MIC vs MBC: What Each Measures and When the Difference Actually Matters
MIC stops bacterial growth; MBC kills it. Learn how MBC is determined from MIC tubes, the MBC/MIC ratio, and the specific clinical scenarios (endocarditis, osteomyelitis, neutropenic sepsis) where the distinction changes treatment.
Minimum Inhibitory Concentration (MIC)
Minimum Inhibitory Concentration (MIC) is the lowest concentration (expressed as mg/L or μg/μL) of an antimicrobial agent that inhibits the visible in-vitro growth of microorganisms. The MIC test determines the antimicrobial activity of a test agent against a specific bacteria. E-test, tube dilution, and agar dilution methods are employed to determine MIC value.
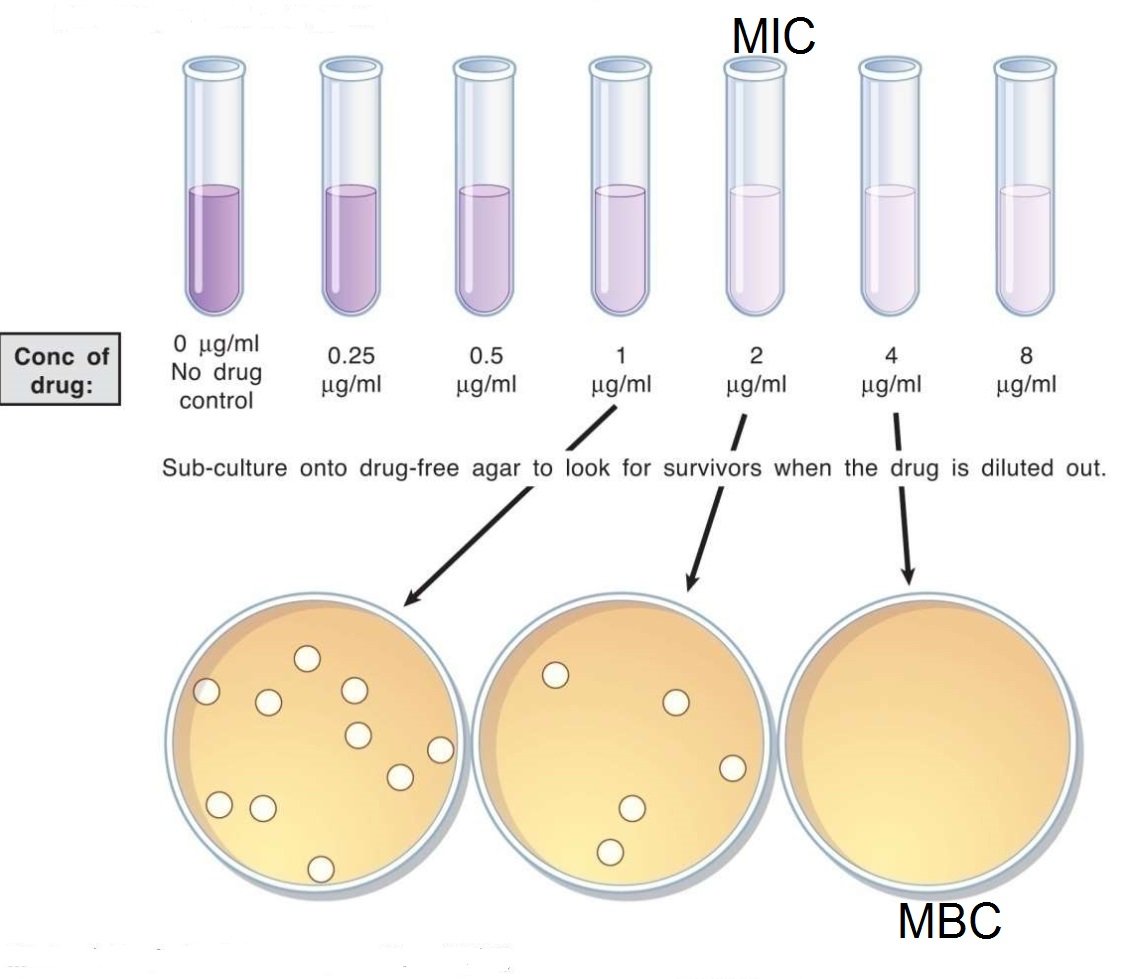 Figure: Minimum Inhibitory Concentration and Mininum Bactericidal Concentration
Figure: Minimum Inhibitory Concentration and Mininum Bactericidal Concentration
While performing the dilution method, the antimicrobial’s lowest concentration (highest dilution) preventing the appearance of turbidity (growth) is considered MIC. At this dilution, the antimicrobial agent is bacteriostatic, i.e. some bacteria may still be alive.
Once the MIC is calculated, it can be compared to known values for a given bacterium and antimicrobial agent and is interpreted as susceptible, susceptible-dose dependent (SSD), intermediate, and resistant. The interpretive criteria for these categories are based on;
- extensive research that correlates MIC with serum achievable levels for each antimicrobial agent,
- particular resistance mechanisms, and
- successful therapeutic outcomes
Relationship between MIC and Zone of Inhibition
The MIC and the zone diameter of inhibition are inversely correlated. The more susceptible the microorganism is to the antimicrobial agent, the lower the MIC and the larger the zone of inhibition. Conversely, the more resistant the microorganism, the higher the MIC and the smaller the zone of inhibition.
MIC is determined only in specific clinical scenarios under the instruction of a Microbiologist, e.g., infective endocarditis. MIC gives valuable information, which will help to customize the treatment to direct only the causative bacterium.
CLSI has recently recommended SDD category reporting instead of “intermediate” when reporting cefepime results for Enterobacteriaceae isolates because there are multiple approved dosing options.
Broth dilution method
The broth (tube) dilution test is the reference method for MIC determination. Serial two-fold dilutions of the antibiotic are inoculated with a standardized bacterial suspension and incubated 18–24 hours; the lowest concentration showing no turbidity is read as the MIC.
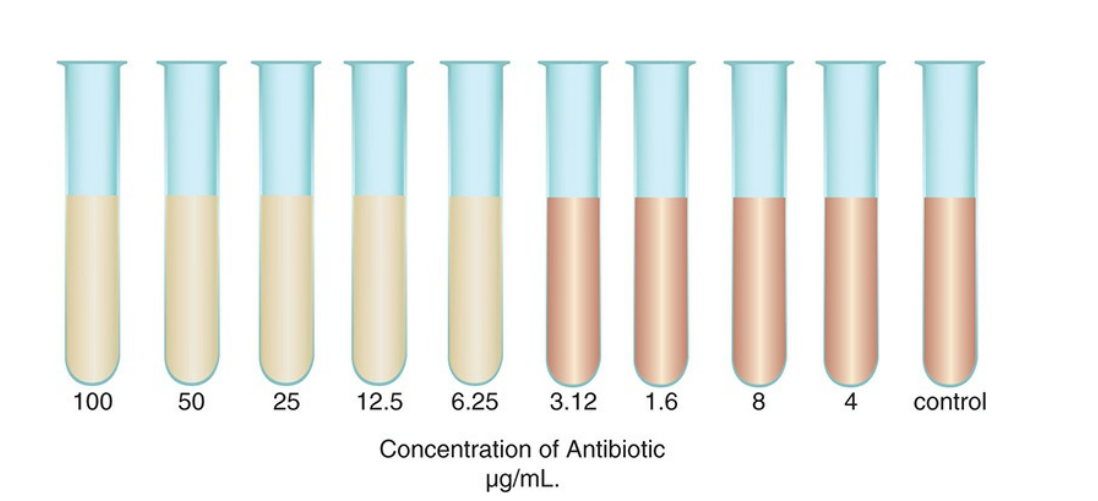 Figure: Broth dilution susceptibility test (MIC 6.25μg/mL)
Figure: Broth dilution susceptibility test (MIC 6.25μg/mL)
In the example above, growth inhibition falls between 6.25 and 3.12 μg/mL — by convention, MIC is read as 6.25 μg/mL, the lowest concentration with no visible growth.
For the full step-by-step procedure — antibiotic stock preparation, McFarland standardization, macrodilution vs. microdilution, and a troubleshooting guide — see Broth Dilution Method for MIC Determination.
Agar dilution method
 Varying concentrations of antimicrobial agents are added to an agar medium, mostly Mueller Hinton Agar (for non-fastidious organisms). Multiple test organisms (at a concentration of 10^4 CFU/mL) can be applied directly or using an inoculum replicating apparatus (steer replicator) on a single agar plate of a particular antibiotic concentration. Results are observed after incubation at 35°C for 18-24 hours.
Varying concentrations of antimicrobial agents are added to an agar medium, mostly Mueller Hinton Agar (for non-fastidious organisms). Multiple test organisms (at a concentration of 10^4 CFU/mL) can be applied directly or using an inoculum replicating apparatus (steer replicator) on a single agar plate of a particular antibiotic concentration. Results are observed after incubation at 35°C for 18-24 hours.
E-test method
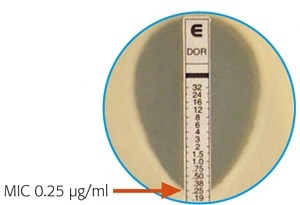 Figure: E-Test showing MIC
Figure: E-Test showing MIC
A plastic strip with a predefined gradient of one antibiotic is applied onto an inoculated agar plate. After 18-24 hours of incubation, a drop-shaped inhibition zone intersects the graded test strip at the inhibitory concentration of the antibiotic.
The intersection of the lower part of the ellipse-shaped growth inhibition area with the test strip indicates the MIC value. Find more about E-test
Automated system for MIC determination
Various commercial automated systems are available for antimicrobial susceptibility testing. Some of the automated system approved by the FDA and currently in use are;
- Vitek 2 system ((bioMérieux))
- MicroScan Walkaway (Beckman Coulter)
- BD Phoenix system (Becton Dickenson Diagnostics)
Reporting MIC results
Laboratories have to report the interpretive category (susceptible, susceptible-dose-dependent, intermediate, or resistant) to the physician with or without MIC value. Only reporting MIC value is not recommended as the physician may fail to interpret it appropriately.
Minimum Bactericidal Concentration (MBC)
Minimum bactericidal concentration (MBC) is the lowest concentration of an antibiotic that kills ≥99.9% of the original bacterial inoculum — not just stops it from growing, but kills it. It's also called the minimum lethal concentration (MLC).
MBC isn't a separate test — it's a second reading taken from the same MIC tubes. From every tube that showed no visible growth in the MIC test, a small volume is subcultured onto antibiotic-free agar and incubated. The MBC is the lowest concentration from which no growth — or fewer than 0.1% of the original inoculum — appears on that subculture plate.
Bacteriostatic or bactericidal? The MBC/MIC ratio
Comparing MBC to MIC tells you which kind of drug you're dealing with for that organism:
- MBC/MIC ≤ 4 → the drug is acting bactericidally against this organism
- MBC/MIC > 4 (sometimes the MBC isn't reached at all within testable concentrations) → the drug is acting bacteriostatically
This isn't a fixed property of the drug class alone — the same antibiotic can behave bactericidally against one organism and bacteriostatically against another, which is exactly why MBC is tested rather than assumed.
Why You'd Actually Order an MBC
Most infections don't need it — a Susceptible/Resistant call from standard AST is enough, because the patient's own immune system clears whatever the drug doesn't kill outright. MBC testing earns its place only when that backup isn't reliable:
- Infective endocarditis — cardiac vegetations are relatively avascular and immune-privileged; a bacteriostatic drug that merely halts growth may not be enough to sterilize the vegetation.
- Osteomyelitis and meningitis — similarly poor antibiotic and immune-cell penetration into bone and CSF.
- Neutropenic or otherwise immunocompromised patients — there's no functional immune system left to finish the job a bacteriostatic drug starts.
The Enterococcal Endocarditis Trap: Ampicillin alone is only bacteriostatic against many enterococci. In a normal infection, the immune system mops up the survivors. But in endocarditis, the vegetation is a relatively immune-privileged space — bacteriostatic activity alone often isn't enough to cure it. This is the textbook reason ampicillin is combined with an aminoglycoside (e.g., gentamicin) for enterococcal endocarditis: the combination achieves a synergistic bactericidal effect that ampicillin alone cannot.
MIC vs MBC at a Glance
| MIC | MBC | |
|---|---|---|
| Measures | Lowest concentration that inhibits visible growth | Lowest concentration that kills ≥99.9% of the original inoculum |
| Endpoint | Bacteriostatic | Bactericidal |
| How it's read | Turbidity (or absence of it) in the dilution series | Subculture of clear tubes onto antibiotic-free agar; colony count |
| Tested routinely? | Yes — basis for standard S/I/R reporting | No — reserved for specific clinical indications |
| When it's ordered | Most bacterial infections, via standard AST | Endocarditis, osteomyelitis, meningitis, neutropenic sepsis |
| Relationship | Determined first | Calculated from the MIC tubes — not a separate test |
Learning & Remembering
MIC = Minimum to Inhibit Colonies (stops growth).
MBC = Minimum to Bust the Colonies (kills them). The difference is "stop vs. kill".
Clinical story: The Enterococcal Endocarditis Trap (above) — why a bacteriostatic drug that works fine for a routine UTI can fail in a heart valve vegetation, and why combination therapy exists.
One sentence that captures it: MIC tells you whether a drug will work; MBC tells you whether it will finish the job — and that difference only changes treatment when the patient's own immune system can't finish the job for it.
Exam facts
| Question | Answer |
|---|---|
| What does MIC measure? | Lowest concentration with no visible growth (bacteriostatic endpoint) |
| What does MBC measure? | Lowest concentration killing ≥99.9% of the original inoculum (bactericidal endpoint) |
| How is MBC determined? | Subculturing clear MIC tubes onto antibiotic-free agar |
| What MBC/MIC ratio defines bactericidal activity? | ≤ 4 |
| Two clinical scenarios where MBC matters | Infective endocarditis, osteomyelitis (also meningitis, neutropenic sepsis) |
| Is MBC part of routine susceptibility reporting? | No |
References and further reading
- CLSI. M07—Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically, 12th ed. Clinical and Laboratory Standards Institute; 2024.
- CLSI. M100—Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute; current annual edition.
- Procop GW, Church DL, Hall GS, Janda WM. Koneman's Color Atlas and Textbook of Diagnostic Microbiology, 7th ed. Wolters Kluwer; 2017.
Frequently Asked Questions
What is the difference between MIC and MBC?
Is a lower MIC always better?
Why isn't MBC tested routinely in clinical labs?
What does an MBC/MIC ratio greater than 4 mean?
Can the same antibiotic be bactericidal against one organism and bacteriostatic against another?
How is MBC determined from the MIC test?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.