Antigen-Antibody Reactions: Types, Stages, and How Each Is Used
The full framework of antigen-antibody reactions: the three stages of binding, and the main reaction types (agglutination, precipitation, complement fixation, neutralization, and labeled immunoassays), with what each detects and where it is used.
An antigen-antibody reaction is the specific binding of an antibody to the antigen that stimulated its production. This single interaction is the basis of both the body's humoral defense and almost every serological test in the diagnostic laboratory. The reaction can be made to reveal itself in many ways, as clumping, as a visible precipitate, as the consumption of complement, as the blocking of a toxin, or as a fluorescent or colored signal, and each of those visible outcomes is the basis of a different family of tests. This article is the map of that landscape: the stages every antigen-antibody reaction passes through, the main reaction types, and what each one is used to detect. Each type links to a dedicated article for its full method.
An antigen-antibody reaction, also known as an antibody-antigen interaction or antigen-antibody binding, is a specific molecular interaction between an antigen and an antibody. Antigens are molecules or molecular structures often found on the surface of pathogens like bacteria, viruses, and other foreign substances, as well as on the surface of cells in the body. Antibodies or immunoglobulins are Y-shaped proteins formed by the immune system as a response to the presence of antigens.
General feature of antigen-antibody reactions
- The reaction is specific; an antigen combines only with its homologous antibody and vice versa. The specificity however is not absolute and cross-reactions may occur due to antigenic similarity or relatedness.
- Whole antibody and antigen molecules take part in the reaction under normal conditions, though isolated antibody fragments (Fab) also retain antigen-binding ability.
- There is no denaturation of the antigen or the antibody during the reaction.
- The combination occurs at the surface, therefore it is the surface antigens that are immunologically relevant.
- The binding is non-covalent and therefore reversible. It is held by hydrogen bonds, ionic bonds, hydrophobic interactions, and van der Waals forces rather than covalent bonds, and its strength is described by affinity and avidity. Reversibility matters in practice: it is what allows bound antibody to be eluted from red cells, and it is why binding strength, not permanence, is what determines whether a reaction becomes visible.
The strength of the interaction is measured as affinity (the fit between a single epitope and paratope) and avidity (the combined strength of all binding sites acting together). For a full treatment, see affinity vs avidity. - Antigens and antibodies can combine in varying proportions, unlike chemicals with fixed valencies. Both antigens and antibodies are multivalent, antibodies are generally bivalent, though IgM molecules may have five or ten combining sites. Antigens may have valencies up to hundreds.
The three stages of an antigen-antibody reaction
Every antigen-antibody reaction passes through the same sequence, and different tests simply read it at different points.
Primary stage. The initial binding of antigen to antibody. It is rapid, reversible, and held by non-covalent forces. On its own it is invisible; specialized labeled techniques (immunofluorescence, ELISA, radioimmunoassay) are needed to detect binding at this stage.
Secondary stage. The bound complexes build into something visible: clumping (agglutination), an insoluble mass (precipitation), complement consumption (complement fixation), or loss of biological activity (neutralization). Most classical serological tests read the secondary stage. Note that the binding is still non-covalent here; the reaction becomes visible because many complexes aggregate into a lattice, not because the bonds change nature.
Tertiary stage. The in-vivo consequences of binding: neutralization of toxins, enhanced phagocytosis, cell lysis, and both protective immunity and immunopathology (allergy, immune-complex disease).
Prozone Phenomenon
At high antibody concentrations, the number of antibody binding sites may greatly exceed the number of epitopes present in the antigens. As a result, most antibodies bind antigen only univalent instead of multivalently. Antibodies that bind univalent can not cross-link one antigen to another.
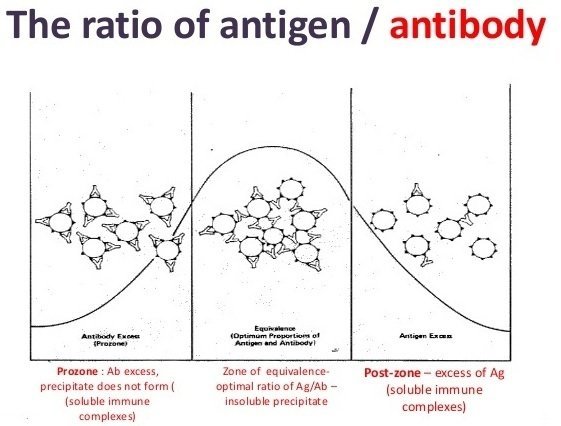 Figure: Prozone phenomenon -
Figure: Prozone phenomenon -
Prozone effects are readily diagnosed by performing the assay at a variety of antibody ( or antigen) concentrations. As one dilutes to an optimum antibody concentration, one sees higher levels of agglutination. When using polyclonal antibodies incomplete antibodies also cause a prozone effect.
The mirror situation, antigen excess, is called the postzone, and it too can suppress a visible reaction. Both are why serological tests are run across a dilution series rather than at a single concentration. The zone of optimal proportions between them is the equivalence zone.
Types of antigen-antibody reactions
 Fig: Tube agglutination test for the determination of antibody titer
Fig: Tube agglutination test for the determination of antibody titer
Agglutination
Antibody cross-links particle-bound antigen (bacteria, red cells, or antigen-coated latex beads) into visible clumps. It is more sensitive than precipitation for detecting antibody, and it is read by eye without instruments. Slide, tube, latex, coagglutination, hemagglutination, and inhibition formats each have their place. For the full taxonomy and clinical examples, see Agglutination test types. Specific applications have their own articles: Widal test, Coombs test, and the treponemal TPHA.
 Figure: Widal Test: Sample showing H positive in screening test
Figure: Widal Test: Sample showing H positive in screening test
Precipitation
When a soluble antigen combines with antibody in optimal proportions, the complexes grow into an insoluble, visible precipitate. Precipitation is most efficient at the zone of equivalence, where antigen and antibody are balanced. It underlies immunodiffusion (Ouchterlony, radial immunodiffusion) and electrophoretic methods such as counterimmunoelectrophoresis (CIE).
Complement fixation
Some antigen-antibody complexes bind (fix) complement. This is exploited in the complement fixation test, where consumption of complement by a test reaction is revealed by the absence of lysis in an indicator system. See Complement fixation test.
Neutralization
Antibody binds an antigen in a way that blocks its biological activity, neutralizing the toxicity of a toxin or the infectivity of a virus. This is the basis of toxin-neutralization and virus-neutralization assays. See Neutralization test (virus and toxins).
Labeled immunoassays
Attaching a detectable label to antibody or antigen makes even primary-stage binding visible. The label may be a fluorophore (immunofluorescence), an enzyme (ELISA), or a radioisotope (radioimmunoassay). See Immunofluorescence assay and ELISA.
How to Remember
Two devices for the two things the hub is meant to lock in.
Three stages, three visibilities. Primary binding is invisible (you need a label to see it, so labeled assays live here). Secondary binding is visible as clumps or precipitates (classical serology lives here). Tertiary is what happens in the body (protection and immunopathology). Match the stage to how you would detect it.
The reaction type is named for what you see. Clump = agglutination. Insoluble mass = precipitation. Complement used up = complement fixation. Activity blocked = neutralization. Glow or color = labeled immunoassay. Name the visible outcome and you have named the reaction type.
Key exam facts in one table
| Point | What to remember |
|---|---|
| Binding forces | Non-covalent: hydrogen, ionic, hydrophobic, van der Waals |
| Reversibility | The binding is reversible (not covalent, not permanent) |
| Specificity | High, but not absolute; cross-reaction occurs with related antigens |
| Affinity vs avidity | Affinity = single-site fit; avidity = combined strength of all sites (see dedicated article) |
| Primary stage | Invisible binding; detected only by labeled assays (IFA, ELISA, RIA) |
| Secondary stage | Visible: agglutination, precipitation, complement fixation, neutralization |
| Tertiary stage | In-vivo effects: neutralization, opsonization, lysis, immunopathology |
| Agglutination | Particle-bound antigen clumps; more sensitive than precipitation for antibody |
| Precipitation | Soluble antigen forms insoluble mass; best at equivalence |
| Prozone | Antibody excess blocks visible reaction → false negative |
| Postzone | Antigen excess blocks visible reaction → false negative |
| Equivalence | Optimal antigen:antibody proportions; maximal visible reaction |
Where students get confused
"Antigen-antibody binding is irreversible." It is not. The binding is non-covalent and reversible. What looks permanent is a large, stable lattice of many complexes, but each individual bond can form and break. This reversibility is exactly what elution techniques exploit.
"The secondary stage uses covalent bonds because it's stable." A common textbook error. The bonds are non-covalent at every stage. The secondary stage is visible because complexes aggregate into a lattice, not because the chemistry changes.
"Agglutination and precipitation are basically the same." Both are the antigen-antibody lattice becoming visible, but agglutination needs a particulate antigen (or one coated on a particle) and precipitation needs a soluble antigen. Agglutination is also generally more sensitive for detecting small amounts of antibody.
"A stronger reaction always means more antibody." Antibody excess (prozone) can suppress a visible reaction, and antigen excess (postzone) does the same. Maximal reaction occurs at equivalence, in the middle, which is why serology is read across dilutions.
References
- Levinson, W. (2020). Review of Medical Microbiology and Immunology (16th ed.). McGraw-Hill.
- Tille, P. M. (2022). Bailey & Scott's Diagnostic Microbiology (15th ed.). Elsevier.
- Procop, G. W., et al. (2017). Koneman's Color Atlas and Textbook of Diagnostic Microbiology (7th ed.). Wolters Kluwer.
- Murphy, K., & Weaver, C. (2016). Janeway's Immunobiology (9th ed.). Garland Science.
Frequently Asked Questions
What is an antigen-antibody reaction?
Is antigen-antibody binding reversible?
What are the three stages of an antigen-antibody reaction?
What is the difference between agglutination and precipitation?
What is the prozone phenomenon?
What are the main types of antigen-antibody reactions?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.