Scrub typhus: Overview, Pathogenesis and Lab Diagnosis
Scrub typhus: Overview, Pathogenesis and Lab Diagnosis
Scrub typhus also known as bush typhus, is an emerging infectious disease caused by a bacteria Orientia tsutsugamushi (formerly known as Rickettsia tsutsugamushi). It is a zoonotic disease primarily affecting rodents, rabbits, and marsupials. Humans are accidental hosts.
Transmission
Scrub typhus infection is transmitted to humans through the bite of infected Leptotombidiummite larvae (chiggers) that are found in grasslands, forests, bush areas, woodpiles, gardens, and beaches. The mites are both the vector and the natural reservoir for O. tsutsugamushi.
Transmission is also possible through unscreened blood transfusions and unhygienic needles. However, there is no person-to-person transmission.
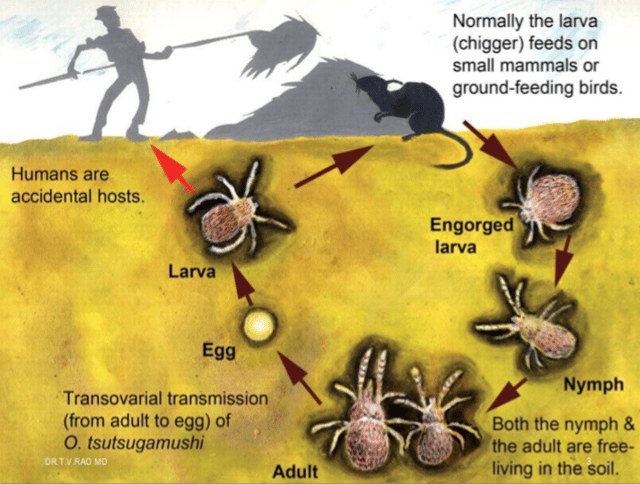 Figure: Life cycle of mite and transmission dynamics of Orientia
Figure: Life cycle of mite and transmission dynamics of Orientia
Risk groups for Scrub Typhus: It affects people of all ages including children. The risk of infection is higher in person undertaking outdoor activities (such as visiting farms, camping, backpacking, hunting, archeological digs) as there is a high chance of getting bitten by chiggers.
Pathogenesis and clinical manifestations
 Figure: Eschar at site of chigger bite (Imagesource)
Figure: Eschar at site of chigger bite (Imagesource)
Human infection is initiated via the bite of an infected larval Leptotrombidium mite (also known as a chigger). The incubation period ranges from 6 to 21 days (usually, 10–12 days). Disease onset is characterized by fever, headache, myalgia, cough, and gastrointestinal symptoms. The severity of the symptoms varies widely, depending on the susceptibility of the host, the virulence of the bacterial strain, or both.
Scrub typhus is clinically diagnosed by the development of an eschar at the bite site. The eschar starts as a small papule that enlarges and subsequently undergoes central necrosis to turn black. An eschar usually occurs at sites where skin surfaces meet or clothes bind, such as the axilla, groin, neck, waist, and inguinal area.
From the second week of onset, if untreated, patients show evidence of systemic infection. This stage of illness can attack different organ systems such as the
- central nervous system (acute diffuse encephalomyelitis, encephalopathy, meningitis, deafness, cranial nerve palsies, eye manifestations)
- cardiovascular system (rhythm abnormalities, myocardial involvement with congestive heart failure, vasculitis),
- renal system (acute renal failure),
- respiratory system (Interstitial pneumonia and acute respiratory distress syndrome) and
- gastrointestinal system (alterations in liver functions, pancreatitis, diarrhea). Sometimes multiorgan dysfunction syndrome (MODS) occurs with an increased case-fatality if not treated promptly.
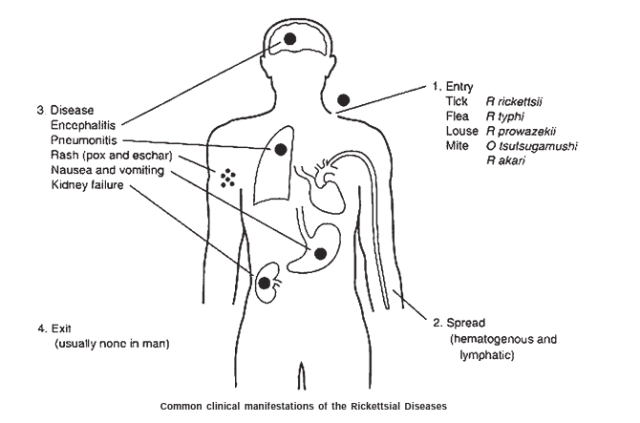 Figure: Common Clinical Manifestations of Rickettsial Diseases
Figure: Common Clinical Manifestations of Rickettsial Diseases
Laboratory Diagnosis
Early diagnosis of acute scrub typhus infection is important for appropriate patient management.
Specimens: Skin or lymph node biopsy, Heparinized blood, EDTA blood, Serum
Methods available include
A) Direct methods like isolation of the pathogen in cell cultures and detection of scrub typhus-specific DNA by polymerase chain reaction (PCR).
B) Indirect methods include detection of antibodies to O. tsutsugamushi by immunofluorescence assay (IFA), enzyme-linked immunosorbent assay (ELISA) and rapid diagnostic assays.
Direct Methods
- Isolation of pathogen: O. tsutsugamushi can be isolated on cell monolayers (such as HeLa, L929, Vero, and BHK21) but requires biosafety level-3 facilities. The median time for positivity is 27 days. As it is more labor-intensive, requires special lab facilities, and treatment cannot be delayed, this method is not appropriate for the routine diagnosis of scrub typhus but is useful for research purposes in reference laboratories.
- Polymerase Chain Reaction (PCR) Techniques: PCR is advantageous as it can detect the disease before antibodies become detectable by serological methods and thus ensures conformity and early diagnosis. It is targeted to detect scrub typhus-specific DNA like 56 kDa, 47 kDa, 16S ribosomal RNA, and GroEL gene targets. Though PCR is highly sensitive and specific in detecting very low numbers of copies, the cost factor prevents its use in routine diagnosis in endemic areas
Indirect Methods
Indirect methods include serological tests that are the mainstay for the diagnosis of scrub typhus and are most commonly employed. After primary infection, IgM antibody appears significantly by the end of the first week whereas IgG antibodies usually take around two weeks to appear at significant levels.
Indirect Immunofluorescent Antibody (IFA)
It is based on the principle of fluorescence-labeled anti-human immunoglobulin and detects antibodies in the serum of the infected patient. The test is positive when the fluorescence-labeled anti-human immunoglobulin binds to the immobilized bacterial antigen that has been placed on a slide.
**Advantages:**It is advantageous as it can use any serotype (Karp, Kato, and Gilliam) as an antigen and can measure either IgG or IgM individually.
Limitations:
- Its main limitation is it can be stated positively only when paired sera demonstrate a fourfold rise in titer or seroconversion. As paired sera are seldom available, a single cutoff titer for IFA, ELISA, and rapid diagnostic tests can be used for diagnosis, provided the baseline cut-off in the population has been determined.
- Also, it requires fluorescence microscopy, which is very labor-intensive, and require trained human resource.
This test was considered the gold standard for the diagnosis of scrub typhus but is currently under review due to its limitations.
Indirect Immunoperoxidase (IIP)
Immunoperoxidase assay is similar to IFA with the only substitution of fluorescein with peroxidase-labeled antibodies and diagnosis can be made without a fluorescent microscope. IIP methods have shown results that are equivalent to IFA. However, the sensitivity of this test is influenced by the various strains (as in IFA) and its subjective readings make it inferior to other serological methods such as ELISA.
Enzyme-linked Immunoabsorbent Assays (ELISA)
Currently, it is the preferred method of choice for serological diagnosis in acute scrub typhus infection. It uses a recombinant p56-kDa type-specific antigen of O. tsutsugamushi strains that combine with IgM antibodies produced against all the strains of scrub typhus. ELISA, is advantageous as it can be automated and thus used to screen large numbers of sera, is objective (optical density value), economical, technically simpler, and able to detect antibody levels also.
Immunochromatographic Tests (ICT)
This is a rapid diagnostic point-of-care test that utilizes recombinant 56-kDa TSA of only the common subgroups (Karp, Kato, and Gilliam) and results in a wide range of sensitivities and specificities in the detection of IgM antibodies.
Weil Felix Reaction
It is an agglutination method for the detection of rickettsial infection in the patient’s serum samples. It is the oldest test in current use which utilizes the detection of host immune response against different Proteus antigens such as OX19, OXK, and OX2 that cross-respond with rickettsiae. It is inexpensive, easy to perform, and results are available overnight; however, it lacks specificity and sensitivity.
Chances of false-positive results are also very high in the case of Proteus infection of the urinary tract, leptospirosis, and relapsing fever. So negative Weil–Felix test results did not exclude scrub typhus and required a further diagnosis for confirmation. Despite lower specificity, Weil–Felix is still performed in laboratories for initial screening of the scrub typhus in rural areas.
Other Clinical Tests
Other tests such as Cerebrospinal Fluid (CSF) evaluation and chest radiographs can be done for patients with signs of scrub meningitis and respiratory symptoms respectively. CSF evaluation shows lymphocytic pleocytosis while chest radiograph may show pleural effusions
Prevention and treatment
- Tetracyclines (doxycycline) and chloramphenicol are drugs of choice and are effective in both oral and intravenous forms against scrub typhus.
- Azithromycin is also an excellent alternative, particularly when resistance to doxycycline is suspected.
- Rifampicin is also used as a second-line treatment option, but with a risk of inducing drug-resistant tuberculosis, it is only given after no active tuberculosis is ruled out.
- No vaccine against scrub typhus is yet available. Therefore, prevention is based mainly on avoiding the arthropod bite.
References and Further Readings
- Scrub Typhus: Clinical, Pathologic, and Imaging Findings. Yeon Joo Jeong, Suk Kim, Yeh Dae Wook, Jun Woo Lee, Kun-Il Kim, and Sun Hee Lee. RadioGraphics. 2007 27:1, 161-172
- Scrub Typhus.Centers for Disease Control and Prevention
- Scrub Typhus. State Pearls
- Scrub typhus: pathophysiology, clinical manifestations and prognosis. Senaka Rajapakse, Chaturaka Rodrigo, Deepika Fernando, Asian Pacific Journal of Tropical Medicine, 2012 5 (4), 261-264
- Orientia tsutsugamushi(Scrub Typhus). Antimicrobe, Infectious Disease Antimicrobial Agents.

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.