CSF Sample: Collection, Processing, Staining, and Culture
CSF Sample: Collection, Processing, Staining, and Culture
 Figure: Skull Meningitis
Figure: Skull Meningitis
Meningitis is an inflammation of the membranes covering the brain and spinal cord known as the meninges. The most common etiologic agents of acute meningitis are enteroviruses (primarily echoviruses and coxsackieviruses) and bacteria (Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae), etc. Organisms expected to cause chronic meningitis (symptoms ≥4 weeks) include Mycobacterium tuberculosis, fungi, and spirochetes.
Viral infections usually get better without treatment but bacterial infection of the meninges is very serious and is a major cause of deaths and disability worldwide. Patients’ age and other factors (i.e, immune status, post neurosurgery, trauma) are associated with specific bacterial pathogens.
Common Causes of Meningitis
Common causes of bacterial meningitis vary by age group:
Age GroupCausesNewbornsGroup B Streptococcus (Streptococcus agalactiae), Escherichia coli, Listeria monocytogenesInfants and ChildrenStreptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae type b (Hib) , Group B StreptococcusAdolescents and Young AdultsNeisseria meningitidis, Streptococcus pneumoniaeOlder AdultsStreptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae type b (Hib), Group B Streptococcus, Listeria monocytogenes
CSF Collection
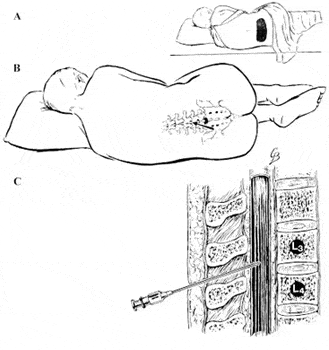 Figure: Collection of cerebrospinal fluid (CSF) by lumbar puncture
Figure: Collection of cerebrospinal fluid (CSF) by lumbar puncture
Whenever possible, collect CSF (1 mL minimum, 3-4 mL if possible)**prior to initiating antimicrobial therapy. CSF is generally obtained by lumbar spinal puncture at the L4-L5 level or L3 and L4and is collected usually in three separate tubes:
- Tube 1: For cell count and differential stains
- Tube 2: For Gram’s stain and culture (A minimum of 0.5–1 mL of CSF should be sent to the microbiology laboratory in a sterile container for bacterial testing. )
- Tube 3: For protein and glucose or for special studies such as VDRL, cryptococcal antigen, or cytology depending on the clinical situation.
- When the specimen volume is less than required for multiple test requests, prioritization of testing must be provided to the laboratory.
- Two to four blood cultures should also be obtained if bacterial meningitis is suspected.
- Inform the microbiology laboratory if unusual organisms are possible (such as Nocardia, Fungi, Mycobacteria, etc.) for which special procedures are necessary.
- Do not refrigerate cerebrospinal fluid.
- Attempt to collect as much sample as possible (approximately 5–10 ml of CSF should be collected) for multiple studies (minimum recommended is 1 ml); prioritize multiple test requests on small volume samples.
Note:
When CSF is collected into five calibrated sterile tubes,
- The first tube is sent to biochemistry (for total protein, glucose, immunoglobulin index, and/or oligoclonal banding),
- 2nd to microbiology for bacterial culture and sensitivity, viral culture, fungal culture, or detection of cryptococcal antigen.
- The third tube is also sent to microbiology for AFB culture and special stain.
- The fourth tube is sent to hematology for cell count, flow cytometry, and cytology.
- The fifth tube is used for the detection of special pathogens such as Acanthamoeba, West Nile virus, viral PCR, anaerobic culture (including gram stain), and Creutzfeldt-Jakob disease (14-3-3 protein).
If only one tube of CSF is available, it should be sent to the microbiology laboratory. If CSF sample is collected in multiple tubes, the first tube collected (which could contain contaminating blood from the lumbar puncture) should not be the tube sent to the microbiology laboratory.
CSF volume & Production in Human
Total CSF in adult85-125 mL Total CSF in neonate10-60 mL Normal rate of CSF production in Adult20 mL/Hour
Processing of CSF Sample
CSF should never be refrigerated prior to culturing because fastidious organisms may not survive lowered temperatures. If bacterial culture cannot be set up immediately, store the CSF at 35°C to maintain body temperature or leave it at room temperature.
CSF from a patient suspected of meningitis is an emergency specimen that requires immediate processing to determine the etiologic agent. Common etiological agents of bacterial agents; N. meningitidis, S. pneumoniae, and H. influenzae are fastidious and fragile bacteria. For successful isolation of these bacteria, CSF must be cultured within one hour of collection or inoculated into Trans-Isolate (T-I) medium for transport to the laboratory if processing within one hour is not feasible.
A delay in examining CSF:
- Reduces the chances of isolating pathogens
- Lowers cell count due to WBCs being lysed
- Falsely shows low glucose value due to glycolysis
Laboratory Tests
Biochemical Testing
In the case of acute bacterial meningitis, CSF analysis shows
Leukocytes/mm 3Predominant Cell TypeProteinGlucoseClinical Setting0-5None15-50 mg/dL45-100 mg/dLNormal2-2000 (mean of 80)MononuclearSlightly elevated (50-100 mg/dL) or normalNormalViral meningitis5-20,000 (mean of 800)PMNElevated (>100 mg/dL)Low (<45 mg/dL), but may be normal early in the course of the diseaseAcute Bacterial Meningitis5-2000 (mean of 100)MononuclearElevated (>50mg/dL)Normal or often low (>45 mg/dL)Meningitis caused by tuberculosis or fungi
- Presence of a large number of inflammatory cells (>1000/mm3) primarily polymorphonuclear neutrophils,
- Decreased glucose level relative to the serum glucose level (the normal ratio of CSF to serum glucose is approximately 0.6) and
- An increased protein concentration.
Interpretation of Biochemical Analysis of CSF Fluid
Microscopy and Staining
The number of organisms in the CSF can be as low as 103 CFU/ml so CSF Gram stains should be prepared after cytocentrifugation. Report positive Gram stain results immediately to clinicians, usually within one hour of receipt.
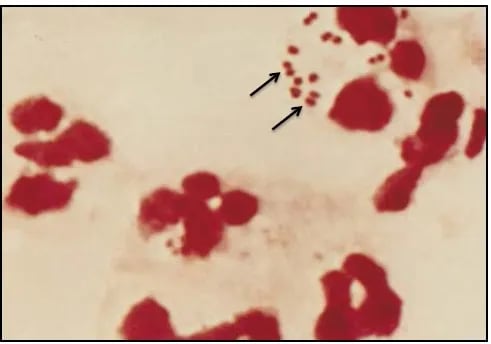 Figure: Gram stain of N. meningitidis in CSF with associated PMNs
Figure: Gram stain of N. meningitidis in CSF with associated PMNs
- N. meningitidis may occur intracellularly or extracellularly in PMN leukocytes and will appear as gram-negative, coffee-bean-shaped diplococci.
- S. pneumoniae may occur intracellularly or extracellularly and will appear as gram-positive, lanceolate diplococci, sometimes occurring in short chains.
- H. influenzae are small, pleomorphic gram-negative rods or coccobacilli with random arrangements.
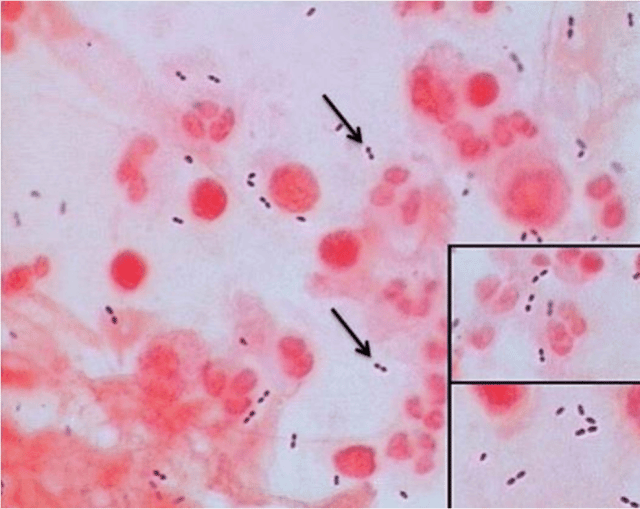 Figure: Streptococcus pneuemoniae: Gram positive diplococci
Figure: Streptococcus pneuemoniae: Gram positive diplococci
If cryptococcal meningitis is suspected, India ink preparation should be done.
Culture and Sensitivity
As CSF is a sterile body fluid collected by transcutaneous aspiration, all organisms recovered from the culture are potential pathogens. Concentration for culture is unnecessary since the plate inoculum is sufficient to detect the usually low numbers of organisms.
Growth on Chocolate Agar plateGrowth on Blood Agar plateGram StainingPresumptive ID++Gram-negative diplococciN.meningitidis++ (α-hemolysis)Gram-positive diplococciS. pneumoniae+ (perform a test for X and V factor requirements)– (negative)Gram-negative pleomorphic coccobacilliH. influenzae
Aerobic bacteria mostly cause bacterial meningitis though anaerobes may be present in CSF in a meningeal abscess or a similar infectious process adjacent to the meninges. Following media are routinely used in the diagnostic laboratory for the isolation of common bacterial agents of meningitis;
Chocolate Agar
On chocolate agar plate, H. influenzae appear as large colorless to grey, opaque colonies with no discoloration of the surrounding medium.
 Figure: N. meningitidis on blood agar plate
Figure: N. meningitidis on blood agar plate
- Overnight growth of N. meningitidis on blood agar plate appears as round, moist, glistening and convex colonies.
- S. pneumoniae appear as small greyish mucoid (watery) colonies with a greenish zone of alpha-hemolysis surrounding them on the blood agar plate.
MacConkey Agar
Summary of identification scheme (Gram staining and culture)
Antigen-Antibody Reactions
- Antigen Testing: Cryptococcal antigen latex agglutination test is the preferred method in the suspected cases of cryptococcal meningitis. Bacterial antigen testing on CSF is not recommended.
- Serology: Serologic diagnosis is based on CSF to serum antibody index, 4- fold rise in acute to convalescent immunoglobulin G (IgG) titer, or a single positive immunoglobulin M (IgM). Submission of acute (3–10 days after onset of symptoms) and convalescent (2–3 weeks after acute) serum samples is recommended.
Molecular Diagnosis
Nucleic acid amplification tests (NAAT)****are now available for most pathogens in developed countries but such facilities may not be available in developing countries or resource-poor settings. Molecular testing has replaced viral culture for the diagnosis of enteroviral meningitis.
Reference and further reading
- CDC meningitis home page
- Laboratory Methods for the Diagnosis of Meningitis, WHO Manual, 2nd Edition

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.