Hypersensitivity Type IV: Mechanism and Clinical Manifestation
Hypersensitivity Type IV: Mechanism and Clinical Manifestation
Hypersensitivity is a body’s response to a particular substance in an exaggerated way, which does not happen in normal cases. Hypersensitivity type IV is different from the rest of the other types of hypersensitivity as it is cell-mediated and delayed-type hypersensitivity. Unlike other types, it involves the interaction of T cells; therefore, it is not antibody-mediated. Since this process takes more time than reactions involving antibodies, a type IV reaction can be referred to as a delayed-type hypersensitivity reaction (DTH).
In DTH, the overreaction of the helper T cells (TH) and overproduction of cytokines damage tissues and cause inflammation and cell death. DTH responses can manifest from contact with allergens or infectious agents, where T lymphocytes have had prior encounters with antigen, giving rise to localized inflammation, erythema, and edema. Although DTH is detrimental, in some cases, the response plays an essential role in defense against intracellular pathogens and contact antigens.
History
Robert Koch first observed DTH. He observed such reactions in individuals infected with Mycobacterium tuberculosis. The patients developed a localized inflammatory response when injected intradermally with a filtrate derived from a mycobacterial culture. And he called this localized skin reaction a “tuberculin reaction.” Later on, other antigens were also found to induce such responses.
Mechanism
DTH reaction occurs in the initial sensitization phase and the effector phase.
Initial phase/ Sensitization phase
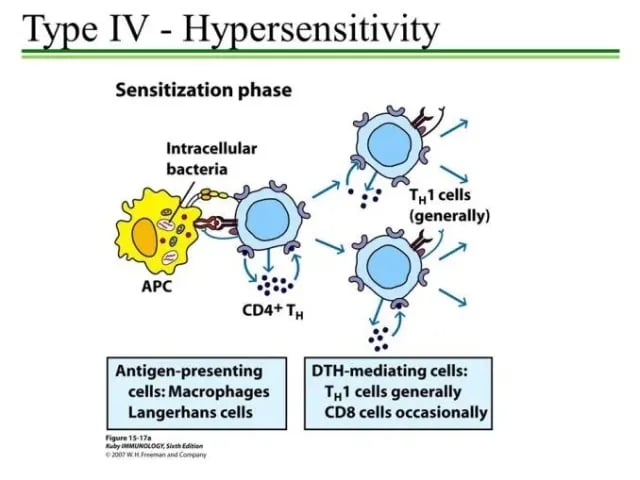 Figure: Type IV Hypersensitivity (Sensitization Phase)
Figure: Type IV Hypersensitivity (Sensitization Phase)
The reaction begins when a foreign antigen is engulfed by antigen-presenting cells (APC). The antigen is expressed in a complex with the MHC-II on the surface of APC. It is recognized by the T helper cell.
Here, APC may be Langerhans (dendritic cells found in the epidermis) and macrophages or vascular endothelial cells. They pick antigens from the skin to regional lymph nodes, where the antigen activates T cells.
Now activated TH cells secrete autocratic cytokines, which help them clonally expand, i.e., TH cells proliferate and differentiate into the TH1 subpopulation.
T helper cells are the primary cells activated during the DTH response’s sensitizing phase (mostly TH1 and TH17). However, in some cases, Cytotoxic T cells are also found to induce a DTH response.
The antigens involved may be either intracellular pathogens or contact antigens. These are actually peptides derived from intracellular bacteria or contact antigens. Some of them are listed in the following table:
Table: Intracellular pathogens and contact antigens inducing DTH. Source: Kuby Immunology
| Antigens | Examples |
|---|---|
| Intracellular bacteria | Mycobacteria um tuberculosis, M. leprae, Listeria monocytogenes, Brucella abortus |
| Intracellular fungi | Pneumocystis carinii, Candida albican, Histoplasma capsulatum, Cryptococcus neoformans |
| Intracellular parasites | Leishmania sp. |
| Intracellular viruses | Herpes simplex virus, Variola (smallpox), Measles virus |
| Contact antigens | Picrylchloride, hair dyes, nickel salts, poison ivy, and poison oak |
The duration of the initial sensitization phase is 1 to 2 weeks after primary contact with an antigen.
Effector phase
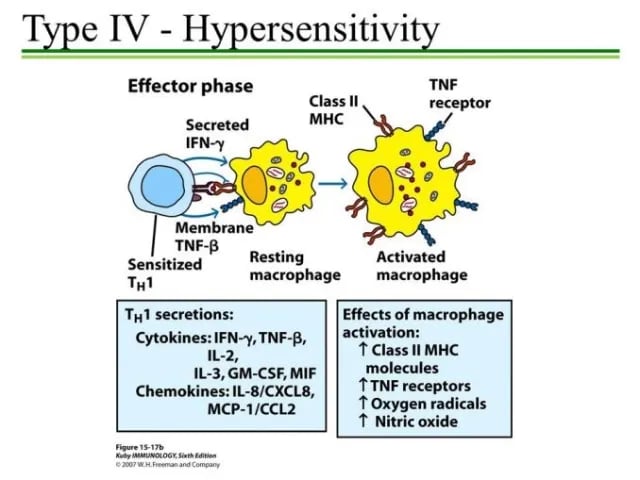 Figure: Type IV Hypersensitivity (Effector Phase)
Figure: Type IV Hypersensitivity (Effector Phase)
Macrophages are the principal effector cells of the DTH response. After a second or subsequent exposure of sensitized TH1 cells to antigen, TH1 cells secrete various cytokines and chemokines. These factors attract and activate macrophages and other non-specific inflammatory cells. Activated macrophages are more effective in presenting antigens.
The reaction occurs not before 24 hours after the second exposure with the antigen (generally, 48 to 72 hours). It is because cytokines require time to induce localized influxes of macrophages and their activation.
Generally, this process kills pathogens rapidly with little tissue damage. However, in some cases, significantly, if the antigen is not quickly cleared, a prolonged DTH response can become destructive to the host. It may lead to a visible granulomatous reaction due to intensive and chronic inflammation.
Cytokines such as IL-2 and interferon-gamma induce the further release of other TH1 cytokines. This mediates the immune response activating macrophages and other non-specific inflammatory cells. Activated CD8+ T cells destroy target cells on contact, whereas activated macrophages produce hydrolytic enzymes and transform into multinucleated giant cells on presentation with specific intracellular pathogens.
The T cells involved in type IV reactions are memory cells derived from prior stimulation by the same antigen. These cells persist for months or years. When T cells are restimulated by the antigen presented on the surface of the APC, the T cells secrete cytokines that recruit and activate lymphocytes and phagocytic cells, which carry out the cell-mediated immune response.
Clinical manifestation
A broad range of inflammatory pathologies takes place. Erythema and edema, granuloma formation, fibrosis, and tissue necrosis can occur as the effect of DTH.
DTH reactions are prominent in autoimmune diseases and have also been demonstrated to play a role in response to transplantation. Some of the adverse effects are listed below:
- Tuberculin reaction
- Contact dermatitis
It occurs after sensitization to simple environmental chemicals, like Urushiol (e.g., nickel, formaldehyde), plant materials (poison ivy), cosmetics, soaps, and other substances. Small molecules enter the skin and act as haptens attach to body proteins which induce cell-mediated hypersensitivity, particularly in the skin. On subsequent exposure to the agent, the sensitized person develops erythema, itching, vesication, eczema, or skin necrosis within 12-48 hours. - Granuloma
A granuloma develops when continuous activation of macrophages induces the fusion of macrophages to form multinucleated giant cells. These giant cells displace normal cells forming palpable nodules and releasing a high concentration of lytic enzymes, destroying surrounding tissues and necrosis. Lungs: Tuberculosis, hypersensitivity pneumonitis, granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis). - Transplant rejection
The host immune system may reject tissue transplantation from a genetically different donor (allogeneic transplantation). This is also because of DTH. - Type 1 diabetes mellitus
Type I diabetes mellitus, or insulin-dependent diabetes mellitus, is caused by DTH. Infiltrates of lymphocytes and macrophages are found in islets of Langerhans in the pancreas. Such cells destroy insulin-producing Beta cells resulting the insulin deficiency. - Others
Multiple sclerosis is an autoimmune disease of the CNS where TH cells react against a self-myelin antigen. Inflammation of the thyroid gland Leprosy
Diagnosis
Some general investigations may be necessary depending on the different types of diseases. Basic routine investigations may include looking at blood, liver, thyroid, and kidney functions.
Control
Usually, DTH causes no life-threatening conditions. And also, there is no specific cure for this type of reaction. Thus, the treatment aims for symptom control only.
- Allergen avoidance can be a preventive measure in contact dermatitis.
- Steroids like prednisolone and dexamethasone can make the condition better.
- Type IV hypersensitivity can usually be resolved with topical corticosteroids.
- Drugs must be taken under specialist supervision. Drugs like interferon, cyclophosphamide, cyclosporine, etc. are used.
References
- Kindt et al.(2007). Kuby Immunology. W. H. Freeman and Company. 6th edition.
- Abbas et al.(2007). Cellular and Molecular Immunology. Saunders, Elsevier. 6th edition.
- www.britannica.com/science/immune-system-disorder/Type-IV-hypersensitivity
- healthinfo.healthengine.com.au/hypersensitivity-reaction-type-iv
- Hwang SA & Actor JK (2015). Hypersensitivity: T Lymphocyte Mediated (Type IV). Wiley Online Library. https://doi.org/10.1002/9780470015902.a0001139.pub3

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.