Neisseria gonorrhoeae: Properties, Pathogenesis, Virulence Factors, and Lab Diagnosis
Neisseria gonorrhoeae causes gonorrhoea — the second most common STI globally. Learn its Gram-negative diplococcus properties, virulence factors (pili, Opa proteins, IgA protease, LOS, PorB), diseases (urethritis, PID, ophthalmia neonatorum), lab diagnosis (Gram stain, culture, NAAT), and AMR resistance timeline.
A 23-year-old man presents with a 3-day history of purulent urethral discharge and dysuria. A urethral swab is taken and a Gram stain is performed while he waits. The result is ready in minutes: Gram-negative diplococci, predominantly intracellular within polymorphonuclear leucocytes. No culture is needed for presumptive diagnosis — this Gram stain appearance in urethral discharge from a symptomatic male is diagnostic for gonorrhoea.
The clinician is about to prescribe ceftriaxone but stops to check current treatment guidelines — the CDC combination therapy recommendations have changed since 2020 due to rising azithromycin resistance. The correct current regimen is ceftriaxone 500 mg IM as a single dose (or 1g if weight ≥150 kg), without routine azithromycin co-administration.
This case illustrates why Neisseria gonorrhoeae demands attention in clinical microbiology: a rapidly evolving resistance profile, simple Gram stain diagnosis in men, complex multi-site disease in women, and a global burden of over 82 million new infections annually.
Neisseria is the only pathogenic gram-negative cocci (precisely diplococci). Two species of Neisseria cause disease in humans; Neisseria meningitidis and Neisseria gonorrhoeae.
Human beings are only known hosts of N.gonorrhoeae. Neisseria gonorrhoeae (often called gonococcus) causes gonorrhoea, the second most common sexually transmitted disease (STDs) of worldwide importance (Chlamydial infections are more common). It causes disease only in humans.
Neisser described the causative agent of gonorrhea, N. gonorrhoeae, in 1879.
Morphology
- Gram-negative cocci, usually seen in pairs (diplococci) with the adjacent sides flattened (typically kidney-shaped); (Looks like two coffee beans kissing).
- In urethral discharge, it is predominately found within the polymorphs.
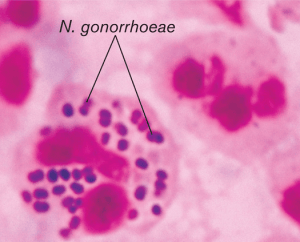 Figure: Neisseria gonorrhoeae (Gram negative diplococci)
Figure: Neisseria gonorrhoeae (Gram negative diplococci)
- Sensitive to dehydration and cold conditions.
- Gonococci do not contain capsules (meningococci do).
Mode of transmission
- Neonates acquired Neisseria gonorrhoeae from the mother during passage through the birth canal. In newborn infants, Neisseria gonorrhoeae causes ophthalmia neonatorum (purulent conjunctivitis).
- Sexual transmission: Acquired during unprotected sex with infected partner.
Virulence Factors of Neisseria gonorrhoeae
N. gonorrhoeae has evolved a sophisticated repertoire of virulence factors that allow it to adhere to mucosal surfaces, evade immune defences, acquire nutrients, and resist killing. These factors explain how a fastidious organism with no environmental reservoir successfully establishes infection in the harsh environment of the urogenital tract.
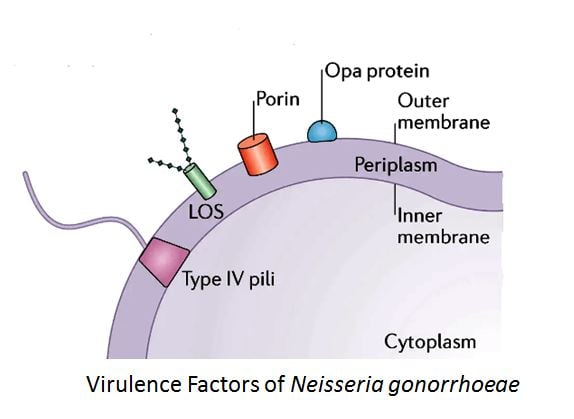 Figure: Virulence factors of Neisseria gonorrhoeae
Figure: Virulence factors of Neisseria gonorrhoeae
1. Pili (Fimbriae) — The Principal Virulence Factor
Pili are the most important virulence determinant of N. gonorrhoeae. They mediate:
- Initial attachment to non-ciliated columnar epithelial cells of the urethra, endocervix, pharynx, and conjunctiva
- Antiphagocytic action — piliated gonococci resist killing by neutrophils; non-piliated strains are avirulent in human experimental infection
Pili are composed of pilin proteins that undergo both antigenic variation (expression of antigenically different pilin proteins from a pool of silent gene cassettes) and phase variation (on/off switching of pili expression). This variation:
- Allows the organism to evade antibody-mediated immunity
- Makes vaccine development against pili extremely difficult
- Is the reason why repeated gonococcal infections do not confer lasting immunity
2. Outer Membrane Proteins — PorB (Porin)
PorB is the major outer membrane porin protein of N. gonorrhoeae. It is a voltage-gated ion channel with multiple virulence functions:
- Mediates epithelial cell invasion under low-phosphate conditions
- Serum resistance — interacts with regulators of both classical and alternative complement pathways, contributing to resistance to complement-mediated killing
- Modulates innate immune response — affects reactive oxygen species generation by neutrophils
N. gonorrhoeae expresses PorB in one of two allelic forms: P.IA strains are associated with disseminated gonococcal infection (DGI); P.IB strains typically cause localised urogenital infections.
3. Opacity (Opa) Proteins
Opa proteins are a family of antigenically distinct outer membrane proteins that undergo phase-variable expression — each gonococcal strain carries 11–12 opa genes but expresses a variable subset:
- Promote persistence in the female genital tract
- Mediate invasion of epithelial cells
- Responsible for the opaque colony morphology on agar (Opa-expressing colonies appear opaque; non-expressing colonies appear transparent)
- Phase variation in Opa expression allows immune evasion throughout the course of infection
4. IgA1 Protease
N. gonorrhoeae produces two distinct extracellular IgA1 proteases that cleave the heavy chain of secretory IgA1 at the hinge region:
- Destroys secretory IgA at mucosal surfaces — the antibody that would otherwise block attachment
- Split products of IgA1 have been found in genital secretions of women with gonorrhoea
- Production of IgA protease is shared with N. meningitidis — reflects their common mucosal niche
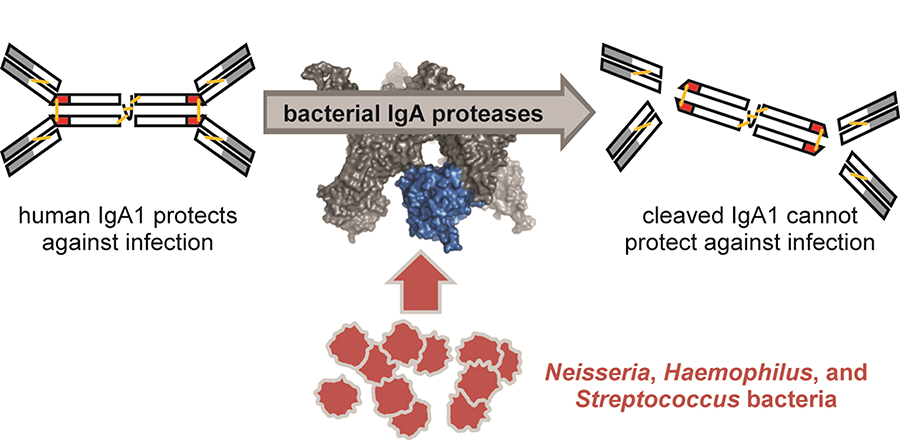 Figure: Role of IgA protease (Image source: Tufts University)
Figure: Role of IgA protease (Image source: Tufts University)
5. Lipooligosaccharide (LOS)
Unlike most Gram-negative bacteria, N. gonorrhoeae produces lipooligosaccharide (LOS) rather than full-length lipopolysaccharide — it has lipid A and core oligosaccharides but no repeating O-antigen side chains:
- Activates the alternative complement pathway
- Marked endotoxic activity — stimulates TNF-α production causing local tissue damage
- LOS undergoes molecular mimicry — its lacto-N-neotetraose structure mimics human cell surface oligosaccharides, reducing antibody recognition
- Sialylation of LOS (acquisition of host sialic acid) further enhances serum resistance
6. Transferrin-Binding Proteins (TbpA and TbpB)
Iron is essential for gonococcal growth and is limiting in host tissues. N. gonorrhoeae scavenges iron exclusively from human transferrin and lactoferrin using two transferrin-binding proteins:
- TbpA and TbpB specifically bind human transferrin (not transferrin from other species — explaining species specificity)
- This iron acquisition mechanism is essential for infection and represents a potential vaccine target
Virulence Factor Summary Table
| Virulence factor | Role | Clinical significance |
|---|---|---|
| Pili | Attachment; antiphagocytic | Principal virulence factor; no lasting immunity due to antigenic variation |
| PorB | Cell invasion; complement resistance | P.IA → disseminated disease; P.IB → local disease |
| Opa proteins | Persistence; invasion; colony opacity | Phase variation enables immune evasion |
| IgA1 protease | Destroys mucosal IgA | Clears antibody blocking attachment |
| LOS | Endotoxin; complement activation; mimicry | Tissue damage; serum resistance |
| Transferrin-binding proteins | Iron acquisition | Species-specific; essential for growth in vivo |
Disease caused by Neisseria gonorrhoeae
Gonococci cause localized infections, usually in the genital tract, and disseminated infections.
 Figure: Opthalmia neonatorum
Figure: Opthalmia neonatorum
- Gonorrhoea in men is characterized primarily by urethritis accompanied by dysuria and a purulent discharge. Epididymitis can occur.
- In women, infection is located primarily in the endocervix, causing a purulent vaginal discharge and inter-menustrual bleeding (cervicitis). The most frequent complication in women is an ascending infection of the uterine tubes (salphingitis, pelvic inflammatory disease (PID)), which can result in sterility or ectopic pregnancy as a result of scarring of tissues.
- In newly born children: Ophthalmia neonatorum (An eye infection which may develop within 2/3 days of vaginal delivery, affects cornea and can cause blindness)
Disseminated gonococcal infections occurs via the blood stream. Gonococcal strains causing disseminated infections are usually resistant to serum and complement. Disseminated infections commonly manifest as septic arthritis, tenosynovitis, pustules in the skin, endocarditis, and meningitis.
Laboratory diagnosis of Gonorrhoea
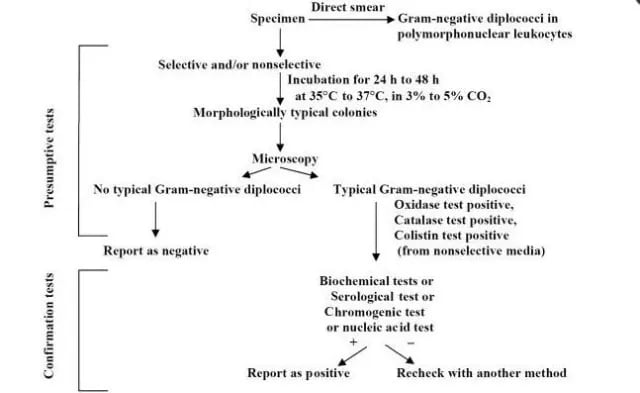 Figure: Algorithm for culture and identification of Neisseria gonorrhoeae
Figure: Algorithm for culture and identification of Neisseria gonorrhoeae
Sample
urethral/cervical/vaginal discharge
- To obtain a urethral specimen swab ( cotton or rayon swab) is inserted approximately 2cm in urethra and rotated gently before withdrawing.
- If there is profuse urethral discharge in male, it can be collected without inserting the swab.
- A few drops of first voided urine can be used in males, but the sensitivity is low compared to discharge.
Transport
Swabs collected for isolation of gonococci may be transported to the laboratory in modified Staurt’s or Amie’s charcoal transport media and held at room temperature until inoculated to culture media. Good recovery of gonococci is possible if swabs are cultured within 12 hours of collection.
Gram Staining
 Figure: Neisseria gonorrhoeae in New York City Agar (LCAT).
Figure: Neisseria gonorrhoeae in New York City Agar (LCAT).
For men, a gram-stained smear of urethral discharge (exudate) showing intracellular Gram-negative diplococci is diagnostic. But as women may carry normal vaginal flora such as Veillonella or occasional gram-negative coccobacilli , may resemble gonococci, same results in case of women may not be diagnostic so culture and identification process is needed, which is a confirmatory test.
Culture
Modified Thayer Martin Medium {Chocolate agar containing antibiotics (vancomycin, colistin, trimethoprim, and nystatin)} is most often used. Modified Newyork City Medium (MNC) is also used for the culture of Neisseria gonorrhoeae. MNC also supports the growth of Mycoplasma.
Biochemical tests for Neisseria gonorrhoeae identification
- Oxidase Test: Positive
- Ferments glucose but not maltose, sucrose or lactose
- DNase Test: Negative
- Beta-galactosidase (ONPG) Test: Negative
- Glutamyl-aminopeptidase (GAP) Test: Negative
Serology
Serological tests to determine the presence of antibody to gonococci are not useful for diagnosis.
Molecular Diagnosis
Presence of gonococcal nucleic acids in patient specimens, using amplification or non-amplification method. These tests are highly sensitive and specific.
Drug Resistance
Antimicrobial resistance in Neisseria gonorrhoeae has been categorized by the CDC as an “urgent threat”.
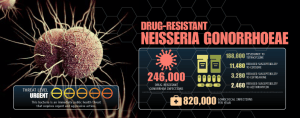 Figure: Neisseria gonorrhoeae infections is an urgent Threat (CDC)
Figure: Neisseria gonorrhoeae infections is an urgent Threat (CDC)
Currently, the CDC recommends an intramuscular shot of an extended-spectrum cephalosporin (ESC), ceftriaxone, plus one oral dose of azithromycin as an empirical treatment for uncomplicated or pharyngeal gonococcal infections.
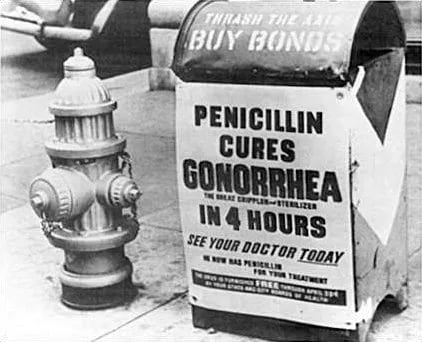 Figure: Penicillin cures Gonorrhea (Source)
Figure: Penicillin cures Gonorrhea (Source)
Current Treatment and Antimicrobial Resistance
Current CDC recommendation (2020–2023 update):
- Uncomplicated urogenital/anorectal gonorrhoea: Ceftriaxone 500 mg IM single dose (or 1g IM if body weight ≥150 kg)
- If chlamydial coinfection cannot be excluded: Add doxycycline 100 mg orally twice daily × 7 days
- Routine dual therapy with azithromycin is no longer recommended — rising azithromycin resistance among gonococci has made azithromycin co-administration counterproductive
Why treatment has changed so dramatically:
- 1935s: Antimicrobial treatment of gonorrhea started in 1935 after discover of sulfanilamide. Neisseria gonorrhoeae developed widespread resistance to sulfanilamide within the first ten years resulting in treatment failures.
- 1940s: Penicillin is used as a treatment of choice for gonorrhea. Penicillin remained effective for next few decades despite a continuous and insidious increase in MICs.
- 1976: End of era of penicillin with discovery and worldwide spread of Neisseria gonorrhoeae harboring plasmid-mediated beta-lactamases.
- 2010s: Alarming decrease in cefixime susceptibility reported from around the world.
- 2018s: Combination of azithromycin and ceftriaxone – has failed to treat the disease
- 2020–2023: CDC removes azithromycin from routine dual therapy due to azithromycin resistance exceeding 5% in surveillance data. Ceftriaxone monotherapy (higher dose) is now the standard. WHO classifies N. gonorrhoeae as a priority 2 (high) pathogen for development of new antibiotics. Oral cefixime is no longer recommended due to pharmacodynamic concerns.
The clinical importance of this change: Providers who continue using the pre-2020 regimen (ceftriaxone + azithromycin) are prescribing suboptimal therapy that contributes to azithromycin resistance without providing additional clinical benefit. Always verify current guidelines — N. gonorrhoeae resistance evolves rapidly.
How to Remember
The Gram stain diagnosis rule:
- Symptomatic male + urethral discharge + intracellular GN diplococci on Gram stain = diagnostic for gonorrhoea (no culture needed for presumptive diagnosis)
- Female (any discharge) + cervical/vaginal sample + GN diplococci = NOT diagnostic (normal vaginal flora may resemble gonococci) → culture or NAAT required
The maltose test — distinguishing gonococcus from meningococcus: Gonococcus: glucose only (no maltose) Meningococcus: glucose AND maltose Memory: Gonococcus = Glucose only; Meningococcus = Maltose too
For a full systematic comparison of both organisms — properties, diseases, virulence, and lab tests side by side — see the dedicated article: Differences between N. gonorrhoeae and N. meningitidis
Virulence factor logic — why each one matters:
- Pili → get in (attachment); phase variation → evade antibody
- Opa proteins → stay in (persistence); phase variation → evade again
- IgA protease → destroy the IgA trying to block attachment
- PorB → resist complement killing in blood (→ disseminated disease)
- LOS → damage tissue (TNF-α); mimic host to avoid detection
- Transferrin binding → steal iron to survive in host tissues
The disseminated gonorrhoea triad: Skin pustules + septic arthritis + tenosynovitis = disseminated gonococcal infection (DGI) Organisms causing DGI typically express P.IA PorB and are serum-resistant (complement-resistant)
References
- Tille, P. M. (2017). Bailey and Scott's Diagnostic Microbiology (14th ed.). Elsevier.
- Edwards, J. L., & Apicella, M. A. (2004). The molecular mechanisms used by Neisseria gonorrhoeae to initiate infection differ between men and women. Clinical Microbiology Reviews, 17(4), 965–981. https://doi.org/10.1128/CMR.17.4.965-981.2004
- Chen, A., & Seifert, H. S. (2013). Neisseria gonorrhoeae-mediated inhibition of apoptotic signalling in polymorphonuclear leukocytes. Infection and Immunity, 81(12), 4474–4482. https://doi.org/10.1128/IAI.00693-13
- Quillin, S. J., & Seifert, H. S. (2018). Neisseria gonorrhoeae host adaptation and pathogenesis. Nature Reviews Microbiology, 16(4), 226–240. https://doi.org/10.1038/nrmicro.2017.169
- Centers for Disease Control and Prevention. (2021). Sexually Transmitted Infections Treatment Guidelines, 2021: Gonococcal Infections. MMWR, 70(4). https://www.cdc.gov/std/treatment-guidelines/gonorrhea.htm
- World Health Organization. (2016). WHO Guidelines for the Treatment of Neisseria gonorrhoeae. Geneva: WHO.

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.