Hepatitis B Virus: Structure, Replication, and Pathogenesis Explained
How HBV's overlapping genes drive chronic infection, why HBcAg never shows up in blood tests, and what makes some carriers infectious for life.
A neonate develops yellowish eyes and skin a month after birth. Screening confirms hepatitis B infection, almost certainly transmitted from the mother during delivery. The family wants to know two things: how did this happen despite the baby seeming healthy at birth, and is this a passing illness or something the child will carry for life?
The honest answer is: it depends far less on the virus than on the baby's own immune system, and that's a strange thing for a virus to leave up to chance. HBV doesn't directly destroy liver cells the way many cytopathic viruses do; the liver damage you see in hepatitis B is largely collateral damage from the host's own cytotoxic T cells trying to clear infected hepatocytes. A strong T-cell response wins the fight and clears the virus, often at the cost of a rough acute illness. A weak response, far more common in neonates and infants whose immune systems haven't matured yet, fails to clear the infection at all, and the virus simply persists, quietly replicating in liver cells the immune system never mounted a real attack against.
This is why a hepatitis B-positive mother's newborn receives both HBIg and vaccine starting at birth, covered later in this article's Prevention and Control section, the goal is to hand the infant ready-made antibodies and a head start on active immunity before that fragile window of weak T-cell defense ever gets tested by the live virus. And it's why understanding the virus's structure matters clinically at all: a genome built to replicate efficiently and persist quietly inside the very cells meant to clear it is what makes chronic carriage, cirrhosis, and hepatocellular carcinoma possible decades later in survivors of exactly this kind of neonatal infection.
Structure of HBV
- Small (approx. 3.2 kb) in size.
- Enveloped.
- The genome is partially double-stranded DNA as its positive strand is incomplete. The negative-strand consists of 4 genes; S, C, P, and X. S gene codes HBsAg and HBeAg, P codes for DNA polymerase with reverse transcriptase activity, and X codes for X-protein that regulates transcription. Similarly, the C gene codes for capsid or core proteins.
- Under an electron microscope, three particles of HBV appear in the serum of patients; spherical (22 nm diameter), filamentous or tubular, and spherical, double-walled with 42 nm diameter, commonly known as Dane particle.
- Nucleocapsids surround the DNA. Proteins like HBV core protein (HBcAg) attached to the genome are also enclosed by nucleocapsid, whereas the virus’s envelope consists of HBsAg and HBeAg.
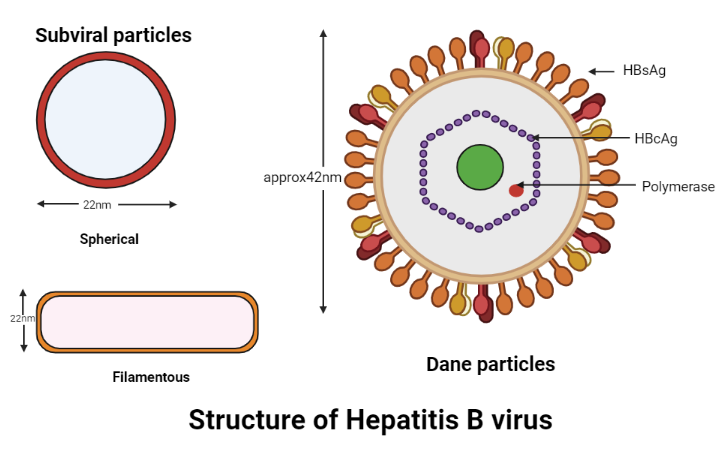 Figure: Structure of hepatitis B virus
Figure: Structure of hepatitis B virus
HBsAg Composition
HBsAg consists of three glycoproteins, S, L, and M, all encoded by the same gene. The S glycoprotein is the major component of HBsAg, which self-associates into 22-nm spherical particles released from the cells. The filamentous particles of HBsAg in the serum contain a large amount of S and only a tiny amount of L and M glycoprotein and other proteins and lipids. The glycoprotein L is essential for virion assembly and formation of filamentous particles, and retention of the structures in the cell.
Genomic arrangements
- The genome of HBV is circular DNA, approximately 3,200 base pairs in length.
- It is capable of independent replication.
- The genetic arrangement of HBV has two distinct features; proteins encoded from overlapping frames and all regulatory sequences residing in protein-encoding sequences.
- The genome has four open reading frames (ORFs). These codes represent the genes that code nucleocapsid protein (core), an envelope protein (s), replicase protein (polymerase), and a protein involved in virus gene expression (X).
- The ORFs, as mentioned above, overlap; it is a distinct feature of the Hepatitis B virus that helps in encoding 50% (in mass) more unique protein than other DNA viruses.
- Unlike other viruses, the cis-acting regulatory elements are found inside the coding genes themselves instead of in the non-coding section.
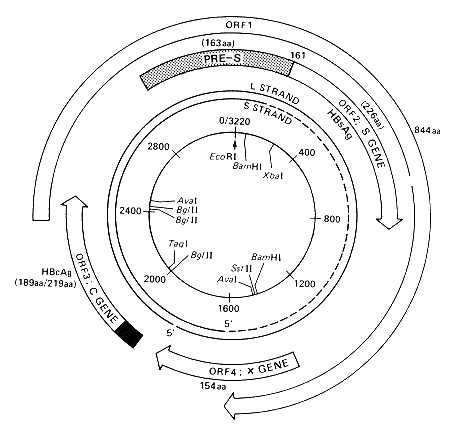 Figure: Source:Abbas, Naaz & Arshad, Yousra & Shakoori, Abdul. (2006). Mutations in the hepatitis B virus core gene and its efficacy as a vaccine – A Review.. Proc. Pakistan Congr. Zool. 26. 103-129.
Figure: Source:Abbas, Naaz & Arshad, Yousra & Shakoori, Abdul. (2006). Mutations in the hepatitis B virus core gene and its efficacy as a vaccine – A Review.. Proc. Pakistan Congr. Zool. 26. 103-129.
How to Remember
Four overlapping genes, one compact genome, and a reason for the compression. Think of HBV's genome as a sentence written so that words share letters: S (surface), C (core), P (polymerase), and X (transcription regulator) genes physically overlap on the same circular DNA strand. Why would a virus evolve such a cramped, overlapping arrangement instead of just having a slightly bigger genome with separate genes? A smaller genome packages faster, fits inside a smaller, more stable particle, and is cheaper to replicate, real advantages for a virus that needs to produce huge numbers of progeny inside a single hepatocyte. The overlap is the price paid for that compactness, and it's also why a single point mutation in HBV can simultaneously affect two different proteins at once, since the same stretch of DNA is doing double duty.
Subtypes and genotypes, two different filing systems, because they answer different questions. Subtypes (ADW, ADR, AYW, AYR) are based on HBsAg's antigenic determinants (d/y and w/r), think of these as the virus's "ID badge," useful for serology and vaccine cross-reactivity. Genotypes (A through H) are based on the genome's actual DNA sequence, the virus's "genetic family tree," useful for tracking geographic spread and predicting disease course. A single virus has one genotype but is classified into one of the four subtype combinations based on what its surface antigen looks like, the two systems exist because clinicians and epidemiologists historically needed different kinds of information from the same virus.
Attachment in two steps, and why the virus doesn't just go straight for the strong grip. HBV first makes weak, low-affinity contact with heparan sulfate proteoglycans (HSP), scattered across the liver's basement membrane, like a hand brushing past a surface. Only afterward does it lock onto NTCP, the high-affinity receptor on the hepatocyte's basolateral membrane. Why bother with the weak first step at all? A low-affinity, low-specificity tether increases the odds of the virus simply bumping into the right cell type long enough to find its real receptor, essentially buying time and proximity before committing to the high-affinity, more selective interaction that actually triggers entry. This two-step "touch then grip" sequence is a common exam point precisely because it's counterintuitive that the virus engages a low-specificity receptor first.
Why chronic carriage is fundamentally a story about the host, not the virus. As the clinical hook above makes clear, HBV itself isn't directly cytopathic in the way some viruses kill cells outright; liver damage and disease outcome instead trace back to how strongly the host's own cytotoxic T cells respond to infected hepatocytes. This single idea explains why the same virus produces wildly different outcomes in a neonate versus an adult, why interferon therapy (which boosts immune activity) is one of the two pillars of chronic treatment, and why "the virus is more aggressive in this patient" is usually the wrong way to think about a severe case, "the immune response is different in this patient" is closer to the truth.
Pathogenesis of Hepatitis B
Physical Properties and Antigenic Classification
- Resistant to extreme temperatures. It can be stored at 37℃ for 60 minutes, for seven days at 44℃, and at room temperature for six months. But are sensitive to high temperatures and are killed when heated to 60℃ for 10 hours and 100℃ for 1 minute.
- HBsAg is a very stable antigen. The same gene encodes the 3 glycoproteins (S, L, and M) of this antigen. S protein being the highest. These are responsible for attachment to host serum albumin, helping in the infection of hepatocytes.
- HBsAg helps in antigenic differentiation of the HBV as HBsAg contains group-specific antigen d or y and w or r. Combining these specific antigens gives rise to 4 subtypes of HBV; ADW, ADR, AYW, and AYR.
- And there is a total of eight genotypic variations (A, B, C, D, E, F, G, and H).
- Although the virus is DNA, formation of RNA with the help of reverse transcriptase mediates the replication. And replication occurs in the nucleus of the infected host cell.
Transmission of Hepatitis B
The transmission is generally in the following ways;
- Sexual intercourse with an infected person.
- Blood transfusion of an infected individual to healthy individuals.
- Organ transfusion without proper screening.
- From the infected mother to the fetus.
- Needle sharing and use of contaminated blades.
Incubation period
The incubation period of hepatitis B infection varies from a few weeks to 6 months.
- The virus enters through blood, and as it has an affinity for hepatocytes, it binds and replicates in those cells. The replication leads to the production of viral antigens that activate the cytotoxic T cells like CD8 lymphocytes, which causes various immunological reactions.
- The stage (acute or chronic) of infection depends upon the cytotoxic T-cell response of the individual. If the reaction is strong, the person can be free from the disease, and if the response is not strong, these individuals could be chronic carriers. Chronic case occurs more in children (neonates and infants) than in adults. Hepatocellular carcinoma is the result of persistent infection of the hepatocytes.
Replication
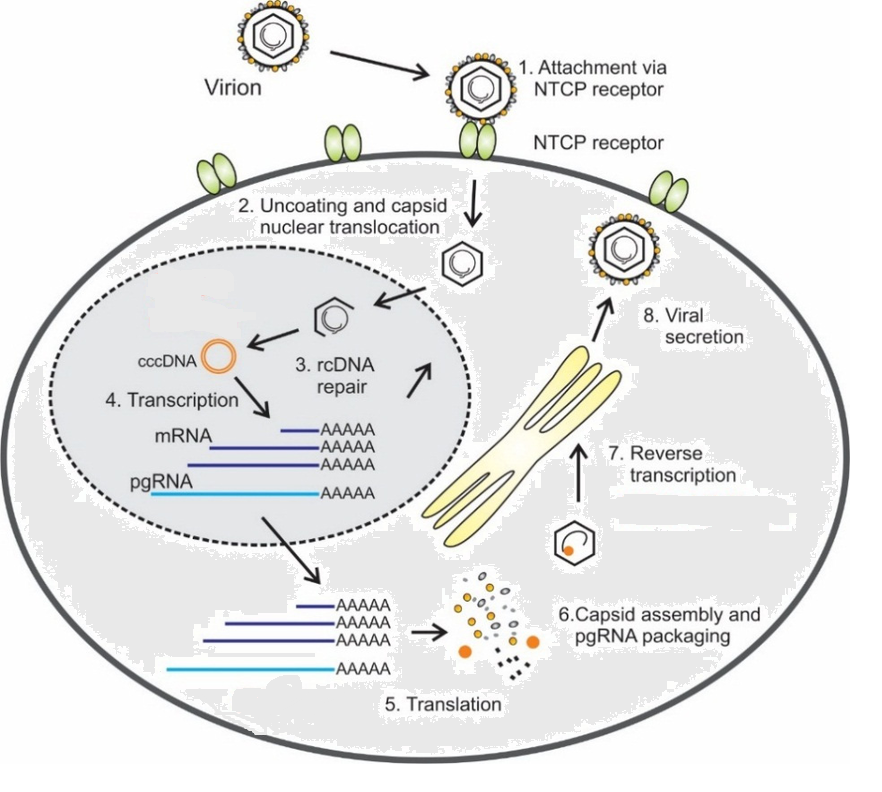
The replication of the hepatitis b virus has the following steps:
- Firstly, the infection begins with low-affinity attachment to heparan sulfate proteoglycans (HSP)– glycoprotein present in the basement membrane and secretary vesicles.
- After that, high-affinity attachment occurs to NTCP (sodium taurocholate co-transporting polypeptide) a carrier protein (glycoprotein) present in the basolateral membrane of the hepatocyte.
- Likewise, the internalization occurs by endocytosis, and the uncoating of the viral envelope facilitates the translocation of capsid with relaxed circular DNA (rcDNA) into the nucleus of the host.
- Similarly, rcDNA repairs into covalently closed circular DNA (cccDNA).
- The cccDNA acts as a template for the transcription of mRNA.
- The mRNA translates the viral protein.
- The viral protein (core, surface, and polymerase protein) and capsid enclose pre-genomic RNA assembles in the cytoplasm.
- The pg-RNA converts into DNA by reverse transcriptase in the viral capsid and may return back into the nucleus to repeat the replication process.
- Then the complete viral particles release from the infected host cell.
 Clinical signs and symptoms
Clinical signs and symptoms
The clinical signs and symptoms of HBV depend on various factors like; age, immune system, and level of HBV in the body.
Acute HBV infection: Symptoms of HBV are as follows:
During the pre-icteric stage
- Anorexia
- Malaise
- Fatigue
During the icteric phase
- Nausea,
- Vomiting
- Jaundice with liver tenderness
- Dark-colored urine
- Although the symptoms may be similar to HAV infections, the severity is high in HBV infections, leading to fatal.
NOTE:Icteric- of, relating to, or affected with jaundice.
Chronic Hepatitis B infections: Most chronic hepatitis cases are asymptomatic, but if symptoms develop, it is similar to acute hepatitis and can be a sign of liver damage. It may lead to
- liver cirrhosis.
- and liver cancer.
Diagnosis of Hepatitis B
Diagnosis relies on a combination of serum collected without anticoagulant, viral antigen and antibody detection, and supporting liver function tests.
Antigen detection: HBsAg and HBeAg are the two markers checked first. HBsAg confirms current infection; persistence of HBsAg beyond six months defines the chronic state. HBeAg signals active viral replication and higher infectivity. HBcAg itself is never detected in serum (see "Why HBcAg is not detected in Serum" below for the mechanism).
Antibody detection: IgM anti-HBc marks recent infection; IgG anti-HBc marks past infection; anti-HBs marks recovery or vaccine-induced immunity; anti-HBe tracks declining replication. Reading these markers together, including the commonly misread "window period" pattern, is covered in full in the dedicated guide to interpreting hepatitis B serology results.
Molecular and supporting tests: HBV PCR is used mainly in chronic-stage monitoring and in working up liver failure of uncertain cause. Liver function tests (ALT, AST, bilirubin) support the diagnosis by quantifying liver injury but don't identify the virus itself.
Why HBcAg is not detected in Serum?
Hepatitis B core antigen (HBcAg) is an intracellular antigen synthesized within infected hepatocytes and is expressed by infected hepatocytes only. Most of the generated HBcAg is assembled into the viral core (nucleocapsid). Free HBcAg does not circulate in significant quantity in the blood, but it does circulate as part of the intact hepatitis B virion. So HBcAg is not detected in serum tests, but antibodies produced against HBcAg, i.e. (anti-HBc), can be detected in the serum throughout HBV infection.
Treatment of Hepatitis B
No specific antiviral therapy is available to treat acute hepatitis B infection. Treatment of symptoms is the only measure in treating acute disease. The antiviral therapy is recommended for chronic cases. The treatment with interferons and nucleoside analogs is the standard method used. These do not cure HBV but only prevent morbidity and complications related to HBV infections.
Interferon: Interferon-alpha is the most common interferon used in treating hepatitis. The interferon prevents the progression of acute infection to chronic and neutralization of viremia.
Nucleoside analogs: Nucleoside analogs such as lamivudine, adefovir, and telbivudine are widely used in antiviral therapy. These analogs halt the replication of HBV. These are bio-available and highly effective antiviral therapy available.
Prevention and Control
The preferable method to prevent and control HBV infections is both vaccines and immunoglobulins .
- Immunoglobulin: The passive immunization just before or after exposure to the virus with HBIg. It is obtained from the patients who have recovered from the infection and contains a high titer of HBsAb. It is recommended to those in recent contact with infected people, who are to be in household contact with the infected people, infants born with HBsAg positive mothers, and those in sexual contact with acutely infected patients.
- Vaccines: Plasma-derived and recombinant DNA HBV vaccines are the two types of vaccines available with HBsAg that generates anti-HBs. Recommended vaccine schedule for adults is at 0,1 and 6 months, and infants are at birth, at 1-2 months, and 6-18 months.
Where Students Get Confused
HBV is a DNA virus, but it replicates using RNA and reverse transcriptase. This contradicts the usual DNA-virus-replicates-in-nucleus-without-RNA-intermediate pattern students learn first. HBV's relaxed circular DNA (rcDNA) is repaired into cccDNA, which is transcribed into pre-genomic RNA, which is then reverse-transcribed back into DNA inside the capsid, a DNA-to-RNA-to-DNA cycle more typical of retroviruses than of classic DNA viruses.
Subtype and genotype are not the same classification, and questions often test the difference deliberately. A genotype is fixed by the genome's DNA sequence; the subtype label (ADW, ADR, AYW, AYR) is based on HBsAg's surface determinants and doesn't map one-to-one onto genotype.
Chronic carriage is far more about the host's immune response than about a "stronger" viral strain. Most students assume a worse outcome means a more virulent virus; for HBV, it's more often the host's weaker T-cell response (as seen disproportionately in neonates and infants) that determines progression to chronic infection, not a uniquely aggressive viral subtype or genotype.
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Family | Hepadnaviridae |
| Genome | Partially double-stranded circular DNA, ~3,200 bp |
| Genes (overlapping ORFs) | S (surface), C (core), P (polymerase/reverse transcriptase), X (transcriptional regulator) |
| Virion particle types | 22 nm spherical, filamentous/tubular, 42 nm Dane particle (complete virion) |
| Subtypes | ADW, ADR, AYW, AYR (based on HBsAg determinants) |
| Genotypes | A through H (based on genome sequence) |
| Attachment receptors | Low-affinity: heparan sulfate proteoglycans (HSP); high-affinity: NTCP |
| Replication intermediate | cccDNA (covalently closed circular DNA), the template for all viral mRNA |
| Chronicity threshold | HBsAg persisting beyond 6 months |
| Highest-risk group for chronic carriage | Neonates and infants (weaker cytotoxic T-cell response) |
| Major long-term complications | Cirrhosis, hepatocellular carcinoma |
| First-line acute treatment | Supportive (no specific antiviral for acute HBV) |
| Chronic treatment | Interferon-alpha, nucleoside/nucleotide analogs (lamivudine, adefovir, telbivudine) |
References
- Krajden, M., McNabb, G., & Petric, M. (2005). The laboratory diagnosis of hepatitis B virus. Canadian Journal of Infectious Diseases and Medical Microbiology, 16(2), 65–72. https://doi.org/10.1155/2005/450574
- Liang, T. J. (2009). Hepatitis B: the virus and disease. Hepatology, 49(5 Suppl), S13–S21. https://doi.org/10.1002/hep.22881
- Parija, S. C. (2012). Textbook of Microbiology and Immunology (2nd ed., pp. 550–555). Elsevier.
Frequently Asked Questions
Why are babies infected with hepatitis B at birth more likely to become chronic carriers than adults?
What's the difference between HBV genotype and subtype?
Why is HBcAg never found on a standard hepatitis B blood test?
Is hepatitis B curable with current antiviral drugs?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.