Staphylococcus aureus: Properties, Pathogenesis & Lab Diagnosis
Staphylococcus aureus morphology, virulence factors and the diseases they cause, plus catalase, coagulase and other tests used for lab diagnosis.
Staphylococcus aureus, a frequent colonizer of the skin and nasal mucosa of humans and animals, is a highly successful opportunistic pathogen.
Roughly a third of healthy people carry it asymptomatically in the nose at any given time. What turns this quiet colonizer into the cause of a boil, a bloodstream infection, or toxic shock syndrome is the set of virulence factors described below, each one doing a specific job in breaching, hiding from, or damaging the host.
Major Characteristics of Staphylococcus aureus
- Gram stain: Staphylococci appear as Gram-positive cocci that occur singly and in pairs, tetrads, short chains, and irregular grape-like clusters
- Catalase Test: Positive
- Coagulase Test: Positive
- Non-motile
- Non-sporing
- Often unencapsulated or have a limited capsule
- Facultative anaerobes.
Main diseases caused by Staphylococcus aureus
Mnemonic: Diseases caused by Staphylococcus can be remembered using this acronym “SOFTPAINS”
- Skin Infections & Surgical wound infections
- Osteomyelitis
- Food poisoning/gastroenteritis
- Toxic shock syndrome
- Pneumonia (mainly hospital-acquired)
- Acute endocarditis
- Infective arthritis
- Necrotizing fasciitis
- Sepsis and Staphylococcal scalded skin syndrome (SSSS)
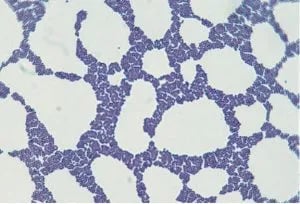 Figure: Staphylococcus in Gram Stain
Figure: Staphylococcus in Gram Stain
Virulence Factors and How They Cause Disease
 Three groups are easier to hold in your head than separate names of virulence factors. Ask what job each one does: hide the bacterium, anchor it in place, or damage the host.
Three groups are easier to hold in your head than separate names of virulence factors. Ask what job each one does: hide the bacterium, anchor it in place, or damage the host.
Analogy for the three-bucket virulence framework: Think of S. aureus like a burglar. Surface factors are the disguise (capsule, Protein A, teichoic acid, hiding from the homeowner's alarm system, your immune system). Enzymes are the tools (coagulase walls off the room it's robbing, hyaluronidase cuts through to the next room). Toxins are the damage left behind (hemolysins, exfoliative toxins, TSST-1, the wreckage). Students who can sort a new virulence factor into "disguise, tool, or wreckage" can usually guess its clinical effect even if they've forgotten the name.
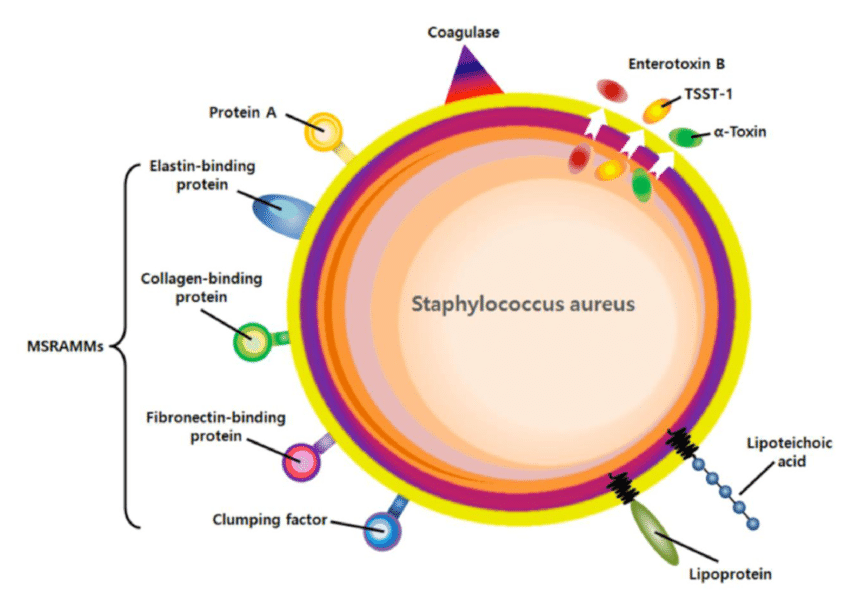
1. Surface and structural factors (adhesion, immune evasion)
- Capsule: inhibits phagocytosis, promotes adherence to host cells and prosthetic devices. Clinical link: why catheter and implant infections are so hard to clear.
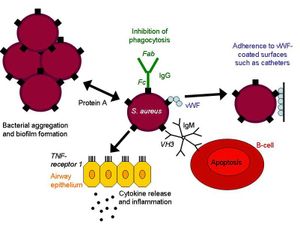
- Protein A: binds the Fc region of immunoglobulin, making S. aureus invisible to opsonins and resistant to phagocytic killing. Clinical link: a major reason infections recur even with an intact antibody response.
 - Teichoic acid (lipoteichoic and wall teichoic acid): mediates adhesion, colonization, and biofilm formation; D-alanine residues confer resistance to defensins and to vancomycin/teicoplanin. Clinical link: connects directly to why biofilm-associated device infections are vancomycin-tolerant even without classical resistance genes.
- Teichoic acid (lipoteichoic and wall teichoic acid): mediates adhesion, colonization, and biofilm formation; D-alanine residues confer resistance to defensins and to vancomycin/teicoplanin. Clinical link: connects directly to why biofilm-associated device infections are vancomycin-tolerant even without classical resistance genes.
- Fibronectin-binding proteins (FnBPA, FnBPB): drive biofilm formation, particularly in MRSA strains.
- Clumping factor: the basis of the slide coagulase test (see Lab Diagnosis below, this is the same molecule the bedside test detects).
2. Toxins (tissue and immune damage)
- Hemolysins (α, β, γ, δ): lyse red blood cells, produce the hemolysis pattern seen on Blood Agar.
- Panton-Valentine Leukocidin (PVL): pore-forming toxin that destroys neutrophils. Clinical link: associated with severe necrotizing skin infections and necrotizing pneumonia, especially community-acquired MRSA.
- Enterotoxins (A-E, heat-stable): survive cooking temperatures. Clinical link: this is why staph food poisoning has a rapid onset (1-6 hours), the toxin is already preformed in the food, the bacteria don't need to multiply in the gut.
- Exfoliative toxins (ETA, ETB): serine proteases that cleave desmoglein and split desmosomes in the epidermis. Clinical link: directly produces Staphylococcal Scalded Skin Syndrome, mainly in infants and young children.
- TSST-1 (superantigen): triggers massive, non-specific T-cell activation and cytokine release. Clinical link: classically tied to tampon-associated toxic shock syndrome, though any TSST-1-producing focus can trigger it.
3. Enzymes (spread and persistence)
- Coagulase: clots plasma by activating prothrombin-like conversion of fibrinogen to fibrin, walls the organism off in a fibrin layer that resists phagocytosis. Clinical link: the biological reason S. aureus tends to form a localized abscess rather than spreading diffusely, and the basis of the coagulase test used to identify it.
- Staphylokinase: breaks down the fibrin clot the organism just made, allowing spread to adjacent tissue once local conditions favor it.
- Hyaluronidase: hydrolyzes hyaluronic acid in connective tissue, facilitating spread.
- DNase: degrades DNA, used as a confirmatory identification test (see below).
- Lipase: hydrolyzes lipids, helps the organism survive in sebaceous skin areas, relevant to why it favors hair follicles and sebaceous glands as infection sites.
- Catalase: breaks down hydrogen peroxide, blunting the oxidative burst neutrophils use to kill it. Clinical link: same enzyme the catalase test detects, this is genuinely a virulence factor and a diagnostic marker at once.
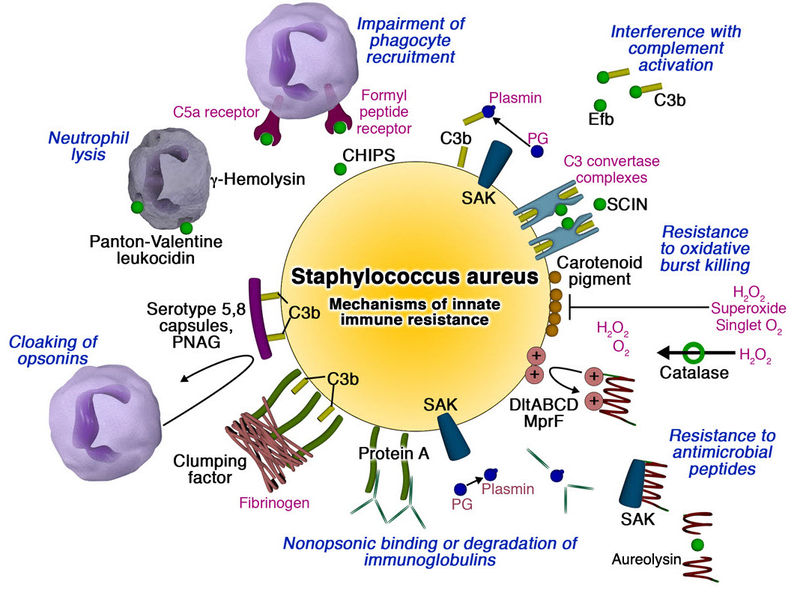 Figure: Mechanisms by which S.aureus subverts innate immune defenses
Figure: Mechanisms by which S.aureus subverts innate immune defenses
How to Remember the Virulence Factors of Staphylococcus aureus
To remember these virulence factors; remember this: every successful infection has to hide, hit, and spread.
Hide (surface and structural factors). Capsule and Protein A work like a burglar's disguise. Protein A binds antibodies backward, by the tail end instead of the business end, so the antibody can't flag the bacterium for destruction. It's a fake ID that fools the immune system's checkpoint.
Hit (toxins). These are the weapons. Hemolysins crack open red cells the way a burglar cracks a safe. PVL is aimed specifically at neutrophils, the building's security guards, disabling them before they can respond. Exfoliative toxin works like a crowbar between floor tiles, prying apart desmosomes between skin cells, which is exactly why SSSS produces sheets of peeling skin rather than a localized rash. TSST-1 doesn't pick one lock quietly, it sets off every alarm in the building at once, a massive non-specific cytokine storm instead of a targeted response.
Spread (enzymes). Coagulase builds a fibrin barricade around the bacterium, that barricade is the abscess you see clinically, walling the infection into one spot. Staphylokinase is the same burglar later tearing down their own barricade to move to the next room, which is why a contained boil can progress to spreading cellulitis. Hyaluronidase is the crowbar through the walls between rooms, the connective tissue, letting infection travel faster once it's ready to move.
Laboratory diagnosis
- Gram staining: Gram-positive cocci in clusters, may appear singly, in pairs, or short chains.
- Culture
- Blood Agar: abundant growth in 18-24 hours, yellow to golden-yellow colonies, with or without beta hemolysis.
- Mannitol Salt Agar (MSA): selective and differential medium. S. aureus ferments mannitol, producing yellow colonies after 24-48 hours at 35°C.
- Biochemical tests:
- Catalase test: Positive (the same enzyme described above that blunts the neutrophil oxidative burst)
- Coagulase test: Positive, distinguishes S. aureus from coagulase-negative staphylococci (CoNS). (detects the same fibrin-walling enzyme described above). CoNS are further separated by novobiocin susceptibility, S. epidermidis is sensitive, S. saprophyticus is resistant.
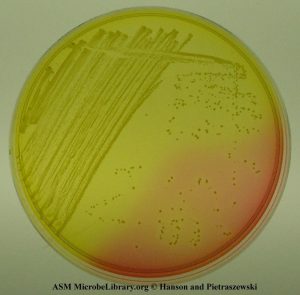 Figure: Yellow colonies of S. aureus in Mannitol Salt Agar (Photo by Anne Hanson and Matthew Pietraszewski, University of Maine)
Figure: Yellow colonies of S. aureus in Mannitol Salt Agar (Photo by Anne Hanson and Matthew Pietraszewski, University of Maine)
Biochemical tests for the identification of S. aureus
| Name of the test | Staphylococcus aureus | Notes |
|---|---|---|
| Catalase test | Positive | To differentiate staphylococci from streptococci. |
| Hemolysis | β-hemolysis or non-hemolysis | |
| Coagulase test | Positive | To differentiate S. aureus from CONS. |
| Mannitol fermentation | Yes | To differentiate S. aureus (fermenter) from CONS (non-fermenter) |
| Furazolidone disk Test | Sensitive | To differentiate staphylococci from micrococci (resistant) |
| Polymyxin B sensitivity test | Resistant | Most staphylococcal species are susceptible to polymyxin B, but S. aureus, S. lugdunensis, and S. epidermidis are resistant. |
| Bacitracin( 0.04-U disk) susceptibility test | Resistant | To separate staphylococci from micrococci (susceptible) |
| Microdase test | Negative | To differentiate staphylococci from micrococci. |
| DNase test | Positive | To differentiate S.aureus from other Staphylococci (-ve) when coagulase test is unavailable. |
Where students actually get confused
- Slide coagulase negative does not always mean CoNS. The slide test detects bound coagulase (clumping factor) only. A small number of S. aureus strains produce free coagulase but little or no bound coagulase, giving a false-negative slide result. Always confirm a negative slide test with the tube coagulase test before calling something CoNS.
- MSA yellow colonies are not proof of S. aureus. Some CoNS, particularly S. saprophyticus, can weakly ferment mannitol given enough incubation time. MSA narrows the field, it doesn't replace coagulase confirmation.
- DNase is a backup, not a substitute. It's useful when coagulase reagent isn't available, but a few CoNS species (notably S. lugdunensis) are also DNase-positive, so a positive DNase result alone shouldn't override a negative coagulase.
- Catalase-positive does not mean Staphylococcus. Micrococcus is catalase-positive too. Catalase only separates staphylococci from streptococci, not staphylococci from micrococci, that distinction needs bacitracin, furazolidone, or the microdase test.
Antimicrobial Resistance
Staphylococcus aureus, including Methicillin-resistant Staphylococcus aureus(MRSA), is one of the most common causes of healthcare-associated infections. The first report of Vancomycin-Resistant Staphylococcus aureus(VRSA) came in 2002. VRSA is also resistant to methicillin and other classes of antibiotics, limiting the available treatment options.
Key exam facts in one table
| Feature | S. aureus | Memory hook |
|---|---|---|
| Gram stain | Gram-positive cocci, clusters | Staphyle is Greek for "bunch of grapes," the name describes the morphology |
| Catalase | Positive | Bubbles when H2O2 is added, that's the test, and the same enzyme protecting it from neutrophils |
| Coagulase | Positive | Builds its own barricade (clot) around itself |
| Mannitol fermentation | Positive | Turns MSA yellow, the same gold that "aureus" (Latin for golden) describes |
| Key abscess-forming enzyme | Coagulase | The "hide" step |
| Key immune-evasion factor | Protein A | A fake ID that fools the immune system |
| Key food-poisoning factor | Preformed heat-stable enterotoxin | Already cooked in, reheating the food won't save you |
| Key SSSS factor | Exfoliative toxin (ETA/ETB) | Pries skin layers apart |
| Key TSS factor | TSST-1 (superantigen) | Sets off every alarm at once, instead of picking one lock |
Self-check questions
- Why does a slide coagulase-negative result not rule out S. aureus, and what's the next step?
- A 6-month-old presents with widespread skin peeling but no organisms cultured from the affected skin. What toxin explains this, and why is culture from the lesion itself often negative?
- Why does staphylococcal food poisoning have a much faster onset than Salmonella gastroenteritis?
- Name the enzyme responsible for the same biological process that the tube coagulase test detects in the lab.
- A catalase-positive, Gram-positive coccus turns out resistant to bacitracin and furazolidone. What organism are you now suspecting, and why doesn't catalase alone settle it?
References
- Forbes, S., Sahm, D. F., & Weissfeld, A. S. (2002). Bailey & Scott’s Diagnostic Microbiology. Mosby.
- Foster, T. (1996). Staphylococcus. In S. Baron (Ed.), Medical Microbiology. (4th ed.). University of Texas Medical Branch at Galveston.
- Tong, S. Y., Davis, J. S., Eichenberger, E., Holland, T. L., & Fowler, V. G., Jr (2015). Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clinical microbiology reviews, 28(3), 603–661. https://doi.org/10.1128/CMR.00134-14
Frequently Asked Questions
What is the difference between Staphylococcus aureus and coagulase-negative staphylococci?
Why is Staphylococcus aureus catalase-positive but Streptococcus is catalase-negative?
Can Staphylococcus aureus be part of normal flora?
What is the difference between MRSA and regular Staphylococcus aureus?
Why does Staphylococcus aureus form abscesses while Streptococcus pyogenes spreads more diffusely?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.