Mucormycosis is a rare and life-threatening fungal disease caused by a group of fungi collectively known as mucormycetes. Since the disease is very fatal, timely diagnosis is crucial for treatment, survival and to reduce the need and extent of surgical resection, disfigurement, and suffering.
The clinical approach to the diagnosis of mucormycosis relies on a high index of suspicion, knowledge of predisposing factors, assessment of presenting signs and symptoms, imaging studies, etc. Mucormycosis can often be misdiagnosed because of its non-specific symptoms and radiological features. For e.g. cases of pulmonary mucormycosis may be diagnosed as aspergillosis, because of its similar sign, symptoms, and radiological presentation of the lungs.
Definitive diagnosis is based on laboratory methods of direct examinations of clinical specimens, fungal cultures, and histopathology.
Table of Contents
Sample
Specimens vary according to the type of infection and clinical presentations. Most commonly used samples include skin scrapings from cutaneous lesions, nasal discharges, scrapings and aspirates from sinuses in patients with rhinocerebral lesions, bronchoalevolar lavages and needle biopsies from pulmonary lesions, and biopsy tissue from patients with gastrointestinal and/or disseminated disease.
Direct microscopic examination
KOH mounts
For a rapid presumptive diagnosis of mucormycosis, KOH wet mounts can be used for direct microscopy. It can be applied to all materials sent to the clinical laboratory. KOH when supplemented with fluorescent brighteners such as Blankophor and Calcofluor white, enhance the visualization of the characteristic fungal hyphae but requires a fluorescent microscope.

If present, the preparation shows, typically thick-walled, refractile hyphae 6–15µm in diameter, swollen cells (≤50 µm) and, sometimes, distorted hyphae. The angle of branching is variable and includes wide-angle (90°) bifurcations.
Histopathological examination
Tissue sections fixed and stained with haematoxylin and eosin (H&E) or specialized fungal stains, such as Grocott methenamine-silver (GMS) or periodic acid-Schiff (PAS) reveal broad-based, ribbon-like, non-septate hyphae with wide-angle branching (approximately 90°).

percutaneous lung biopsy shows broad-based, ribbon-like, non-septate hyphae with right-angle branching and swollen cells. (Image source)
Histopathology is a very important diagnostic tool since it distinguishes the presence of the fungus as a pathogen in the specimen from a culture contaminant and is indispensable to define whether there is blood vessel invasion. It can also reveal co-infections with other molds.
Both of the direct staining methods are inexpensive, yet invaluable method to rapidly give a presumptive diagnosis. However, it cannot identify a fungus to the genus or species level.
Culture methods
Culture is a method of a definitive diagnosis of mucormycosis and allows both identification to the genus and species level, and antifungal susceptibility testing.
Most medically important Mucorales are thermotolerant and are able to grow rapidly at (3–5 days) on most fungal culture media, such as Sabouraud agar and potato dextrose agar incubated at 25–30°C. For species of Cunnighamella and Rhizopus genera, a microaerophilic environment improves culture yield. Some other species Apophysomyces elegans and Saksenaea vasiformis fail to sporulate on routine media, therefore, require a nutrient-poor medium (e.g., water agar with 0.1% yeast extract) to sufficiently sporulate for microscopic identification.
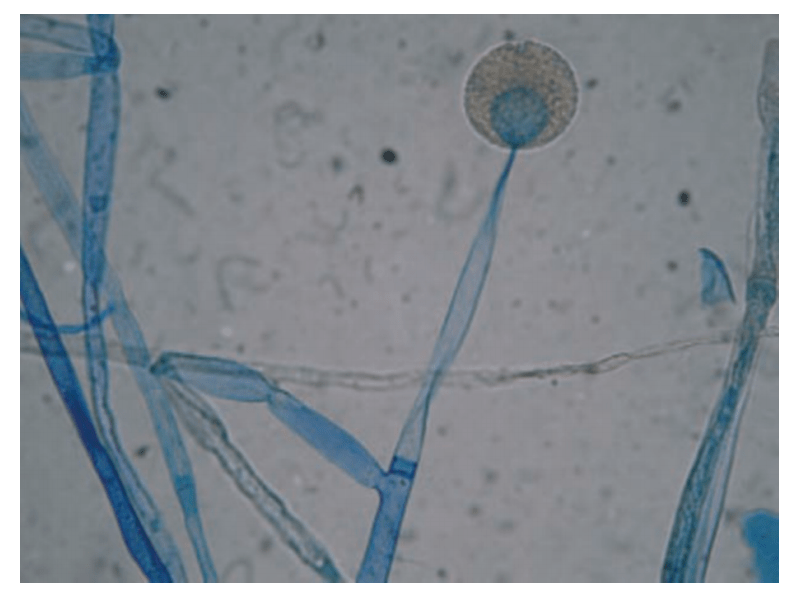
cotton blue staining shows a globose intact sporangium with sporangiospores and branched sporangiophores. (Image source)
Colonies produce fluffy white, gray, or brown hyphae filling the culture container within 24 to 96 hours. The hyphae are coarse and dotted with brown or black sporangia. It is impossible to distinguish the genera based on colony morphology, as they appear similar.

Identification of genera is based on the presence of aseptate hyphae and sporangial morphology. This includes the arrangement and number of sporangiospores, the shape, color, presence or absence of columellae and apophyses, as well as the arrangement of the sporangiophores and the presence or absence of rhizoids. Lactophenol cotton blue staining can be used to achieve better visualization.
Some of the most common types include
| Organisms | Best growth °C | Sporangiophore | Apophysis | Columella | Sporangium | Rhizoids |
| Absidia sp. | 37 | Branched, hyaline | Conical | Dome-shaped | Pear-shaped | Primitive, rare |
| Apophysomyces sp. | 24-42 | Non-branched, brown | Bell-shaped | Rarely elongated | Pear-shaped | Tuft, originating from a foot cell |
| Mortierella sp. | >40 | Branched, hyaline | – | – | Spherical | Primitive |
| Mucor sp. | <37 | Branched, non-branched, hyaline | – | Varying shapes | Spherical | Absent |
| Rhizomucor sp. | 20-60 | Branched, brown | – | Spherical | Spherical | Primitive, rare |
| Rhizopus sp. | 37 | Non-branched, brown | Not prominent | Spherical | Spherical | Abundant, often well developed. |
Limitations of Culture
- Culture positivity rate is very low, if isolated it should be correlated with clinical presentation and predisposing factors for confirmation.
- Isolation may be hampered if the processing of the specimens involves tissue grinding, a procedure that kills the non-septate hyphae of these fungi.
- Exudates and necrotic tissue contain few viable organisms; thus the inoculum from these specimens must be heavy
- Since Zygomycetes may be isolated as contaminants from laboratory material, their isolation from clinical specimens of susceptible hosts should not be disregarded as contamination.
Serology
Antibodies to Zygomycetes can be detected by enzyme-linked immunosorbent assays (ELISAs), double diffusion, immunoblot assays. However, these are not in use due to poor specificity and sensitivity, cross-reactivity with Candida and Aspergillus species or lack clinical validation.
Molecular methods
Recent advances in molecular biology have contributed to the development of rapid, accurate, and sensitive methods for pathogen detection. Most commonly used are conventional PCRs, RFLP, DNA sequencing of defined gene regions, and melt curve analysis of PCR products.
- The conventional PCR assay is based on analysis of internal transcribed spacer (ITS) region. Modifications by pan-fungal PCR followed by oligonucleotide array for species discrimination provides a high sensitivity. However, these are cost intensive, require skilled personnel to interpret the data generated, more laborious, and susceptible to cross contaminations.
- A PCR-RFLP assay targeting the 18S rRNA gene is effective for detection of mucormycetes, owing to its low molecular evolution rate. However, it is not in use because of its high cost (as restriction enzymes are expensive) and labor intensive process.
- DNA sequencing targeting the ITS sequence is efficient for the identification of mucormycetes down to genus and species level. It can be applicable directly to the DNA extracted and amplified from frozen tissue.
- A semi-nested RT-PCR assay targeting cytochrome B genes followed by high-resolution melt curve analysis (HMR), allows genus detection and identification of species within the genus with high sensitivity.
- There is therefore a lot of ongoing research, focusing on non-invasive methods, such as qPCR for the detection of circulating mucoralean DNA in blood (plasma or serum) or urine as it has a low turnaround time and has a low detection level capacity.
Automated systems
Proteomic profiling (e.g., MALDI-TOF) is already well established for routine identification of bacteria and yeasts but is difficult in the case of molds due to the presence of complex fungal structures (single or multiple types of conidia, mycelium and/or yeast stages), wide differences of growth rates and lack of valid databases.
The major advantages of MALDI-TOF are given by low costs per reaction, automated interpretation profiles, and fast turnaround times. It is a cost-effective solution but the database for MALDI-TOF identification needs to be further enriched and the cultivation and extraction methods need to be optimized to make this method applicable for routine identification of mucormycetes.
References and further readings
- C. Lass-Florl, Zygomycosis: conventional laboratory diagnosis, Clinical Microbiology and Infection, Volume 15, Supplement 5,2009, Pages 60-65 (Tables and figures of culture and microscopy)
- Robert Branscomb, MT(ASCP) An Overview of Mucormycosis Lander Medical Clinic, Lander, WY laboratorymedicine> june 2002> number 6> volume 33
- Lackner M, Caramalho R 1 & Lass-Flörl C Laboratory diagnosis of mucormycosis: current status and future perspectives Future Microbiol. (2014) 9(5), 683–695