Aspergillus fumigatus: Morphology, Pathogenesis, Lab Diagnosis
Aspergillus fumigatus: virulence mechanisms (gliotoxin, fibrinogen binding), invasive aspergillosis pathogenesis, galactomannan testing protocol, azole resistance, and treatment. The species responsible for ~90% of invasive aspergillosis cases.
Aspergillus fumigatus is the single most clinically significant species within the genus Aspergillus, responsible for approximately 90% of cases of invasive aspergillosis; the most severe and life-threatening form of Aspergillus disease. While the genus Aspergillus contains over 250 species (with A. flavus, A. niger, and A. terreus also having clinical relevance), A. fumigatus deserves dedicated attention because of its unique virulence factors, its dominant role in invasive disease, and the growing clinical concern around antifungal resistance in this specific species.
For general Aspergillus characteristics, classification, all clinically important species, and the complete spectrum of aspergillosis clinical syndromes, see our comprehensive Aspergillus guide. This article focuses specifically on what makes A. fumigatus clinically distinct.
What makes *A. fumigatus* the dominant invasive species
Compared to other Aspergillus species, A. fumigatus has three properties that explain its clinical dominance in invasive disease:
- Small conidial size (2–3.5 µm) — small enough to bypass upper respiratory tract filtering and reach the alveoli directly, unlike A. flavus (3–6 µm conidia, which tend to deposit in the upper respiratory tract causing sinusitis instead)
- Thermotolerance — A. fumigatus grows at 37°C (body temperature) and survives temperatures up to 70°C, an adaptation that may have evolved from its ecological niche in compost and decaying vegetation, but which conveniently allows it to thrive at human body temperature
- Gliotoxin production — a potent immunosuppressive mycotoxin (detailed below) that actively disables the host's primary cellular defence against this organism
Major characteristics of *Aspergillus fumigatus*
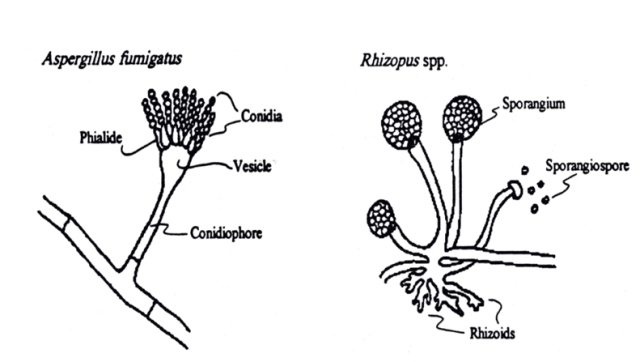 Figure: Aspergillus fumigatus and Rhizopus
Figure: Aspergillus fumigatus and Rhizopus
- Aspergillus species exist only as molds, they are not dimorphic.
- Highly aerobic in nature
- They have septate hyphae that form dichotomous branches (lateral and/or apical branches the same width as the parent hyphae from which they were derived) emerging at ~ 45-degree angles from the parent hyphae (i.e. acute angle branching).
- The walls of the hyphae are more or less parallel, in contrast to Mucor and Rhizopus walls, which are irregular.
- The conidia of Aspergillus form radiating chains in contrast to those of Mucor and Rhizopus, which are enclosed within a sporangium.
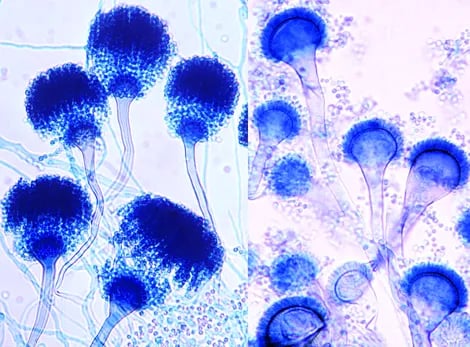 Figure: Conidial heads of A. fumigatus. Note: uniseriate row of phialides on the upper two thirds of the vesicle.
Figure: Conidial heads of A. fumigatus. Note: uniseriate row of phialides on the upper two thirds of the vesicle.
Aspergillus binds to fibrinogen and laminin in the alveolar basement membrane. Macrophages are able to ingest and kill the conidia but the organism produces gliotoxin which may inhibit phagocytosis.
Why gliotoxin matters: the immune evasion mechanism explained
Gliotoxin is an epipolythiodioxopiperazine (ETP) class mycotoxin produced by A. fumigatus that actively disables the host's first line of cellular defence:
- Induces apoptosis (programmed cell death) in macrophages and other immune cells after they ingest conidia
- Inhibits NADPH oxidase activity in phagocytes, reducing their ability to generate the reactive oxygen species needed to kill ingested conidia
- Suppresses T-cell activation and proliferation
- Inhibits NF-κB signalling, reducing the inflammatory response that would otherwise recruit more immune cells to the site of infection
This explains a critical clinical pattern: A. fumigatus doesn't just passively evade the immune system because the host is immunocompromised — it actively produces a molecule that disables the immune cells that do encounter it. This is part of why neutropenic patients (with very few neutrophils to begin with) are at such extreme risk: not only do they have fewer phagocytes, but the few macrophages encountering the fungus are also being actively suppressed by gliotoxin.
Neutrophils can adhere and kill the hyphae. If neutrophils are overwhelmed by more numbers of hyphae, they may invade pulmonary and vascular tissue leading to thrombosis and necrosis which may lead to hematogenous spread (to other organs including brain).
Aspergillus fumigatus can colonize and later invade abraded skin, wounds, burns, the cornea, the external ear and paranasal sinuses. It is the most common cause of fungal sinusitis. In immunocompromised patients especially those with neutropenia, it can invade the lungs and other organs causing invasive aspergillosis.
Aspergilli are well known for their ability to grow in cavities in lungs, especially cavities caused by tuberculosis. Within the cavities, they produce an aspergilloma “fungus ball”, which can be seen on X-ray as a radiopaque structure that changes its position when the patient is moved from an erect to a supine position.
Allergic bronchopulmonary aspergillosis (ABPA) is an infection of the bronchi by Aspergillus species. Patient with ABPA has asthmatic symptoms with a high IgE titer against Aspergillus antigens, and they expectorate bronchial plugs containing hyphae.
Laboratory Diagnosis
Sample: Sputum, bronchial washings, and tracheal aspirates from patients with pulmonary disease and tissue biopsies from patients with disseminated disease.
Direct Microscopic Examination: Biopsy specimen shows septate, branching hyphae invading tissue. KOH preparation of sputum, bronchoalveolar lavage, transbronchial biopsy, and other biopsies reveal non-pigmented septate hyphae, 3-5 um in diameter with characteristic dichotomous branching. The hyphae have a tendency to branch repeatedly. The branches arise at an angle of approximately 45 degrees.
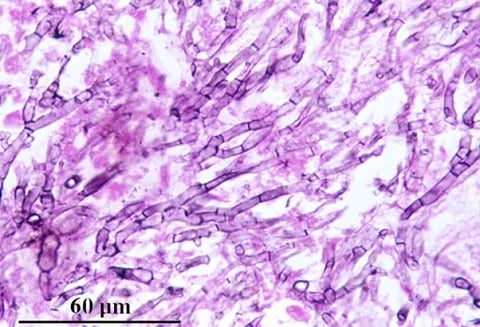 Figure: Dichotomously branched, septate hyphae of Aspergillus fumigatus in lung tissue section after Methenamine silver stain(Source)
Figure: Dichotomously branched, septate hyphae of Aspergillus fumigatus in lung tissue section after Methenamine silver stain(Source)
Culture: Culture is regarded as the ‘Gold Standard Method’. Clinical specimens should be inoculated onto primary isolation media, like Sabouraud’s dextrose agar. Colonies are fast-growing and may be white, yellow, yellow-brown, brown to black, or green in color. Microscopically, cultures show colonies with characteristic radiating chains of conidia. However, positive cultures from a non-sterile specimen, such as sputum, do not prove disease because colonization is common.
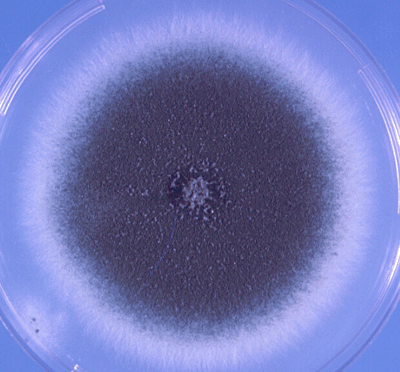 Figure: colonies of A.fumigatus with typical blue-green surface pigmentation on Czapek dox agar (Source)
Figure: colonies of A.fumigatus with typical blue-green surface pigmentation on Czapek dox agar (Source)
Antigen detection: Several antigen tests for the detection of Aspergillus from blood, urine and CFS are now available. In a person with invasive aspergillosis, there may be high titers ofgalactomannan antigenin serum. As galactomannan is rapidly eliminated from the blood, serial screening twice weekly is recommended for optimal diagnosis.
Antibody detection (serology): Immunodiffusion tests for the detection of antibodies to Aspergillus species have proven to be of value in the diagnosis of allergic, aspergilloma, and invasive aspergillosis. Patient with ABPA has high levels of IgE specific for Aspergillus antigens. IgG precipitins are also present.
Azole Resistance in *Aspergillus fumigatus*: An Emerging Clinical Crisis
Triazole antifungals (voriconazole, itraconazole, posaconazole, isavuconazole) are first-line treatment for invasive aspergillosis. Over the past two decades, azole-resistant A. fumigatus has emerged as a serious clinical problem, with two distinct origins that every clinician and microbiologist should understand:
1. Agricultural (environmental) resistance — the dominant mechanism
This is the more concerning and more common route, and it is unique among major resistance crises because the resistance develops in the environment, not in the patient.
Azole-class fungicides (structurally similar to medical triazole antifungals) are widely used in agriculture to protect crops from fungal disease. A. fumigatus is ubiquitous in soil and compost — it is repeatedly exposed to these agricultural azole fungicides in the environment. This exposure selects for resistant strains in the environment, completely independent of any human antifungal treatment.
The clinical consequence: A patient can present with azole-resistant invasive aspergillosis on their very first exposure to the organism — having never received antifungal treatment before. This is fundamentally different from typical antibiotic resistance, which usually develops after a patient receives the drug. The most common resistance mutation associated with environmental azole resistance is the TR34/L98H mutation in the cyp51A gene.
2. Patient-acquired resistance
Less common, but still clinically significant — resistance can develop during prolonged azole therapy in an individual patient, particularly in patients with chronic pulmonary aspergillosis or aspergilloma receiving long-term azole treatment, or in patients with cavitary lung disease where the fungal burden persists despite treatment.
Clinical and laboratory implications
- Antifungal susceptibility testing is increasingly recommended for A. fumigatus isolates from invasive disease, particularly in regions with documented environmental resistance
- Molecular detection of cyp51A mutations can provide faster resistance detection than traditional culture-based susceptibility testing, which can take days
- When azole resistance is confirmed or strongly suspected, liposomal amphotericin B becomes the preferred first-line agent rather than voriconazole
- Geographic surveillance matters — environmental azole resistance rates vary significantly by region, reflecting local agricultural fungicide use patterns, and clinicians should be aware of local resistance prevalence when selecting empirical therapy
Why fumigatus deserves special attention?
"A. fumigatus doesn't just wait for a weak immune system — it actively disables the one it finds, and increasingly, it may already be resistant to your first-choice drug before you've even started treatment."
This single sentence captures why A. fumigatus is treated as clinically distinct from other Aspergillus species: its unique virulence biology (gliotoxin-mediated immune suppression) and its unique resistance epidemiology (environmentally-acquired, pre-existing resistance) both demand specific clinical awareness beyond general Aspergillus knowledge.
Treatment
For the treatment of invasive aspergillosis, voriconazole is the drug of choice, and liposomal amphotericin B, posaconazole, caspofungin, and isavuconazonium are alternative drugs. A fungus ball growing in a sinus or in a pulmonary cavity can be surgically removed. Patients with ABPA can be treated with corticosteroids and antifungal agents, such as itraconazole.
References and further reading
- Aspergillus- The University of Adelaide
- Laboratory methods in Basic Mycology in Bailey & Scott’s Diagnostic Microbiology, Forbes, 11th edition
- Verweij, P. E., Snelders, E., Kema, G. H., Mellado, E., & Melchers, W. J. (2009). Azole resistance in Aspergillus fumigatus: a side-effect of environmental fungicide use? The Lancet Infectious Diseases, 9(12), 789–795. https://doi.org/10.1016/S1473-3099(09)70265-8
- Scharf, D. H., Heinekamp, T., & Brakhage, A. A. (2014). Human and plant fungal pathogens: the role of secondary metabolites. PLoS Pathogens, 10(1), e1003859. https://doi.org/10.1371/journal.ppat.1003859
Frequently Asked Questions
Why is Aspergillus fumigatus responsible for more invasive disease than other species?
What is gliotoxin and how does it help A. fumigatus evade immunity?
What is environmental azole resistance and why is it different from typical resistance?
How is galactomannan testing used to diagnose invasive aspergillosis?
What is first-line treatment for invasive aspergillosis and when does it change?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.