Antimicrobial Susceptibility Testing (AST): Guidelines and Best Practices
Antimicrobial Susceptibility Testing (AST): Guidelines and Best Practices
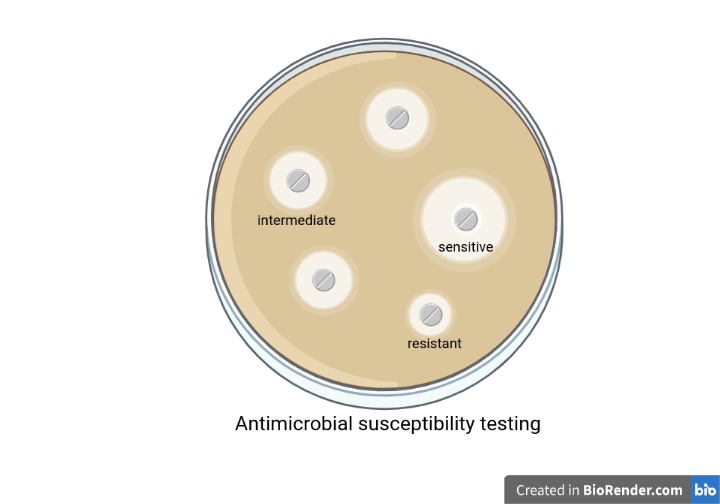
Antibiotic susceptibility testing should be performed only on clinically significant isolates, not on all microorganisms recovered in culture. Clinical and Laboratory Standards Institute (CLSI) recommends the use of modified Kirby-Bauer method for routine antibiotic susceptibility testing.
According to CLSI, to avoid errors following guidelines should be used:
- Antibiotic discs should be of the correct diameter (6.35 mm).
- Antibiotic discs should be of the right potency.
- The stock supply should be stored frozen (-20° C).
- The working supply should be kept no longer than one month in a refrigerator (2–8° C).
- Only Mueller Hinton agar of performance-tested quality should be used.
- Correct pH (7.2–7.4) of the finished medium is essential for some antibiotics.
- The inoculum should be standardized against the prescribed turbidity standard.
- Zone sizes should be measured precisely.
- Zone sizes should be interpreted by referring to a table of critical diameters. Zone diameters for each organism should fall within limits.
Antimicrobial susceptibility testing should be carried out with the standard strains to evaluate and validate the test procedure and the materials used in susceptibility testing. Such testings should be done;
- when a new batch of discs is put into use;
- when a new batch of medium is put into service;
- Once a week, in parallel with the routine antibiograms.
Standard strains that are commonly used in practice are;
- Staphylococcus aureus(ATCC 25923;
- Escherichia coli(ATCC 25922);
- Pseudomonas aeruginosa (ATCC 27853).
Selection of Antimicrobial Agents
Antimicrobial agents for testing against a particular bacterial isolate are the antimicrobial battery or panel. Selecting the appropriate antimicrobials for susceptibility testing can be challenging given the vast numbers of antimicrobial agents available.
****Certain microorganisms can be intrinsically resistantto particular antimicrobial classes; therefore, it is unnecessary and misleading to test specific agents for activity in vitro. Antimicrobials to which the organisms are intrinsically resistant are routinely excluded from the test battery (eg vancomycin vs. gram-negative bacilli).
Nitrofurantoinis limited to useonly in the treatment of urinary tract infections, and should not be tested against microorganisms recovered from material other than urine.
Best Practices in Selection of Antimicrobial Agents for AST
- Antimicrobials of the same class may have similar in-vitro activities against selected bacterial pathogens. In these cases, a representative antimicrobial that predicts susceptibility to other members of the same class should be chosen.
- If the resistance to a particular agent is common, the utility of the agent may be sufficiently limited so that routine testing is not warranted, and only more potent antimicrobials must be included in the test panel.
- Antimicrobials developed for use against particular organisms must be included in the test panel of that organism only (e.g. ceftazidime is developed for use against Pseudomonas aeruginosa but not against Staphylococcus aureus).
- Antibiotics must be able to achieve anatomic approximation. Nitrofurantoin achieves adequate levels only in the urinary tract, so it should not be included in batteries tested against bacterial isolates from other body sites.
- The antimicrobial agent used in the test panel must be available in the local market/pharmacy.
- The use of antimicrobial susceptibility testing method also limits the use of antimicrobials as resistance may not be detected for that particular agent from this specific method in use.
- The number of antimicrobials to be tested should be limited to ensure AST’s relevance and practicality.
- A periodic review of microorganisms currently predictably susceptible to specific antimicrobial agents is recommended to ensure that emergent, unexpected resistance is detected. Following the poor response to a standard antimicrobial treatment regime, emerging resistance may also be suspected.
Set of Drugs for Antimicrobial Susceptibility Testing
World Health Organization has published the basic set of drugs for routine susceptibility testing in various situations. The drugs are divided into two sets. First set includes the drugs that are available in most hospitals and for which routine testing should be carried out for every strain.
Tests for drugs in set twoare to be performed only at the special request of the physician, or when the causative organism is resistant to the first-choice drugs, or when other reasons (allergy to a drug, or its unavailability) make further testing justified.
According to WHO, In very rare cases, one or more additional drugs should be included when there is a special reason known to the physician, or when new and better drugs become available. Therefore, periodic revision of this list is desirable, and this should be done after appropriate discussions with clinical staff. Many problems arise in practice, because clinicians are not always aware that only one representative of each group of antimicrobials is included in routine tests. The result obtained for this particular drug may then be extrapolated to all, or most, of the other members of the group.
Staphylococcus
| Set 1: First Choice | Set 2: Additional drugs |
|---|---|
| Benzylpenicillin | Gentamicin |
| Oxacillin | Amikacin |
| Erythromycin | Co-trimoxazole |
| Tetracycline | Clindamycin |
| Chloramphenicol |
Intestinal Enterobacteriaceae
| Set 1: First Choice | Set 2: Additional drugs |
|---|---|
| Ampicillin | Norfloxacin |
| Chloramphenicol | |
| Co-trimoxazole | |
| Tetracycline | |
| Nalidixic acid |
UrinaryEnterobacteriaceae
| Set 1: First Choice | Set 2: Additional drugs |
|---|---|
| Sulfonamide | Norfloxacin |
| Trimethoprim | Chloramphenicol |
| Co-trimoxazole | Gentamicin |
| Ampicillin | |
| Nitrofurantoin | |
| Nalidixic acid | |
| Tetracycline |
Enterobacteriaceae isolated from blood and tissues
| Set 1: First Choice | Set 2: Additional drugs |
|---|---|
| Ampicillin | Cefuroxime |
| Chloramphenicol | Amikacin |
| Co-trimoxazole | Ceftriaxone |
| Tetracycline | Ciprofloxacin |
| Cefalotin | Piperacillin |
| Gentamicin |
Pseudomonas aeruginosa
- The benzylpenicillindisc is used to test susceptibility to all β-lactamase-sensitive penicillins (such as oral phenoxymethylpenicillin and pheneticillin).
- Ampicillin is the prototype of a group of broad-spectrum penicillins with activity against many Gram-negative bacteria. As it is susceptible to β-lactamase, it should not be used for testing staphylococci. Generally, the susceptibility to ampicillin is also valid for other members of this group: amoxycillin, pivampicillin, talampicillin, etc.
- Oxacillin disc is representative of the whole group of β-lactamase-resistant penicillins (including meticillin, nafcillin, cloxacillin, dicloxacillin, and flucloxacillin). Moreover, there is good clinical evidence that cross-resistance exists between the meticillin and the cephalosporin groups. Therefore, it is useless and misleading to include cefalotin in the antibiogram for staphylococci. The oxacillin disc is much more resistant to deterioration and is therefore preferred for the standardized diffusion test.
- The results for the tetracycline disc may be applied to chlortetracycline, oxytetracycline, and other members of this group. However, most tetracycline-resistant staphylococci remain normally sensitive to minocycline. A disc of minocycline may thus be useful to test multiresistant strains of staphylococci.
- The result with the chloramphenicol disc may be extrapolated to thiamphenicol, a related drug with a comparable antibacterial spectrum, but without known risk of aplastic anemia.
- Erythromycin is used to test the susceptibility to some other members of the macrolide group (oleandomycin, spiramycin)
- Only one representative sulfonamide (sulfafurazole) is required in the test.
- Cefalotin. The only cefalotin needs to be tested routinely, as its spectrum is representative of all other first-generation cephalosporins (cefalexin, cefradine, cefaloridine, cefazolin, cefapirin). Where second-and third-generation cephalosporins and related compounds (cefamycins) with an expanded spectrum are available, a separate disc for some of these new drugs may be justified in selected cases (cefoxitin, cefamandole, cefuroxime, cefotaxime, ceftriaxone). Although some cephalosporins can be used to treat severe staphylococcal infections, the susceptibility of the infecting strain can be derived from the result of oxacillin
- The co-trimoxazole disc contains a combination of trimethoprim and sulfonamide (sulfamethoxazole). In co-trimoxazole the two components of this synergistic combination have comparable pharmacokinetic properties and generally act “as a single drug”.
- Aminoglycosides group includes streptomycin, gentamicin, kanamycin, netilmicin, and tobramycin. Their antimicrobial spectra are not always close enough related to permitting assumption of cross-resistance, but against susceptible pathogens, these agents have been shown to be equally effective.WHO strongly recommended that each laboratory select a single agent for primary susceptibility testing. The other agents should be held in reserve for the treatment of patients with infections caused by resistant organisms.
| Set 1: First Choice | Set 2: Additional drugs |
|---|---|
| Piperacillin | Amikacin |
| Gentamicin | |
| Tobramycin |
References
- Gajic, I., Kabic, J., Kekic, D., Jovicevic, M., Milenkovic, M., Mitic Culafic, D., Trudic, A., Ranin, L., & Opavski, N. (2022). Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods. Antibiotics (Basel, Switzerland), 11(4), 427. https://doi.org/10.3390/antibiotics11040427
- Khan, Z. A., Siddiqui, M. F., & Park, S. (2019). Current and Emerging Methods of Antibiotic Susceptibility Testing. Diagnostics (Basel, Switzerland), 9(2), 49. https://doi.org/10.3390/diagnostics9020049
- Jorgensen, J. H., & Ferraro, M. J. (2009). Antimicrobial susceptibility testing: a review of general principles and contemporary practices. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 49(11), 1749–1755. https://doi.org/10.1086/647952

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.