Pneumocystis jirovecii: Properties, Pathogenesis, Lab Diagnosis
Pneumocystis jirovecii: Properties, Pathogenesis, Lab Diagnosis
Pneumocystis jirovecii (previously known as Pneumocystis carinii) is an opportunistic atypical fungal pathogen that does not respond to conventional anti-fungal agents*. P. jirovecii is an organism of low virulence that spreads through the air and causes serious and often fatal pneumonia called Pneumocystis jirovecii pneumonia (PJP) in immunocompromised patients, particularly in AIDS patients.
*The most common form of treatment is trimethoprim/sulfamethoxazole (co-trimoxazole). This medicine is given by mouth or through a vein for 3 weeks.
Pneumocystis jirovecii is common in the environment and does not cause illness in healthy people. The fungus can live in their lungs without causing symptoms. Asymptomatic infection is also quite common. Serologic evidence suggests that most children are exposed to this organism by age 3 to 4.
Pneumocystis jirovecii pneumonia was a relatively rare infection before the AIDS epidemic. Infection with P.jirovecii is an AIDS-defining illness. People with a weakened immune system (i.e. people having medical conditions like an organ transplant, blood cancer, autoimmune diseases, stem cell transplant, etc) are at high risk of developing Pneumocystis pneumonia.
Do you know?Pneumocystis jiroveciwas previously classified as a protozoan. In tissue, it appears as a cyst that resembles the cyst of protozoa. Currently, it is considered a fungus, based on nucleic acid and biochemical analysis. In 1988, scientists have changed both the classification and the name of this organism since it first appeared in patients withHIV.
Salient features ofPneumocystis jirovecii
Differences with fungal pathogens
- It does not grow in vitro in fungal culture media.
- Ergosterol which is the major cell wall component of the fungal pathogen is absent in P. jiroveci.
- It is insensitive to most conventional anti-fungal agents.
Similarities with fungal pathogens
- Possess chitin in all stages of its life cycle.
- Pneumocystis takes fungal stain eg. methenamine silver stain.
- Pneumocystis and fungi have similar cyst wall ultrastructure.
- The protein synthesis elongation factor (EF3) and thymidylate synthase of Pneumocystisare more homologous to those of ascomycetous fungi.
- The ribosomal RNA studies reveal that 16S-like RNA of Pneumocystis shares substantial sequence homology with various species of Ascomycota.
Pathogenesis
Pneumocystis is transmitted from person to person through an airborne route. Asymptomatic lung colonization can occur in immunocompetent people but people with HIV/AIDS or immunocompromised patients may show signs of fever, cough, dyspnea, and, in severe cases, respiratory failure.
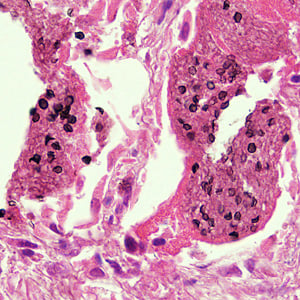
P. jirovecii has a special predilection for lung tissues. It attaches to the Type I alveolar epithelium, which allows the fungus to transition from its small trophic form to the larger cystic form. It causes hypertrophy of alveolar cells. The inflammatory response of the host causes lung injury and may also result in infiltration of macrophages; filling alveolar spaces with foamy eosinophilic material and plasma cells. This impairs gaseous exchange, leading to hypoxia and possibly respiratory failure.
Laboratory Diagnosis
Pneumocystis jiroveciicannot be cultured in vitro, therefore, laboratory diagnosis relies on cytological staining, immunofluorescent assay, or molecular diagnosis in bronchopulmonary secretions.
Sample
Expectorated sputum has a very low sensitivity and should not be submitted for diagnosis. Bronchoalveolar lavage (BAL) and induced sputum have been demonstrated to be the most useful clinical samples. In situations where these two techniques cannot be used, transbronchial biopsy or open lung biopsy may be used.
Microscopy and staining
Giemsa stain is used to demonstrate the nuclei of trophozoites and intracystic stages and silver stain is used to demonstrate the cyst wall. Immunofluorescence microscopy using monoclonal antibodies can detect both cystic and trophic forms with higher sensitivity than conventional microscopy.
Culture
Does not grow in fungal culture media and even in cell culture. In 2014, Verena Schildgen et al. reported a successful culture of P.jirovecii from BAL specimen but Liu et.al, could not reproduce the result(i.e. they failed to culture P. jirovecii).
Molecular Diagnosis
Molecular methods have shown very high sensitivity and specificity and are regarded as the gold standard technique for the detection of P. jirovecii. The genome of P. jirovecii present in the sample is amplified by Polymerase Chain Reaction (PCR) and is detected after agarose-gel analysis using a suitable DNA ladder.
Others tests
Blood test to detect β-D-glucan (a part of the cell wall of many different types of fungi) can be used to diagnose Pneumocystis pneumonia.
References and further readings
- Schildgen V, Mai S, Khalfaoui S, Lüsebrink J, Pieper M, Tillmann RL, Brockmann M, Schildgen O. 2014. Pneumocystis jiroveciican be productively cultured in differentiated CuFi-8 airway cells. mBio 5:e01186-14. doi:10.1128/mBio.01186-14.
- Liu, Y., Fahle, G. A., & Kovacs, J. A. (2018). Inability to CulturePneumocystis jirovecii. mBio, 9(3), e00939-18. doi:10.1128/mBio.00939-18
- Ruffolo JJ. Pneumocystis carinii Cell Structure. In: Walzer, PD, editor. Pneumocystis carinii Pneumonia. 2nd ed. Marcel Dekker; 1994. p. 25-43.
- Pneumocystis (Carinii) JiroveciPneumoniaby Justina Truong; John V. Ashurst.

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.