Hypersensitivity Reactions: an Overview
Hypersensitivity Reactions: an Overview
Hypersensitivity refers to an exaggerated or unnecessary reaction produced by the host immune system. It is an immunological dysfunction, mainly targeted at innocuous antigens with consequent tissue damage.
The human immune system protects body from damage by fighting invasive substances and infections. Sometimes, however, it can ‘overreact,’ identifying harmless substances as harmful, which causes undesirable consequences. This is called a hypersensitivity response.
Hypersensitivity reactions include allergies and autoimmune diseases. Exogenous substances cause allergies, whereas endogenous substances cause autoimmune disorders in sensitive individuals. Sometimes, the term allergy is used to explain hypersensitivity. However, these are different terms. Allergies are signs and symptoms, but hypersensitivity reaction is an immunological process in the body. Certain types of hypersensitivity reactions show an allergy (mainly type I reactions) in response to exogenous (and harmless) antigens.
The symptomatic reaction only occurs in sensitized individuals, i.e., must have had at least one prior asymptomatic contact with the offending antigen.
Classification of Hypersensitivity Reactions
The human body shows different types of hypersensitivity reactions, depending on the antigen a person has exposure to and how the body responds to it.
Historically hypersensitivity was divided on a time basis into immediate and delayed reactions. Generally, quick response develops in less than 24 hours, and delayed reaction develops within 24-48 hours.
However, the most popular classification is Coombs and Gell’s classification. This was given in 1963, which classifies hypersensitivity into four different types. Each type differs based on the antigen type the body identifies, the kind of host immune response, or how quick the response is.
Type I, II, and III are antibody-dependent and immediate reactions, whereas type IV is antibody-independent and has delayed response.
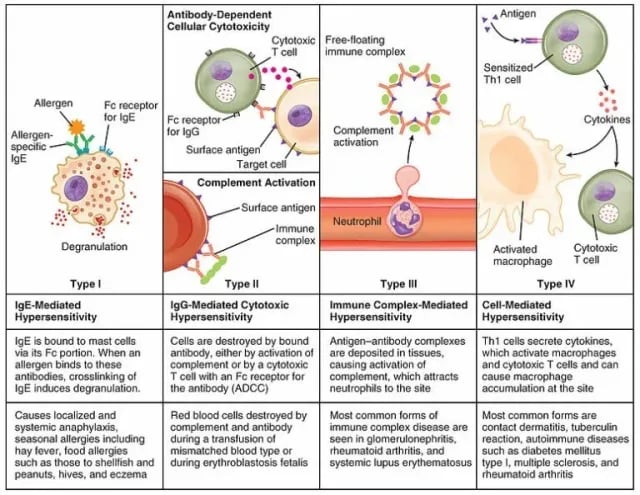 Figure: Different types of hypersensitivity
Figure: Different types of hypersensitivity
Type I Hypersensitivity
Type I hypersensitivity or allergy is the most common immune disorder. It is also known as an immediate or anaphylactic hypersensitivity reaction. The reaction usually takes 15-30 minutes from the time of exposure to the allergen (antigen), but sometimes, delayed onset (10-12 hours) can be seen.
The initial introduction of an antigen (or an allergen) produces IgE response. Cross-linking of IgE with sensitized cells ultimately leads to release of mediators like histamine, leukotriends, and prostagladins causing widespread vasodilation, bronchoconstriction, and increased permeability of vascular endothelium.
Read more about mechanism of Type I hypersensitivity
The reaction affects the skin, eyes, nasopharynx, and gastrointestinal tract. The response may be systemic or local, and the reaction may cause a range of symptoms from minor inconvenience to death. Examples of type I hypersensitivity reactions are anaphylaxis, food allergy, asthma, allergic conditions of rhinitis, and conjunctivitis.
Type II Hypersensitivity
Type II hypersensitivity reactions are cytotoxic and may affect a variety of organs and tissue. The antigens usually are endogenous, although exogenous chemicals (haptens) which can attach to cell membranes can also lead to type II hypersensitivity. Thus, type II hypersensitivity reactions may occur in response to host cells (i.e., autoimmune) or non-self cells, as in blood transfusion reactions. Type II reactions are antibody-mediated. IgG or IgM antibodies are involved, targeting antigens on cell surfaces.
Type II hypersensitivity can lead to tissue damage by three main mechanisms.
- Antibody and complement-mediated destruction
- ADCC(Antibody-Dependent Cell-Mediated Cytotoxicity) and
- Target cell dysfunction
Read more about Type II hypersensitivity mechanism here
Type II hypersensitivity reactions include newborns’ hemolytic disease, Graves disease, Myasthenia gravis, blood transfusion reaction, and Goodpasture syndrome.
Type III Hypersensitivity
This is caused by antigen-antibody complex or immune complex. The response may be the pathogenic mechanism of diseases caused by many microorganisms. These can deposit in capillaries or joints and trigger inflammation if not eliminated.
The reaction occurs 3-10 hours after exposure. Mainly, IgG antibodies are involved in the response. However, IgM antibodies are also applied.
Read more about the mechanism of Type III hypersensitivity here
Localized reactions like Arthus reaction, farmer’s lung disease, rheumatoid arthritis, systemic reactions like serum sickness, and systemic lupus erythematosus are examples of type III hypersensitivity reactions.
Type II is distinguished from type III by the location of the antigens. In type II, cell-bound antigens are involved, whereas in type III, antigens are soluble.
Type IV Hypersensitivity
Type IV hypersensitivity reactions are also called delayed-type hypersensitivity (DTH), as response starts only after 24 to 72 hours. The reaction takes longer than all other types because of the time required to recruit cells to the exposure site.
Unlike other types, it is a cell-mediated hypersensitivity reaction. Antigen-specific activated T-cells mediate it.
Read more about the mechanism of Type IV hypersensitivity here.
Transplant rejection, granuloma, contact dermatitis, tuberculin reaction, Multiple sclerosis, insulin-dependent diabetes mellitus.
Different types of hypersensitivity reactions can be summarized in the following table:
| Type | Name of Hypersensitivity | Main actor | Time of response | Reaction | Associated Diseases/adverse Reactions |
|---|---|---|---|---|---|
| I | Anaphylactic hypersensitivity | IgE antibody | Immediate (minutes) | Mast cell activation releases histamines and other mediators | AnaphylaxisAsthmaAtopy |
| II | Antibody-dependent hypersensitivity | Antibodies IgM and IgG,ComplementMAC | Hours to days | Antigens embedded in host cells cause complement activation and destruction by MAC. | Hemolytic anemiaRheumatic heart diseaseThrombocytopeniaErythroblastosis fetalisGraves’ disease |
| III | Immune complex-mediated hypersensitivity | IgG antibody,Complement,Neutrophils | Hours to days/weeks | Antibody binds to soluble antigens, forming a circulating immune complex deposits in a vessel wall and causes a local inflammatory response. | Serum sicknessRheumatoid arthritisArthus reactionPost streptococcal glomerulonephritisReactive arthritisSystemic lupus erythematosis |
| IV | Delayed or cell- Mediated hypersensitivity | T cells | Delayed (24 to 72 hours) | APC activates TH1/CTL. T cells activate macrophages and cause a local inflammatory response. | Contact dermatitisMantoux testTransplant rejection |
Diagnosis
Diagnosis of hypersensitivity reactions is based on symptoms, personal history, and medical records. Laboratory findings of blood, urine, imaging, allergic skin test, biopsy or culture, liver, and kidney function tests, TSH and TFT, etc. are carried out depending on the nature of the disease and hypersensitivity types.
Type I, II, and III are antibody-mediated, and their clinical features can overlap. In such a case, differential diagnosis is necessary.
In type I reaction, the diagnosis is primarily based on the association of antigen exposure to clinical manifestations, such as fever, arthritis, and rash. Physical examination, in addition to IgE level in serum and allergy tests, is performed.
Diagnosis of type II reaction includes the detection of circulating antibodies against the tissue involved and the presence of antibodies and complement in the lesion (biopsy) by immunofluorescence. Coombs test is done in transfusion reaction and anemia. Pregnancy history is required to diagnose erythroblastosis fetalis; ultrasound, fetal laboratory test, and maternal antibody tests are performed. In rheumatoid arthritis, CRP, ASO, and ESR are performed. Diagnosis tests in vivo include delayed cutaneous reactions (e.g., manteaux test in type IV hypersensitivity reactions).
Management and control
The first and most important way of minimizing hypersensitivity reactions is finding out the cause and eliminating or avoiding it. If it is impossible, one can follow treatment procedures to reduce the risks. Such reactions are treated according to the symptoms and diseases. Some of the measures are listed below:
- Removal of the offending agent
- Reviewing the drug allergy list and related side effects for patients
- Use of immunotherapy and immunosuppressive drugs in autoimmune conditions or in hypersensitivity reactions, under the supervision of a specialist.
- Rapid cessation of transfusion, and supportive care in case of blood transfusion reaction
- Use of humanized or genetically engineered antibodies instead of antibodies from animal origin.
References
- Hypersensitivity reactions – knowledge @ amboss. ambossIcon. (n.d.). Retrieved November 9, 2022, from https://www.amboss.com/us/knowledge/Hypersensitivity_reactions/
- Basu S, Banik BK (2018) Hypersensitivity: An Overview. Immunol Curr Res 2: 105.https://www.omicsonline.org/open-access/hypersensitivity-an-overview-105371.html
- Momtazmanesh S & Rezaei N (2022). Encyclopedia of Infection and Immunity.www.sciencedirect.com/topics/medicine-and-dentistry/hypersensitivity
- Speller J (2022). Hypersensitivity reactions: TeachMe Physiology https://teachmephysiology.com/immune-system/immune-responses/hypersensitivity-reactions/

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.