Streptococcus agalactiae (GBS): Properties, Pathogenesis, Lab Diagnosis
Streptococcus agalactiae (Group B Strep) virulence factors, neonatal disease patterns, and the CAMP, bacitracin, and hippurate tests for lab diagnosis.
Streptococcus agalactiae, also known as Group B Streptococcus (GBS), is a major cause of neonatal sepsis and meningitis. Other infections caused by Group B Streptococci include postpartum endometritis and bacteremia among pregnant women and pneumonia, endocarditis, skin and soft tissue infections, etc., in adults with underlying diseases.
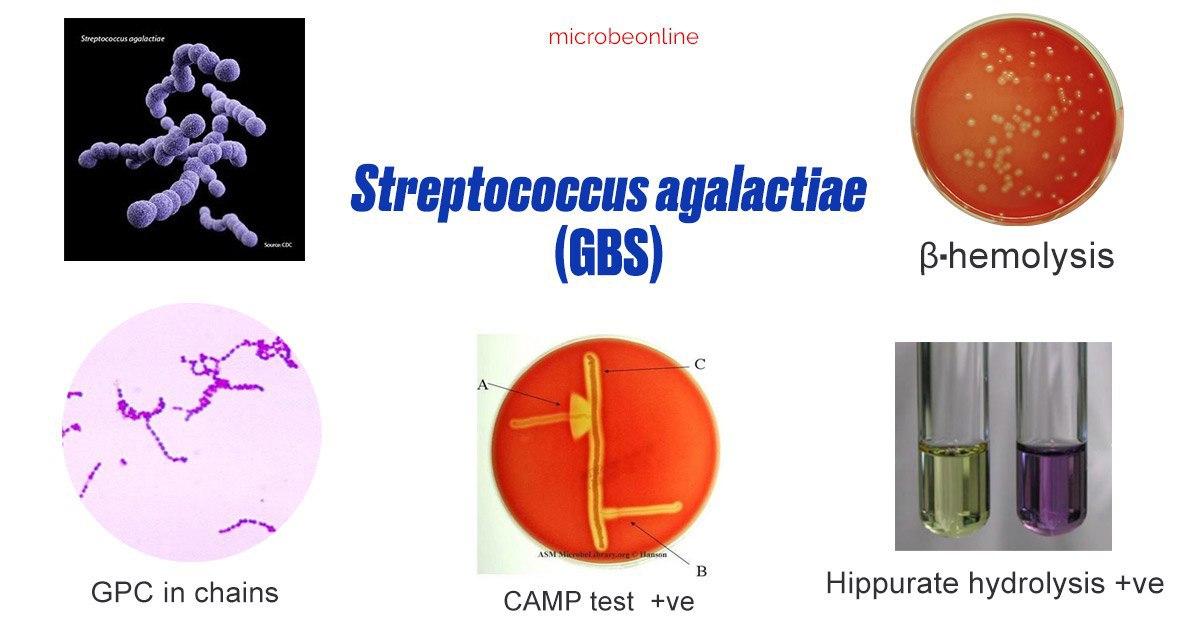 Figure: Properties of Streptococcus agalactiae
Figure: Properties of Streptococcus agalactiae
General Properties
- Gram-positive cocci in pairs and chains
- Capsulated: S. agalactiae has 10 distinct serotypes including nine capsular serotypes; Ia, Ib, and II to VIII and one nontypeable strain (serotype IX)
- Facultative anaerobic
- Non-sporing
Why these swabs get collected in the first place
Rectovaginal GBS colonization is found in 10-37% of pregnant women, and on its own it's harmless to the mother. The reason labs routinely process vaginal/rectal swabs in late pregnancy at all is a specific prevention strategy: universal antenatal screening at 35-37 weeks identifies carriers so that intrapartum antibiotic prophylaxis can be given during labor.
This has measurably reduced early-onset neonatal GBS disease, though it has little effect on late-onset disease, since early-onset disease comes from intrapartum exposure while late-onset disease is often acquired after birth from other sources.
Pathogenesis
Virulence Factors of *Streptococcus agalactiae*
- Polysaccharide capsular antigens: Inhibits activation of the alternative complement cascade and prevents phagocytosis
- C5a peptidase: C5a peptidase produced by the streptococci cleave complement component C5a and interfere with C5a-mediated neutrophil chemotaxis. This peptidase also binds to fibronectin and serves as a bacterial adhesin and invasin
- Beta-hemolysin/cytolysin: Pore-forming hemolysin that is able to lyse pulmonary alveolar epithelial and endothelial cells and plays a role in neonatal lung infection and subsequent sepsis.
- Lipoteichoic acid: Participate in facilitating adherence as the first step in infection.
- Cell surface proteins:
C antigen: May mediate internalization of organisms within human cervical epithelial cells following attachment. Protect organisms from intracellular killing following phagocytosis
Cell surface penicillin-binding protein (PBP 1a): Enables streptococcal cells to resist intracellular killing by phagocytic cells.
Hyaluronic acid lyase: This may act to spread infection by the breakdown of hyaluronic acid in the extracellular matrix, and may act on the hyaluronic acid present in concentrations in placental tissues, fetal tissues, and amniotic fluids.
Disease & Clinical Presentation of *Streptococcus agalactiae*
Rectovaginal colonization of Streptococcus agalactiae is found in 10% to 37% of pregnant women which may be transient, intermittent, or persistent. The presence of group B streptococci in the female genital tract at the time of birth can lead to infection of the neonate. Streptococcus agalactiae is a predominant cause of acute meningitis in neonates.
Predisposing factors for neonatal infection with S. agalactiae are;
- rupture of membranes more than 18 hours before delivery
- labor prior to 37 weeks (infant is premature)
- absence of maternal antibody, and
- heavy colonization of the genital tract by S. agalactiae
Neonatal disease with group B streptococci follows two patterns, termed early-onset disease and late-onset disease.
- Early-onset disease: is associated with in utero or perinatal (during passage through a birth canal that is colonized with group B streptococci) organism acquisition. Onset of disease occurs within 12 hours to 5 days after birth. The disease spectrum includes bacteremia, pneumonia, meningitis, septic shock, and neutropenia.
- Late-onset-disease: acquired from the birth canal of colonized mothers or from postnatal acquisition from the mother, other caregivers, or nosocomially Onset of disease occurs within 7 days to 3 months (average 3 to 4 weeks) after birth. Bacteremia is the predominant clinical presentation, and about 25% of these infants also develop group B streptococcal meningitis.
Laboratory diagnosis
Specimen Collection
- Detection of carriers (i.e. perinatal detection of GBS): One vaginal and one rectal swab, collected and sent in Amies of Stuart’s medium without charcoal, within 4 hours of sample collection.
- Diagnosis of cases: CSF, blood and other samples (depending on clinical presentations).
Enrichment broth: Todd-Hewitt broth with antimicrobials (gentamicin, nalidixic acid, or colistin) is used to suppress the growth of vaginal flora and allow the growth of S. agalactiae.
The presence of Gram-positive cocci in short chains in the CSF of neonates is presumptively identified as Streptococcus agalactiae.
A: Culture
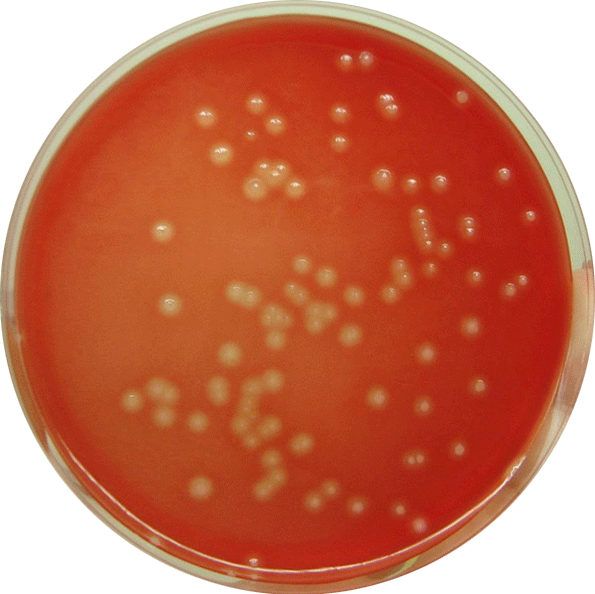 Figure: Beta-hemolytic colonies of S. agalactiae (Image source: wikimedia.org)
Figure: Beta-hemolytic colonies of S. agalactiae (Image source: wikimedia.org)
Culture media: Blood Agar
Isolation of Streptococcus agalactiae from a genital site of a woman at term should be communicated as an urgent report.
Colony characteristics in blood agar: Colonies are larger than group A streptococci; translucent to opaque; flat, glossy; narrow zone of beta-hemolysis. Some strains are non-hemolytic.
Test for the identification of suspected GBS (S. agalactiae) colonies
- Catalase test: When we observe beta-hemoytic colonies in blood agar, performing catalase test, helps to differentiate between beta-hemolytic streptococci from staphylococci. Staphylococci are catalase-positive whereas streptococci are catalase-negative.
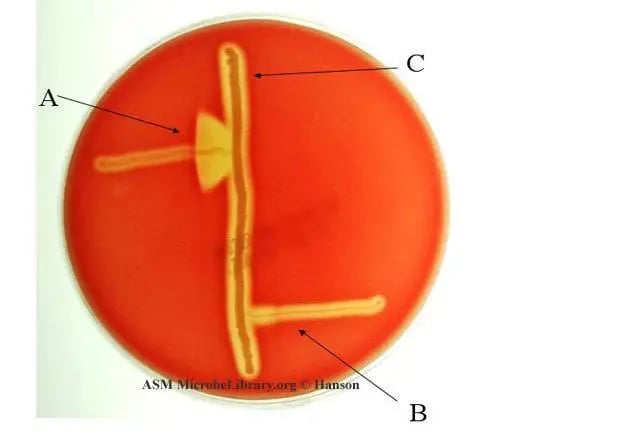 Figure: CAMP test: A. Streptococcus agalactiae (positive) B. Streptococcus pyogenes (negative) Image source: ASM
Figure: CAMP test: A. Streptococcus agalactiae (positive) B. Streptococcus pyogenes (negative) Image source: ASM
CAMP test: CAMP test may be employed for presumptive identification of catalase-negative, beta-hemolytic streptococci. S. agalactiae gives enhanced arrowhead beta-hemolysis at the juncture of S.agalactiae and S. aureus streaks; when streaked at perpendicular with beta-hemolytic S. aureus in blood agar.
Bacitracin resistant: Bacitracin sensitivity test helps to differentiate between two beta-hemolytic streptococci; Streptococcus pyogenes (GAS)and Streptococcus agalactiae(GBS). GAS is bacitracin sensitive whereas GBS is bacitracin resistant.
How to Remember Properties of Group B Streptococci?
GAS and GBS are taught back to back specifically because they're a contrast pair, and the bench results flip almost completely between them:
| GAS (S. pyogenes) | GBS (S. agalactiae) | |
|---|---|---|
| Bacitracin | Sensitive | Resistant |
| CAMP test | Negative | Positive |
| PYR | Positive | Negative |
If you remember GAS's profile from the S. pyogenes article, GBS is simply the mirror image on all three. The one test that doesn't flip is hippurate hydrolysis, GBS is positive, and that's the one place where GBS stands alone rather than opposing GAS, since most other beta-hemolytic streptococci are hippurate-negative too.
The CAMP test itself is worth understanding mechanistically rather than memorizing as a color change: the "arrowhead" enhanced hemolysis only appears where the GBS streak meets the S. aureus streak, because the CAMP factor GBS produces acts synergistically with staphylococcal beta-hemolysin, neither organism alone produces that pattern, it's the interaction at the junction that does.
One more connection worth making explicitly: GBS's C5a peptidase is the same enzyme family as the Anti-C5a peptidase you already met in S. pyogenes, both cleave the same complement fragment to blind neutrophil chemotaxis. Different organism, same trick.
Biochemical Tests
Following biochemical tests are useful for the identification of S. agalactiae.
| Name of the test | S. agalactiae | Notes |
|---|---|---|
| Catalase test | Negative | Streptococci are catalase-negative, whereas staphylococci are catalase positive. |
| Hemolysis | β-hemolysis | |
| CAMP test | Positive (enhanced arrowhead hemolysis) | Presumptive identification of Group B beta-hemolytic streptococci |
| Pyrrolidonyl-β-naphthylamide (PYR) test | Negative | Streptococcus pyogenes is PYR positive. |
| Bacitracin sensitivity test | Resistant | S. pyogenes , the other β-hemolytic streptococci are bacitracin sensitive. |
| Hippurate hydrolysis test | Positive | Differentiation of β-hemolytic Streptococcus agalactiae from other β-hemolytic streptococci. |
B: Other tests
- Latex agglutination: Several commercial antigen detection kits are available for diagnosis of neonatal sepsis and meningitis using serum CSF or urine as a sample.
- DNA probe, nucleic acid amplification test (NAAT), or other molecular testing are also available for the identification of S. agalactiae.
Where students actually get confused
- Colonization is not infection. Most colonized pregnant women and their newborns never develop disease. The lab result "GBS positive" on a screening swab means carrier status, not a diagnosis requiring treatment of the mother, it changes intrapartum management, not maternal treatment.
- Catalase-negative and beta-hemolytic alone doesn't confirm GBS. S. pyogenes fits that too. CAMP, bacitracin, and hippurate are what separate them.
- Early-onset vs late-onset is about source, not just timing. Early-onset (within 5 days) comes from intrapartum exposure during passage through a colonized birth canal. Late-onset (up to 3 months) can come from the same source or from postnatal acquisition, including nosocomial spread, this distinction matters for outbreak investigation, not just for staging the case.
Key exam facts in one table
| Feature | S. agalactiae (GBS) | Memory hook |
|---|---|---|
| Catalase | Negative | Rules out Staph only |
| Hemolysis | Beta (narrow zone) | Narrower than GAS |
| CAMP test | Positive | Opposite of GAS |
| Bacitracin | Resistant | Opposite of GAS |
| PYR | Negative | Opposite of GAS |
| Hippurate | Positive | The one that doesn't flip |
| Main virulence factor | Polysaccharide capsule | Same anti-phagocytic job as in S. pneumoniae |
| Screening window | 35-37 weeks | Determines intrapartum prophylaxis |
| Early-onset disease | Within 5 days | Intrapartum source |
| Late-onset disease | Up to 3 months | Birth canal or postnatal source |
Self-check questions
- Why does universal GBS screening happen at 35-37 weeks rather than earlier in pregnancy?
- What's the mechanistic reason the CAMP test produces enhanced hemolysis specifically at the junction of the two streaks?
- A throat-style panel comes back catalase-negative, beta-hemolytic, CAMP-positive, bacitracin-resistant, PYR-negative. Which organism is this, and how do you know it's not S. pyogenes?
- An infant develops sepsis at 6 weeks of age. Is this early-onset or late-onset GBS disease, and what does that imply about the likely source?
- GBS and GAS both produce a C5a peptidase. What does this enzyme block, and why is that useful to both organisms despite their very different disease patterns?
References and further readings
- Procop, G. W., & Koneman, E. W. (2016). Koneman's Color Atlas and Textbook of Diagnostic Microbiology (7th International ed.). Lippincott Williams and Wilkins.
- Teatero, S., Ferrieri, P., Martin, I., Demczuk, W., McGeer, A., & Fittipaldi, N. (2017). Serotype distribution, population structure, and antimicrobial resistance of group B Streptococcus strains recovered from colonized pregnant women. Journal of Clinical Microbiology, 55(2), 412-422. https://doi.org/10.1128/JCM.01615-16
- Tille, P. (2017). Bailey & Scott's Diagnostic Microbiology (14th ed.). Mosby. https://amzn.to/2IgqSJU
- Raabe, V. N., & Shane, A. L. (2019). Group B Streptococcus (Streptococcus agalactiae). Microbiology Spectrum, 7(2). https://doi.org/10.1128/microbiolspec.GPP3-0007-2018
Frequently Asked Questions
Does testing positive for GBS during pregnancy mean the baby will get sick?
What is the difference between early-onset and late-onset GBS disease in newborns?
Why is the CAMP test result different for GBS and GAS?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.