Malaria RDTs: Principle, Procedure, Results, and Limitations (Including HRP-2 Deletion
Learn how malaria rapid diagnostic tests work, how to interpret T1/T2/C line results, and the critical limitation of HRP-2 gene-deleted P. falciparum strains — with exam questions.
A community health worker in a remote district of Nepal sees a febrile child at 2 a.m. The nearest microscopy-equipped lab is four hours away. She runs a malaria RDT using a finger-prick blood sample. In 15 minutes, she has an answer — and can start treatment or refer immediately without waiting for microscopy. This is the promise of the malaria RDT: bringing parasite-confirmed diagnosis to the last mile.
But RDTs are not infallible. Understanding what they detect, what they miss, and why a positive or negative result still requires microscopy confirmation is essential for any clinician or laboratory scientist working in malaria-endemic settings.
Some antigens (e.g. pLDH-parasite Lactate dehydrogenase or Aldolase ) are produced by all malarial species but some antigens (HRP2-histidine-rich protein-2) are produced by a single species of malarial parasite. RDTs offer the potential to provide accurate and timely diagnosis, reaching those previously unable to access good quality microscopy services. The RDT works through the lateral flow or Immunochromatographic strip method and notifies the presence of antigens by acolor change/formation of bands on an absorbing nitrocellulose strip.
RDTs give results in about15 minutes, so a patient with malaria can begin treatment right away. There is no need to wait for microscope results.
The RDT test kits come in many formats:
- Card
- Dipstick
- Hybrid cassette-dipsticks
- Plastic cassette
The three main groups of antigens detected by commercially available RDTs are:
- Histidine-rich protein 2 (HRP-2), specific to P. falciparum. It is an abundant soluble, heat-stable antigen in the cytoplasm and membrane of infected erytocytes.
- Parasite-specific plasmodium lactate dehydrogenase (pLDH), currently available as P. falciparum specific, pan-specific, and P. vivax-specific.
- Aldolase (pan-specific). These two antigens are conserved major enzymes in the glycolytic pathway of malaria parasites, they are abundant and are soluble in the parasite.
Note: Pan-specific means that the RDT detects all four types of plasmodia that infect humans.
PRINCIPLE
RDTs for detecting malaria antigens are based on the immunochromatographic test principle. These RDTs capture parasite antigens from peripheral blood using monoclonal antibodies prepared against a target malarial antigen and conjugated to gold particles in a mobile phase. The test area contains an immobilized monoclonal antibody, which captures the Ag-Ab complex giving a visible line.
If malaria antigen is present in the blood sample, Ag-Ab complex will be formed as it combines with the labeled pan-specific antibody present in the mobile phase. This Ag-Ab complex will migrate along the test strips, which will be captured by the specific antibodies present in the immobile phase (here T1 contains monoclonal antibodies specific to P.falciparum i.e. HRP2 antigen and T2 contains plasmodium pan-specific antibody i.e. pLDH) thus producing a visible colored line. Control line containsgoat anti-mouse antibody and ensures that the system is controlled for migration.
Malaria antigens currently targeted by RDT are HRP-2, pLDH, and Plasmodium aldolase.
HRP-2 : HRP-2 is a water-soluble protein produced by asexual stages and young gametocytes of Plasmodium falciparum. It is expressed on the RBC membrane surface, and because of its abundance in P.falciparum, it is the first antigen to be used to develop an RDT for its detection.
pLDH and aldolase: pLDH, an enzyme found in the glycolytic pathway of the malaria parasite, is produced by sexual and asexual stages of the parasite. Different isomers of pLDH for each of the four Plasmodium spp. infecting humans exist, and their detection constitutes a second approach to RDT development. Several other enzymes of the malaria parasite glycolytic pathway, notably aldolase have been suggested as target antigens for RDT for species other than Plasmodium falciparum.
Materials Required
- New unopened test packet
- New unopened alcohol swab
- New unopened lancet
- New pair of disposable gloves
- Buffer
- Timer
- Sharps box
- Pencil or pen.
Test Instructions
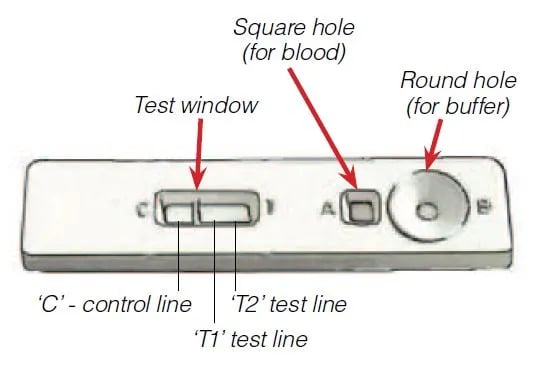 Figure: RDT
Figure: RDT
- Check the expiry date on the test packet.
- Put on gloves. Use new gloves for each patient.
- Open the test kit packet and remove, test pad, capillary tube and desiccant sachet.
- Write the patient’s name on the test.
- Open the alcohol swab. Grasp the 4th finger on the patient’s left hand. Clean the finger with the alcohol swab. Allow the finger to dry before pricking.
- Open the lancet. Prick patient’s finger to get a drop of blood. Do not allow the tip of the lancet to touch anything before pricking the patient’s finger.
- Discard the lancet in the Sharps Box immediately after pricking finger. Do not set the lancet down before discarding it.
- Use the capillary tube to collect the drop of blood.
- Use the capillary tube to put the drop of blood into the square hole marked “A”.
- Discard the capillary tube in the Sharps Box.
- Add buffer into the round hole marked “B”.
- Wait for 15 minutes after adding buffer.
- Read the results (see below)
- Dispose of the gloves, alcohol swab, desiccant sachet and packaging in a non-sharps waster container.
- Record the test results in your register. Dispose of cassette in non-sharps waste container.
Interpretation of the test results
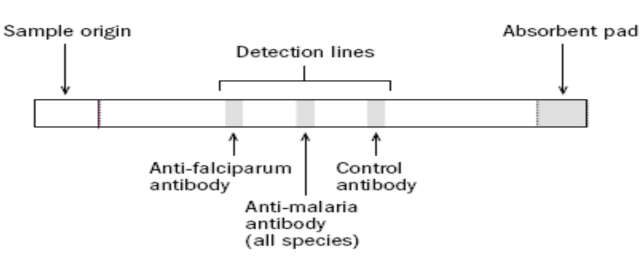 Figure: RDTs for lab diagnosis of Malaria
Figure: RDTs for lab diagnosis of Malaria
In the Kit we are using, ‘T1’ test line is specific for P. falciparum, ‘T2‘ test line is Pan-specific and ‘C‘ is the control line.
 Figure: Malaria RDT Test One
Figure: Malaria RDT Test One
A line in ‘T1‘ and a line in ‘C’ means the patient DOES have falciparum malaria. The test is POSITIVE even if the line in‘T1‘ is very faint.
A line in ‘T2’and a line in ‘C’ means the patient DOES have non-falciparum malaria (P. vivax, P. ovale, P. malariae) or a mixed infection of these.
Lines in ‘T1‘ and ‘T2’ and a line in ‘C’ means the patient DOES have falciparum malaria mono-infection or a mixed infection.
4. NO Line in ‘T1’ or ‘T2’ and a line in ‘C’ means the patient DOES NOT have either falciparum malaria or non-falciparum malaria.
5.NO Line in‘T1‘ or ‘T2’ and NO LINE in ‘C’ means the test is damaged. Results are INVALID.
6. Line in ‘T1’ or ‘T2′ and NO LINE in ‘C’ means the test is damaged. Results are INVALID.
 Figure: Malaria RDT Test Two
Figure: Malaria RDT Test Two
Advantage of Rapid Diagnostic test for Malaria diagnosis
High-quality malaria microscopy is not always available in every clinical setting where patients might seek medical attention. The laboratories associated with these health care settings may now use an RDT to more rapidly determine if their patients are infected with malaria.
- RDTs can provide a parasite-based diagnosis in places where microscopy is not possible or practical.
- RDTs can be used to distinguish fevers caused by malaria parasites from those caused by other illnesses, such as meningitis and acute respiratory infection (that cause symptom similar to malaria). RDTs can thus help to target anti-malarial treatment (ACTs) to patients who really have malaria. When RDTs show that a febrile patient does not have malaria, that patient is more likely to seek diagnosis and treatment for the illness he/she does have.
- It helps to avoid unnecessary use of ACTs on patients who do not have malaria. This will help to prevent or delay drug resistance, making ACTs effective for a longer period.
- Relatively easy (with minimal training required) and rapid (giving timely results)
- Little or no manipulation of sample required, can be performed in places without laboratories
- Most of the RDTs do not require refrigeration, hence tests can be performed where there is no power supply
- Uses whole blood (prick or venous blood prick preferred)
Limitation of Rapid Diagnostic test for Malaria diagnosis
- RDTs cannot test how many malaria parasites are present in the blood. They can only test whether parasites are present or absent (qualitative result only). Any quantification of parasitemia will require further laboratory tests.
- RDTs that detect malaria antigen, Histidine-rich protein 2 or ‘HRP2’ can not be used to check for effectiveness of treatment, because this antigen can remain in the blood for at least two weeks after the parasites are killed by drugs. Other malaria antigens, pLDH, and aldolase disappear from the blood rapidly, so RDTs based on those antigens will usually be negative a few days after effective treatment.
- Costs per test may exceed those of microscopy.
- Short shelf-life, requiring efficient procurement, transportation, storage, and distribution systems
- Intensity of test band varies with the amount of antigen present at low parasite densities-this may lead to reader variation in test results.
- In many cases, they are less sensitive (and less specific) than laboratory-based tests. The RDT may not be able to detect some infections with a lower number of malaria parasites circulating in the patient’s bloodstream.
- The use of the RDT does not eliminate the need for malaria microscopy. All negative RDT must be followed by microscopy to confirm the result. In addition, all positive RDT’s should also be followed by microscopy.
Microscopy is needed to determine the species of malaria detected by the RDT. Microscopy (thick and thin blood smear) is needed to quantify the proportion of infected RBCs, which is an important prognostic indicator.
Critical Limitation: HRP-2 Gene Deletion in P. falciparum
This is the most significant emerging limitation of HRP-2-based RDTs and is now examined in postgraduate microbiology and parasitology courses.
P. falciparum strains with deletions of the pfhrp2 gene (and sometimes the related pfhrp3 gene) do not produce HRP-2 antigen. An RDT that relies solely on HRP-2 detection will return a false-negative result for these strains — the patient has falciparum malaria, but the RDT shows negative.
This is not a hypothetical problem. WHO surveillance has confirmed pfhrp2-deleted strains across multiple countries, with particularly high prevalence in:
- Parts of the Amazon basin (Peru, Brazil, Colombia)
- East Africa (Eritrea, Ethiopia)
- South Asia (reports from India)
Clinical consequence: In areas with high pfhrp2 deletion frequency, an HRP-2-based RDT cannot be relied upon to rule out P. falciparum. WHO recommends:
- Using combination RDTs that detect both HRP-2 and pLDH (which is not gene-deleted)
- Following all negative RDTs with microscopy when clinical suspicion is high
- Ongoing surveillance for pfhrp2 deletion in endemic regions
Exam note: If a question describes a febrile patient with peripheral travel history and a negative HRP-2 RDT but a positive blood smear showing P. falciparum — pfhrp2 gene deletion is the explanation.
Where Students Actually Get Confused
1. "A negative RDT means no malaria." No. All negative RDTs should be followed by microscopy if clinical suspicion remains. Low-level parasitaemia may be below the detection threshold of the RDT (typically 100–200 parasites/μL). Additionally, pfhrp2-deleted strains will test negative on HRP-2 RDTs despite active infection.
2. "A positive HRP-2 RDT confirms active falciparum malaria." Not quite. HRP-2 persists in blood for up to 2–4 weeks after successful treatment. A positive HRP-2 result may reflect cleared infection rather than active disease. This is why pLDH-based results are more useful for treatment monitoring — pLDH disappears within days of parasite clearance.
3. "RDT can replace microscopy." No — RDT and microscopy are complementary, not interchangeable. Microscopy is still required to: (a) quantify parasitaemia (prognostic indicator for severe disease), (b) identify species when RDT gives an ambiguous result, (c) confirm negative RDTs with high clinical suspicion.
4. "T2 line positive means non-falciparum." T2 detects pan-specific antigen (pLDH). If only T2 is positive (with C), it means non-falciparum malaria OR a mixed infection where the falciparum load is too low to trigger T1. Always confirm species by microscopy.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Three RDT antigen targets | HRP-2, pLDH, Aldolase | HRP-2 = falciparum only; pLDH + aldolase = all species |
| HRP-2 specificity | P. falciparum only | "H for falciparum" |
| pLDH specificity | Pan-specific (all Plasmodium spp.) or species-specific isoforms | pLDH = Pan-specific Lactate DeHydrogenase |
| RDT result time | 15 minutes | Fastest field tool |
| HRP-2 persistence after treatment | Up to 2–4 weeks | Cannot use HRP-2 RDT for treatment monitoring |
| pLDH after treatment | Clears within days | Use pLDH-based RDT for treatment monitoring |
| pfhrp2 gene deletion | P. falciparum strains lacking HRP-2 gene → false-negative HRP-2 RDT | WHO surveillance confirmed in Amazon, East Africa, South Asia |
| Detection threshold | ~100–200 parasites/μL (variable by brand) | Low parasitaemia may be missed |
| RDT after negative result | Must confirm with microscopy | Negative RDT ≠ no malaria |
| T1 line = | P. falciparum (HRP-2 target) | T1 = falciparum |
| T2 line = | Pan-specific (pLDH target) | T2 = any species |
| Invalid result | No C line regardless of T1/T2 | No control = no result |
Self-check questions
- A patient treated for P. falciparum malaria 10 days ago is now afebrile. An HRP-2 RDT is still positive. Does this mean treatment has failed?
- A traveller returning from the Peruvian Amazon has fever and a negative HRP-2 RDT. Blood smear shows ring forms. What is the most likely explanation?
- Which malaria RDT antigen is most appropriate for monitoring treatment response, and why?
- What does a result of T1 positive + T2 positive + C positive indicate?
- Why must all negative RDTs be followed by microscopy?
Answers:
- Not necessarily — HRP-2 persists for up to 4 weeks after treatment. pLDH-based RDT or blood smear would be more informative.
- pfhrp2 gene deletion — the P. falciparum strain lacks the HRP-2 gene; HRP-2 RDT cannot detect it.
- pLDH — it disappears from blood within days of parasite clearance, reflecting current parasite burden.
- P. falciparum monoinfection or mixed infection with non-falciparum species.
- Low-level parasitaemia may be below RDT threshold; pfhrp2-deleted strains give false-negatives; clinical judgment requires both tools.)
References and further reading
- Sastry, A. S., & Bhat, S. (2014). Essentials of Medical Parasitology. Jaypee Brothers Medical Publishers.
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- Wongsrichanalai, C., Barcus, M. J., Muth, S., Sutamihardja, A., & Wernsdorfer, W. H. (2007). A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT). American Journal of Tropical Medicine and Hygiene, 77(6 Suppl), 119–127. https://www.ncbi.nlm.nih.gov/books/NBK1695/
- Bell, D., Wongsrichanalai, C., & Barnwell, J. W. (2006). Ensuring quality and access for malaria diagnosis: how can it be achieved? Nature Reviews Microbiology, 4(9 Suppl), S7–S20. https://doi.org/10.1038/nrmicro1525
- World Health Organization. (2023). Guidelines for malaria. WHO. https://www.who.int/publications/i/item/guidelines-for-malaria
- World Health Organization. (2023). Response plan to pfhrp2 gene deletions (2nd ed.). WHO. https://www.who.int/publications/i/item/9789240101838
- Cheng, Q., Gatton, M. L., Barnwell, J., et al. (2014). Plasmodium falciparum parasites lacking histidine-rich protein 2 and 3: a review and recommendations for accurate reporting. Malaria Journal, 13, 283. https://doi.org/10.1186/1475-2875-13-283
- Kozycki, C. T., Umulisa, N., Rulisa, S., et al. (2017). False-negative malaria rapid diagnostic tests in Rwanda: impact of Plasmodium falciparum isolates lacking hrp2 and declining malaria transmission. Malaria Journal, 16, 123. https://doi.org/10.1186/s12936-017-1771-3
- Mouatcho, J. C., & Goldring, J. P. D. (2013). Malaria rapid diagnostic tests: challenges and prospects. Journal of Medical Microbiology, 62(10), 1491–1505. https://doi.org/10.1099/jmm.0.052506-0
Frequently Asked Questions
What antigens do malaria RDTs detect?
Can a malaria RDT be used to monitor treatment response?
What is pfhrp2 gene deletion and why does it matter?
What does it mean if only the control line (C) appears on a malaria RDT?
What does an invalid malaria RDT result look like?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.