Borrelia species: Properties, Pathogenesis, Lab Diagnosis
Borrelia species: Properties, Pathogenesis, Lab Diagnosis
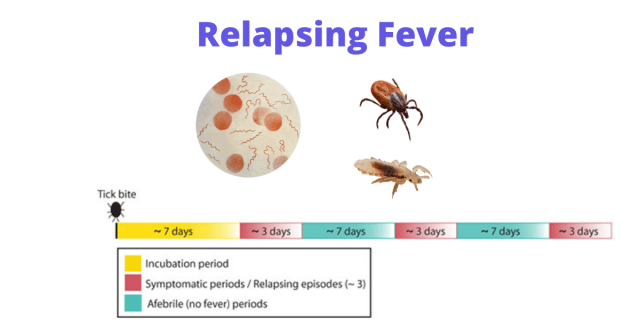
Relapsing fever is a bacterial infection characterized by recurrent episodes of fever and nonspecific symptoms following exposure to insect vector-carrying Borrelia species.
 There are two main types of relapsing fever:
There are two main types of relapsing fever:
- Epidemic relapsing fever also known as Louse-borne relapsing fever (LBRF) is caused by B. recurrentis and transmitted by a louse. LBRF outbreaks most commonly occur in conditions of overcrowding and social disruption. Note: epidemic typhus is also louse-borne typhus.
- Endemic relapsing fever also known as Tick-borne relapsing fever (TBRF) is caused by Borrelia species other than B. recurrentis such as B. duttoni, B. hermsiiand *B. turicatae.It is transmitted by a tick.
Borrelia miyamotoi disease (sometimes called hard tick relapsing fever) is another newer type of relapsing fever which is now getting increased attentions.
Pathogenesis
Mode of transmission:
- Epidemic relapsing fever: Human-human transmission occurs by the body louse (Pediculus humanus).Borreliae are introduced by crushing of the louse (e.g. by scratching) leading to deposition of insect’s infected hemolymph containing numerous spirochetes on the abraded skin and mucous membranes.
- Endemic relapsing fever: It is transmitted by bite of an infected tick (Ornithodoros species).
From the inoculated site, Borrelia spreads rapidly leading to bacteremia and fever. Host’s immune system tries to eliminate the bacilli from the body.
However, the borrelial surface antigens frequently undergo antigenic variation. Each time, new antigens are produced which can evade host’s immune system leading to repeated bacteremia and recurrent febrile episodes.
Difference between Epidemic and Endemic relapsing fever
| Character | Epidemic relapsing fever (louse-borne) | Endemic relapsing fever (tick-borne) |
|---|---|---|
| Agent | B. recurrentis | B. duttoni, B. hermsii |
| Epidemiology | Epidemic | Usually endemic |
| Natural host | Humans | Rodents |
| Vector | Pediculus humanus spp . | Various; Ornithodoros hermsii, O. turicatae, O.parkeri in USA |
| Distribution | East Africa (Sudan and Ethiopia) | North America, Central Asia, and Africa |
| Hemorrhage, CNS features | More common | Less common |
| Treatment | Doxycycline-single-dose | Doxycycline for 1 week. |
Both epidemic and endemic relapsing fever have similar manifestations although not identical. Incubation period is about 7-8 days.
Recurrent febrile episodes lasting for 3-5 days occur intervening with afebrile periods for 7-9 days. Subsequent episodes are shorter
Non-specific symptoms may be present like alteration of sensorium, abdominal pain, vomiting and diarrhea.
Hemorrhages: Petechiae, epistaxis, and blood-tinged sputum are more likely in epidemic RF.
Neurologic features such as meningitis, seizure, focal deficits, paraplegia and psychosis may occur in 10-30% of cases and are more common in epidemic RF.
Laboratory Diagnosis
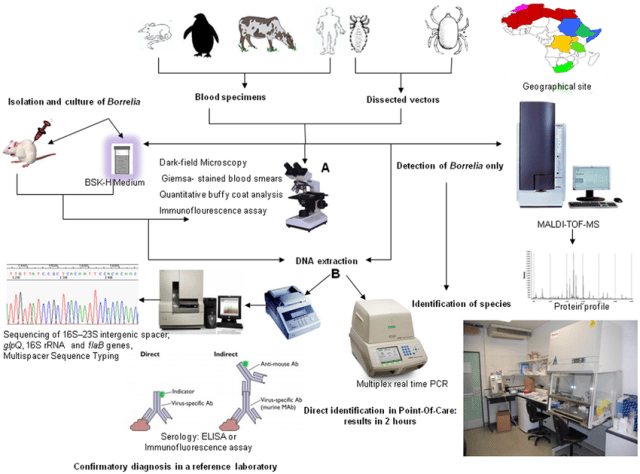 Figure: Approaches for the diagnosis of Relapsing fever (Image source: Aurélien Fotso Fotso and Michel Drancourt)
Figure: Approaches for the diagnosis of Relapsing fever (Image source: Aurélien Fotso Fotso and Michel Drancourt)
Microscopy
- Peripheral thick or thin smear-stained by Wright or Giemsa stain
- Direct fluorescent antibody test using monoclonal antibody aids in species identification.
- Dark ground microscope (low sensitivity).
- Quantitative buffy coat (QBC) analysis is an alternative method with higher sensitivity.
- It is poorly gram-negative
Microscopy and Staining
Detection of the spirochetes in the blood of the patient during the febrile illness. In contrast to other spirochetes the relapsing fever borreliae are well stained by acid aniline dyes, such as Wright’s or Giemsa’s stains.
The borrelial spirochetes are thin, undulant, or overtly spiral organisms that are most visible when they are located between RBCs. Thick and thin films should be made as for malaria, because in some cases spirochetes will be detected only by examination of the thick film.
Culture
During the afebrile period, microscopy fails to detect Borrelia; hence, the confirmation is made by isolation of Borrelia from blood. Animal pathogenicity testing can be done by intraperitoneal inoculation into white mice.
Serology
ELISA and IFA (indirect fluorescence assay) are available to detect serum antibodies. A fourfold rise in antibody titer between acute and convalescent serum samples or with a single convalescent serum sample that is reactive. However, false-positive results may occur in other spirochete infections.
An IFA titer of 1:128 to 1:256 or higher is considered positive. However, only a few reference laboratories perform serology for the diagnosis of this infection because the borreliae need to be cultivated to use in an indirect IFA.
GIpQ assay: It is the most reliable serological method. It is an immunoblot assay detecting antibody against the recombinant GlpQ antigen (glycerophosphodiester phosphodiesterase).
Molecular methods
Multiplex Real-time PCR has been developed targeting 16SrRNA, flagellar B protein (flaB), gyrase B (gyrB) and GlpQ genes to identify the various species of Borrelia.
References and further readings
- Fotso, Aurélien & Drancourt, Michel. (2015).Laboratory Diagnosis of Tick-Borne African Relapsing Fevers: Latest Developments. Frontiers in Public Health. 3. 10.3389/fpubh.2015.00254.
- Color Atlas and Textbook of Diagnostic Microbiology, Koneman, 5th edition

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.