pH 8.5 — inoculate pellicle layer only |
| String test result | Positive — bile salt lyses cell wall → DNA release → viscosity → mucoid string |
| String test: Aeromonas | Negative — key clinical differentiation (both oxidase positive, both from diarrheal stool) |
| String test sensitivity/specificity | ~86% / ~70% — screening tool only; requires confirmation by serotyping |
| Serogroups causing epidemics | O1 and O139 only (non-O1/non-O139 cause mild sporadic diarrhoea, not epidemics) |
| O1 biotypes | Classical and El Tor |
| O1 serotypes | Ogawa, Inaba, Hikojima |
| El Tor vs Classical | El Tor: chicken RBC agglutination positive, polymyxin B resistant. Classical: opposite. El Tor = current pandemic biotype |
| Cholera toxin target | GM1 ganglioside on intestinal epithelium |
| Cholera toxin mechanism | B subunit binds GM1 → A subunit ADP-ribosylates G protein → adenylate cyclase locked "on" → ↑cAMP → active ion/water secretion → rice-water stool |
| Primary treatment | Oral Rehydration Salts (ORS) — 80% of cases |
| Severe dehydration IV fluid | Ringer's lactate preferred (corrects metabolic acidosis) |
| Antibiotic (adults) | Single-dose doxycycline 300 mg |
| Antibiotic (children/pregnancy) | Azithromycin |
| Antibiotic resistance concern | El Tor O1: documented tetracycline resistance in some Asian regions; check local sensitivity |
Where Students Get Confused
"Aeromonas and V. cholerae are easily distinguished on standard culture." They are not — this is the primary lab challenge the string test addresses. Both are gram-negative bacilli, both grow on TCBS and MacConkey agar, both are oxidase positive, and both cause acute watery diarrhoea. Without the string test and subsequent serology, a provisional identification of V. cholerae from a diarrheal stool culture is based on very little. The oxidase-positive result is a starting point, not a conclusion.
"Antibiotics are the primary treatment for cholera." They are adjunct treatment. The mechanism of cholera (a toxin-driven secretory process) cannot be reversed by antibiotics — the toxin is already activating adenylate cyclase in cells throughout the intestinal epithelium, and clearing the bacterium from the gut does not immediately stop this process. ORS addresses the actual pathophysiological problem (fluid and electrolyte loss) directly. Antibiotics shorten the illness and reduce stool volume — important benefits — but a patient dying of cholera who receives antibiotics without adequate rehydration will still die of dehydration.
"A positive string test confirms V. cholerae." It does not. Specificity is only 70%, meaning 30% of positive string test results are from organisms other than V. cholerae. A positive string test in combination with yellow TCBS colonies and positive oxidase raises the probability substantially, but serological confirmation with O1/O139 antisera is required for definitive identification.
"APW broth should be shaken or vortexed before plating." It should not. V. cholerae grows as a surface pellicle at the top of alkaline peptone water because it is an aerobe and the alkaline pH enriches selectively for it. Shaking redistributes this pellicle throughout the broth and dilutes the organism's effective concentration at the surface. Always inoculate solid media from the pellicle layer only, without disturbing the broth.
"Non-O1, non-O139 V. cholerae causes cholera epidemics." It does not. Non-O1 and non-O139 serogroups can cause sporadic diarrhoeal illness and other infections, but they lack the cholera toxin gene and cannot cause epidemic cholera. Only O1 and O139 carry the virulence factors responsible for the epidemic and pandemic forms of the disease.
References
- Ojeda Rodriguez, J. A., & Kahwaji, C. I. (2022). Vibrio cholerae infection. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560568/
- Faruque, S. M., Albert, M. J., & Mekalanos, J. J. (1998). Epidemiology, genetics, and ecology of toxigenic Vibrio cholerae. Microbiology and Molecular Biology Reviews, 62(4), 1301–1314. https://doi.org/10.1128/MMBR.62.4.1301-1314.1998
- Yoon, S. H., & Waters, C. M. (2019). Vibrio cholerae. Trends in Microbiology, 27(9), 806–807. https://doi.org/10.1016/j.tim.2019.03.007
- Neogy, K. N., & Mukherji, A. C. (1970). A study of the "string" test in vibrio identification. Bulletin of the World Health Organization, 42(4), 638–640. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2427439/
- Lam, S. Y. (1983). A rapid test for the identification of Vibrio cholerae in stools. Journal of Diarrhoeal Diseases Research, 1(2), 87–89.
- Tamrakar, A. K., Goel, A. K., Kamboj, D. V., & Singh, L. (2006). Surveillance methodology for Vibrio cholerae in environmental samples. International Journal of Environmental Health Research, 16(4), 305–312. https://doi.org/10.1080/09603120600734303
- Grados, P., & Battilana, C. (1994). Detección de portadores de Vibrio cholerae convalecientes mediante el enterotest. Boletín de la Oficina Sanitaria Panamericana, 116(4), 285–289.
Frequently Asked Questions
Why is oral rehydration salts (ORS) the primary treatment for cholera rather than antibiotics?
Why is the string test not used as a standalone confirmatory test for V. cholerae?
Why do V. cholerae strains grow best in alkaline peptone water, and why is only the surface pellicle used for plating?
What is the difference between V. cholerae O1 Classical and El Tor biotypes clinically?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.