Treponema pallidum: Properties, Pathogenesis, and Disease
Treponema pallidum: Properties, Pathogenesis, and Disease
Treponema (trepos meaning turn and nema meaning thread) pallidum is a member of the spirochete family having a characterized distinct helical shape. It is the causative agent of syphilis, an infectious venereal disease in humans.
Treponema pallidum was first discovered in 1905 by Fritz Schaudinn and Erich Hoffmann in chancres and inguinal lymph nodes of the patients.
Properties
- Morphology: Treponemes are extremely thin and delicate with tapering ends. Treponemes cannot be visualized by light microscope but can be seen under dark ground or phase contrast microscope.
- Staining: Treponemes do not take ordinary stain but can be stained by fluorescence staining and silver impregnation methods.
- Size: 6-14μm * 0.2 μm
- Spirals: They are flexible, spirally coiled around the long axis; possess 6-14 spirals spaced at intervals of 1 μm with amplitude of 1-1.5 μm
- Motility: actively motile exhibiting flexion extension, translatory, and corkscrew motility. They have a typical tendency to bend at right angle at the midpoint.
- Endoflagella
About 3-4 flagella are present in periplasmic space. Flagella provide motility to bacteria thus helping in tissue invasion and dissemination. Highly antigenic, thus stimulating a strong early antibody response.
- Anaerobic/microaerophilic (i.e. requires a very low concentration of oxygen)
- Extremely delicate organisms (heat, drying, disinfectants)
- Pathogenic treponemes are obligate intra-cellular parasites (i.e. they cannot be grown in artificial culture media but are maintained by subcultures in susceptible animals such as rabbit testes).
- Humans are the only source of treponemal infection; there are no known nonhuman reservoirs.
Classification
Classification of the pathogenic treponemes is based primarily upon the clinical manifestations of the respective diseases they cause. Four members are human pathogens
- Treponema pallidum subsp pallidum that causes venereal syphilis;
- T. pallidum subsp pertenue that causes yaws;
- T. pallidum subsp endemicum that causes endemic syphilis; and
- T. carateum that causes pinta.
Besides, there are few commensal treponemes found in the mouth and GI tract of humans and few animal treponemes found in rabbits.
Pathogenesis
Transmission
Infection begins when T. pallidum penetrates the host, usually through intact or abraded mucous membranes. Venereal syphilis is transmitted by sexual contact; other diseases are transmitted by close non-venereal contact.
Acquired Syphilis
- Treponema pallidum enters via body fluids
Cuts/breaks in skin or mucous membranes (external genitalia) Mouth
- Sexual contact: abrasions during sexual contact/direct contact with a syphilis chancre increases risk of transmission.
- Contaminated needles or blood transfusion (rare)
- Direct contact with a skin lesion
Congenital Syphilis
T. pallidum infects the fetus in the uterus **(transplacental)**or when exiting through birth canal of an infected mother.
Pathogenesis Mechanism
- Within few hours of entry via skin or mucosa, the organism enters the lymphatics and blood to produce systemic infection and metastatic foci.
- Incubation period is variable (9-90 days; median 21 days) and is inversely proportional to the number of organisms (average inoculum size is 500-1000) inoculated. During the incubation period, the bacteria not only invade the lymphatics but also disseminate to the bloodstream where it adheres to the surface proteins of endothelial cells. After an incubation of 2-4 weeks, the clinical sign and symptoms appear.
- Approximately, 30% of persons who have sexual exposure with an infected partner develop syphilis.
- Clinically, patients suffering from syphilis pass through four stages if left **untreated, primary, secondary, latent and tertiary (or late)**stages.
Virulence factors
Potential virulence factors which account for T. pallidum‘s ability to cause disease include
- Endoflagella: They provide motility to the bacteria, thus helping in tissue invasion and dissemination. They are also highly antigenic, stimulating a strong early antibody response.
- Outer membrane proteins promote adherence to host cells.
- Hyaluronidase (an enzyme produced by virulent treponemes) facilitate perivascular infiltration
- Coating with host cell fibronectin protects against phagocytosis
Tissue destruction primarily results from host’s immune response to infection.
Antigens
T. Pallidum is antigenically complex and poorly understood. Based on the type of antibody response, three antigens are identified;
- Group-specific antigen: Protein antigen present in all treponemes (pathogenic and nonpathogenic). Antibodies to this antigen can be detected in sera of syphilitic patients by using antigens of Reiter treponemes.
- Species-specific antigen: It appears to be polysaccharide in nature. Treponemal antibodies induced by this antigen in a syphilitic patient can be detected by using specific T. pallidum antigens.
- Non-specific antigen: It is a heterophile antigen. Antibody against this antigen is detected by using beef heart antigen by various non-treponemal tests.
Clinical Manifestations
Clinically, syphilis can be of two types acquired syphilis (in adults by sexual contact excluding neurosyphilis) and congenital syphilis (acquired from mother to child). Acquired syphilis: On the basis of disease progression, acquired syphilis has been further divided into stages.
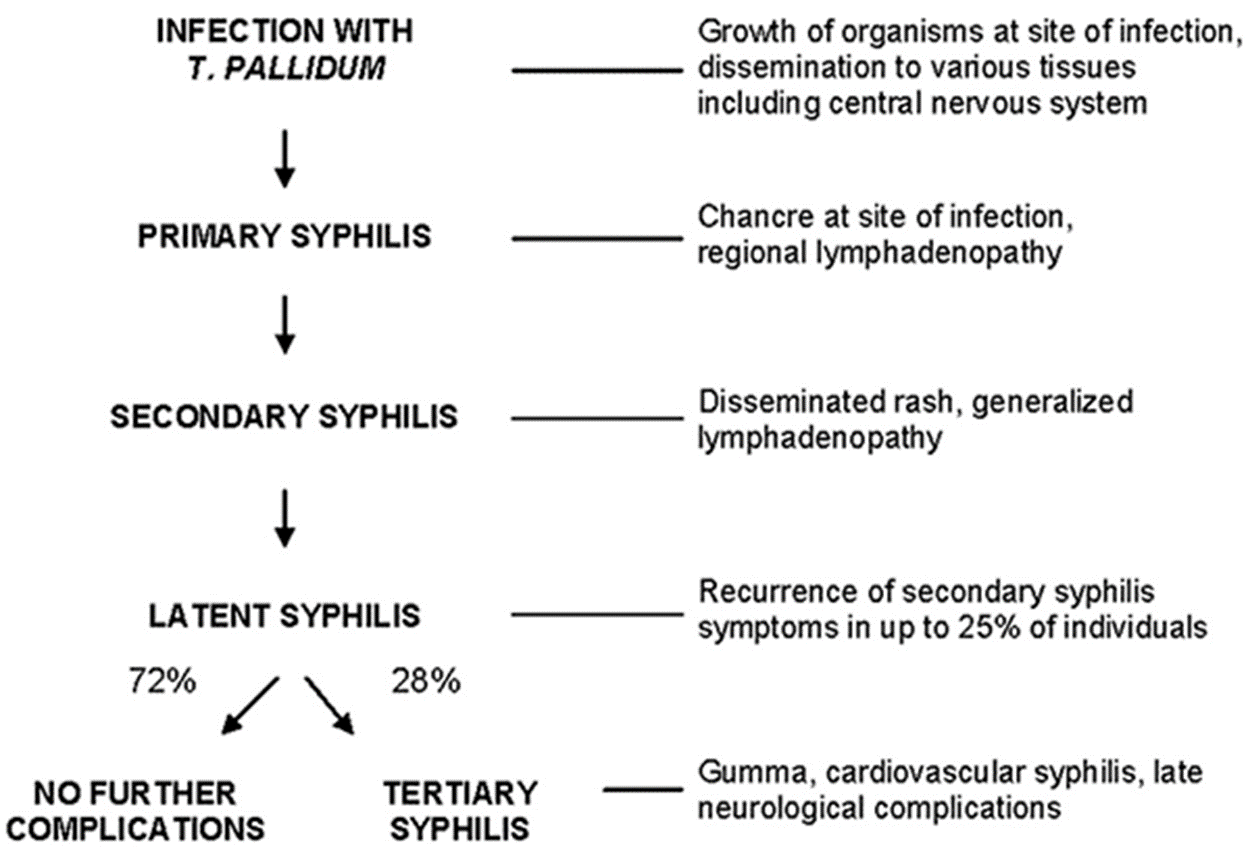 Figure: Stages of Syphilis
Figure: Stages of Syphilis
Primary syphilis
- Primary syphilis is the stage of infection that occurs in 2-4 weeks after infection and usually begins as a single painless papule that rapidly becomes ulcerated, hard, and indurated (popularly called hard chancre). It is covered by thick exudate, every rick in spirochetes.
- Chancre appears on external genital corona of the penis, labia, vaginal wall cervix, perianal area, mouth, anal canal. Serological tests are positive in 80% individuals at this stage.
- Regional lymphadenopathy appears within 1 week of onset of skin lesions. Lymph nodes are painless firm, non-suppurative, and often bilateral.
- The chancre generally heals within 4-6 weeks (range 2-12 weeks), but lymphadenopathy may persist for months.
- If acquired by non-veneral mode, then the primary syphilis is presented as follows:
If transmitted by direct contact: The primary chancre is extra genital, usually on the fingers. If transmitted by **blood transfusion-**the primary chancre does not occur.
In some individuals, the appearance of primary chancres does not fit the classic description. Nonindurated lesions with irregular borders, multiple and/or painful lesions, especially in the anal area are seen in HIV-infected individuals. The untreated lesion or lesions usually heal spontaneously in 2 to 8 weeks.
Secondary syphilis
Secondary syphilis usually develops 4-8 weeks after the healing of primary lesions. In secondary syphilis, skin and mucous membranes are primarily affected. During this stage, widespread dissemination of the infection to various parts of the body occurs.
In most cases, the widely disseminated maculopapular rash appears at palms and soles. Symptoms such as fever, malaise, anorexia, weight loss, pharyngitis, laryngitis, and/or arthralgias are also common. Other clinical manifestations include lesions in the mouth and oral cavity, lymphadenopathy, condyloma latum, glomerulonephritis, nephritic syndrome, hepatitis, arthritis, osteitis, and periosteitis. Temporary alopecia may occur. Nails become brittle and pitted.
Condylomata lata represent one of the manifestations of secondary syphilis in which beningn and painless mucocutaneous papules are formed in warm moist intertriginous areas which later coalesce to form large pink to grey lesions
The manifestations of secondary syphilis are transient because most patients at this stage develop immune responses and the disease gets cured. In 13-15% of cases, the disease progress to the latent stage and finally to the tertiary stage.
Latent syphilis
The period between secondary and tertiary syphilis, termed latency, can last for many years. After several weeks, secondary lesions disappear and disease becomes latent. Latent syphilis is divided into two stages, based upon an approximation of the time of infection.
- Early latent syphilis: occurs within 1st year of infection
- Late latent syphilis: occurs after one year of infection
Disease is not infectious at this stage, except for transmission from mother to fetus (congenital syphilis). Positive serological tests for syphilis and normal CSF findings.
Possible fates of latent syphilis:
- Persistent lifelong infection (common)
- Development of late syphilis (rare)
- Spontaneous cure
Tertiary or Late Syphilis
Develops after many years (decades) in persons with untreated secondary syphilis.
Tertiary syphilis develops in up to 35% of untreated secondary syphilis patients after 10-25 years of initial infection. Late syphilis can be categorized into neurosyphilis, cardiovascular syphilis, and granulomatous syphilis.
- Appearance of degenerative granulomatous lesions called GUMMAS in skin, bone and nervous system.
- Approx 20% patients may develop neurosyphilis or cardiovascular syphilis.
Cardiovascular syphils and granulomatus syphilis are uncommon in the antibiotic era due to the frequent exposure to antibiotics while neurosyphilis is the most common manifestation of tertiary/late syphilis because of the generally poor penetration of antibiotics into the CNS.
- Neurosyphilis may manifest as meningitis, meningovascular syphilis, general paresis of insane (paralytic dementia) and tabes dorsalis.
- Cardiovascular syphilis is characterized by aneurysm of ascending aorta and aortic regurgitation
Congenital syphilis
T. pallidum can be transmitted from the bloodstream of the infected woman to the developing fetus at any time during pregnancy, although the risk is much higher during early maternal syphilis than during later stages. Neonates may also be infected during passage through the infected birth canal at delivery. Affected infants typically have low weight at birth, pulmonary hemorrhage, secondary bacterial infection, and severe hepatitis.
Congenital syphilis is divided into stages: early manifestations appearing in the first two years of life, late manifestations appearing after two years, and residual stigmata.
- Early manifestations are infectious and resemble severe symptoms of adult secondary syphilis; they usually become apparent 2 to 10 weeks after delivery. Symptoms include persistent rhinitis with a whitish discharge that is sometimes tinged with blood, accompanied by desquamation of the skin of palms and soles.
- Late manifestations of congenital syphilis occur between the 5-25 years of ages interstitial keratitis may cause damage to the cornea and iris, and eighth-nerve deafness may be apparent. Hutchinson’s teeth, peg-shaped notched upper incisors, is another characteristic late stigma of congenital syphilis.
References and Further Readings
- Medical Microbiology, 4th edition. Editor: Samuel Baron
- Fantry L E., Tramont E C “Treponema Pallidum (Syphilis)”
- Blenden D. C. “The Application of A Silver Impregnation Stain for Treponema Pallidum” The Journal of Investigative Dermatology,1965, Vol. 45, No. 1

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.