RPR Test (Rapid Plasma Reagin): Principle, Procedure, Interpretation, and Syphilis Screening Algorithm
The RPR test is a non-treponemal screening test for syphilis using cardiolipin antigen. Learn its flocculation principle, qualitative and quantitative procedures, treatment monitoring by titer, false positive causes, and the two-test algorithm for syphilis diagnosis.
A 24-year-old woman attends her first antenatal visit at 10 weeks of pregnancy. Routine blood tests include an RPR screen for syphilis — a standard WHO recommendation for all pregnant women in their first trimester. The result is reactive at a titer of 1:16.
This single result initiates a specific clinical pathway: the RPR reactive result must be confirmed by a treponemal test (TPHA or FTA-ABS) before treatment is given. If confirmed, she receives benzathine penicillin G. Without treatment, her baby faces a 70–100% risk of congenital syphilis — a preventable cause of stillbirth, neonatal death, and long-term disability.
This is why syphilis screening with RPR exists: to identify a treatable infection in a population (pregnant women, sexual health attendees, blood donors) before clinical disease or vertical transmission occurs. Understanding how RPR works, what a reactive result means, and crucially what it does not mean, is essential for anyone involved in antenatal care, sexual health, or clinical laboratory practice.
The rapid plasma reagin (RPR) test is a macroscopic, nontreponemal flocculation card test used to screen for syphilis.
Let’s first analyze the test name:
Rapid: It is a rapid test that can be done within a few minutes.
Plasma: The sample is plasma (or serum)
Reagin: The term “reagin” means that this test does not look for antibodies against the actual bacterium, but rather for antibodies against substances released by cells when they are damaged by Treponema pallidum.
In some textbooks you can find reagin means an antibody to cardiolipin.
RPR test is one of the nonspecific tests (another non-specific test is VDRL Test) commonly used to screen the population for syphilis. The RPR test measures IgM and IgG antibodies to lipoidal material released from damaged host cells as well as to lipoprotein-like material, and possibly cardiolipin released from the treponemes.
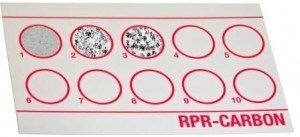 Figure: RPR Test card
Figure: RPR Test card
The anti-lipoidal antibodies are antibodies that are produced not only as a consequence of syphilis and other treponemal diseases but also in response to nontreponemal diseases of an acute and chronic nature in which tissue damage occurs.
The Two-Test Algorithm: Screening and Confirmation
The single most important clinical concept about the RPR test is that a reactive RPR result alone does not diagnose syphilis. RPR measures antibodies against cardiolipin — a lipid component of cell membranes — not against Treponema pallidum itself. These reagin antibodies are produced in syphilis but also in many other conditions (see False Positives below). A reactive RPR without confirmatory treponemal testing will lead to unnecessary treatment and patient distress.
The WHO-recommended two-test algorithm:
| Step | Test | Type | Purpose |
|---|---|---|---|
| Step 1 — Screen | RPR or VDRL | Non-treponemal | Sensitive, cheap, fast; detects most active syphilis; also positive in false-positive conditions |
| Step 2 — Confirm | TPHA, FTA-ABS, or TPPA | Treponemal | Specific for T. pallidum antibodies; confirms true syphilis; remains positive for life after infection |
Interpreting the two-test combination:
| RPR | Treponemal test | Interpretation |
|---|---|---|
| Reactive | Reactive | Confirmed syphilis — treat according to stage |
| Reactive | Non-reactive | Biological false positive RPR — investigate underlying cause (autoimmune, infection, pregnancy) |
| Non-reactive | Reactive | Past treated syphilis (treponemal tests remain positive for life) OR very early/late syphilis where RPR is negative |
| Non-reactive | Non-reactive | No serological evidence of syphilis |
Reverse algorithm (used in some high-resource laboratories): Some laboratories screen with a treponemal EIA/CLIA first, then confirm reactive results with RPR. This "reverse" algorithm is more sensitive for late syphilis but may detect more biologically false-positive treponemal tests. The traditional algorithm (RPR first) remains standard in most LMIC settings including South Asia, Africa, and Southeast Asia due to cost and equipment considerations.
Antigen used in RPR Test
RPR antigen contains cardiolipin, lecithin, cholesterol, 10% choline chloride, EDTA, charcoal, etc in a buffer.
The antigen is prepared from a modified Venereal Disease Research Laboratory (VDRL) antigen suspension containing choline chloride to eliminate the need to heat inactivate serum, ethylenediaminetetraacetic acid (EDTA) to enhance the stability of the suspension, and finely divided charcoal particles as a visualizing agent.
Positive Control: Prepared from human serum samples containing antibodies to Treponema pallidum. Serum is ready to use. Bring to room temp before use.
The test kits can be purchased from many commercial sources.
RPR vs VDRL: Choosing Between the Two Non-Treponemal Tests
Both RPR and VDRL are non-treponemal screening tests for syphilis using cardiolipin-based antigens. Students frequently ask why two tests exist — the answer is practical rather than scientific:
| Feature | RPR | VDRL |
|---|---|---|
| Specimen | Unheated serum or plasma | Heated serum (56°C for 30 min to inactivate complement) |
| Reading | Macroscopic — visible black flocculation on card | Microscopic — requires microscope at 100× |
| Equipment needed | Rotator, high-intensity light source | Rotator, microscope |
| Setting | Field-friendly; antenatal clinics, sexual health, outreach | Laboratory-based |
| CSF testing | Not validated for CSF | CSF VDRL is the standard test for neurosyphilis |
| Sensitivity (primary syphilis) | ~86% | ~78% |
| Sensitivity (secondary syphilis) | ~99% | ~100% |
| Treatment monitoring | Both can be used; RPR more practical in clinic settings | Standard in many reference labs |
| Cost | Slightly higher (charcoal antigen card) | Lower (glass slide reagents) |
Practical rule: RPR is preferred in clinical and field settings — no heating, no microscope, results visible to the naked eye. VDRL is preferred for CSF testing in suspected neurosyphilis — the only validated non-treponemal test for cerebrospinal fluid. Using RPR on CSF is not recommended because it was not validated for that specimen type.
RPR Test Principle
RPR antigen is mixed with unheated or heated (to inactivate complement) serum or with unheated plasma on a plastic-coated card.
If antibodies are present, they combine with the lipid particles of the antigen, causing them to agglutinate. The charcoal particles coagglutinate with the antibodies and show up as black clumps against the white card (macroscopically visible flocculation-type precipitation if the patient’s sera contain reagin).
Without some other evidence for the diagnosis of syphilis, even a reactive nontreponemal test does not confirm T. pallidum infection and treponemal tests such as Treponema pallidum haemagglutination assay (TPHA) or Fluorescent Treponemal Antibody Absorption Test (FTA-Abs) must be done to confirm syphilis.
If antibodies are not present in the test serum, the test mixture is uniformly gray.
PREPARATION FOR THE RPR ASSAY
Bring RPR antigen suspension, positive control, negative control, and samples to room temperature (20–30°C) before use.
All reagents are ready for use as supplied. Gently mix the reagents before use; avoid foaming.
Qualitative RPR Test Procedure
- Label a RPR card with patient and control information being careful not to interfere with the test areas of the card.
- Using disposable serum dispensers or droppers, dispense one free-falling drop (0.05 ml) of serum or plasma sample onto a circle on the test card. When using droppers/dispensers, keep it in a vertical position to ensure accurate delivery.
- Repeat by adding one free-falling drop of positive control and negative control using a new dispenser for each sample.
- Spread the sample smoothly across the circle area using the paddle side of the dispenser as shown by instructor. Take care not to scratch the test area.
- After mixing the antigen solution by swirling, add one drop of the antigen suspension to each sample/control testing area. Note: hold the antigen container upside down directly over the test area such that the drop falls directly onto the center of the circle. DO NOT STIR OR SPREAD THE ANTIGEN.
- Place the card on an automatic rotator and cover to maintain humidity. Rotate at 100 ± 5 rpm for 8 minutes (7 minutes 50 seconds to 8 minutes 30 seconds). Following rotation, a brief hand rotation and tilting of the card (3–4 times) should be performed to aid in differentiating nonreactive from minimally reactive results.
- Immediately read results macroscopically in the “wet” state under a high-intensity light source.
Interpretation of RPR Test
- Non-reactive (NR) – smooth suspension, no clumping or slight roughness
- Reactive (R) – any degree of clumping
If the test is negative, but the physician still suspects the infection is present, the more specific treponemal tests (FTA-ABS, MHA-TP, TPHA, etc.) should be performed.
Quantitative RPR and Titer Monitoring
The qualitative RPR (reactive or non-reactive) identifies who has reagin antibodies. The quantitative RPR expresses the titer — the highest dilution at which the test remains reactive — and is essential for:
1. Staging the infection: Higher titers generally correlate with more active disease:
- Primary syphilis: often 1:4 to 1:32
- Secondary syphilis: typically high titers 1:16 to 1:256
- Latent syphilis: variable, often lower
- Late/tertiary syphilis: may be low or even negative
2. Confirming treatment response: After adequate treatment, RPR titers should fall. The expected pattern:
| Time after treatment | Expected titer change | Interpretation |
|---|---|---|
| 6 months | ≥4-fold decrease (e.g., 1:32 → 1:8) | Adequate treatment response |
| 12 months (primary/secondary) | Titer ≤1:4 or non-reactive | Treatment successful |
| 24 months (latent) | Titer ≤1:4 or non-reactive | Treatment successful |
| No change or rising titer | — | Treatment failure or reinfection — re-evaluate and re-treat |
The four-fold rule: A four-fold change in titer (either increase or decrease) is considered clinically significant — equivalent to a two-dilution change (e.g., 1:4 to 1:16, or 1:32 to 1:8). This rule applies to both confirming disease progression and confirming treatment response. A titer that does not fall four-fold within expected timeframes suggests treatment failure, reinfection, or neurosyphilis.
3. Detecting reinfection: A four-fold rise in titer in a previously treated patient with a low stable titer strongly suggests reinfection, warranting repeat treatment.
Serofast reaction: Some patients, particularly those treated in late-stage syphilis or latent infections of unknown duration, maintain a low persistent RPR titer (often ≤1:4) even after adequate treatment. This "serofast" state does not indicate treatment failure and should not prompt repeat treatment in the absence of clinical symptoms or evidence of reinfection.
False-positive results
As reagin antibodies are also produced by patients with other infectious and non-infectious conditions, false-positive results are likely to occur.
Patients with the following infectious diseases may produce reagin antibodies;
- Chancroid
- Chickenpox
- Hepatitis
- Infectious mononucelosis
- Leprosy
- Leptospirosis
- Lymphogranuloma venereum (LGV)
- Malaria
- Measles
- Ricekttsial disease
- Trypanosomiasis and
- Tuberculosis
Non-infectious conditions
- Autoimmune disorders (rheumatoid disease)
- Drug addiction
- Other factors (old age, pregnancy, recent immunization
Uses of non-treponemal tests
As antibodies to Treponema pallidum may persist indefinitely regardless of the disease state or prior therapy, treponemal tests (FTA-ABS, TPHA or TPPA) fail to differentiate between active and past syphilis infection but non-treponemal tests (such as VDRL and RPR) may help to differentiate between active and past syphilis infection.
Nontreponemal antibodies are generally detected by the rapid plasma reagin (RPR) assay, which is typically positive during current infection and negative following treatment or during late/latent forms of syphilis.
RPR Sensitivity by Stage of Syphilis
RPR sensitivity varies significantly depending on when in the disease course it is performed. This is clinically important because a negative RPR does not rule out syphilis in certain situations:
| Stage | RPR sensitivity | Clinical note |
|---|---|---|
| Primary syphilis (chancre present) | ~86% | Window period — early primary syphilis may be seronegative; if clinical suspicion high, repeat in 2–4 weeks or perform darkfield microscopy |
| Secondary syphilis (rash, systemic) | ~99% | Highest sensitivity; RPR almost always reactive; high titers |
| Early latent (<1 year) | ~95% | Still quite sensitive |
| Late latent / latent unknown duration | ~73% | Reduced sensitivity; treponemal test more reliable |
| Tertiary syphilis | ~70% | Low sensitivity; may be non-reactive; treponemal test essential |
| Neurosyphilis | Variable | Serum RPR may be reactive but VDRL-CSF is the standard test for CNS involvement |
The prozone phenomenon (false-negative at high titer): In secondary syphilis with very high antibody concentrations, the RPR can paradoxically give a non-reactive result — the excess of antibody relative to antigen prevents flocculation (prozone effect). If secondary syphilis is strongly suspected clinically but RPR is non-reactive, request that the laboratory test the sample at dilutions (1:2, 1:4, 1:8) to detect the prozone phenomenon. This is an important but frequently missed source of false-negative RPR results.
How to Remember
RPR = the screening test that monitors treatment, not the test that confirms syphilis.
Two properties define everything about RPR's clinical role:
- It is non-treponemal — detecting antibodies to cardiolipin, not to T. pallidum. Therefore it is non-specific (false positives exist) and cannot stand alone as a diagnosis.
- It is quantitative — the titer rises in active disease and falls after treatment. No other syphilis test does this reliably. This is its unique clinical value.
The two-test rule for syphilis — always:
Screen with RPR → Reactive → Confirm with TPHA or FTA-ABS → Both reactive → Diagnose syphilis and treat RPR reactive + treponemal non-reactive = biological false positive — do not treat for syphilis
RPR vs VDRL — the one-sentence distinction: RPR = macroscopic card test, no heating, no microscope, field-friendly. VDRL = microscopic slide test, serum must be heated; only validated option for CSF (neurosyphilis).
The charcoal makes RPR possible: The black charcoal particles in the RPR antigen are what make the result visible to the naked eye. Without the charcoal, flocculation (as in VDRL) is only visible under a microscope. The charcoal is not part of the immunological reaction — it co-agglutinates with the antibody-lipid complex purely as a visible marker. Remembering this explains why RPR cards must be read immediately while still wet — the charcoal settles on drying.
The prozone trap: Very reactive = very high antibody = may paradoxically give false-negative on neat sample. If secondary syphilis is strongly suspected but RPR is negative → request diluted testing. This is tested in examinations specifically because it is counterintuitive.
The syphilis serology trio as a clinical anchor:
| Test | Non-treponemal or Treponemal | Reactive in treated past infection? | Use |
|---|---|---|---|
| RPR / VDRL | Non-treponemal | No (usually reverts) | Screen; monitor treatment |
| TPHA / TPPA | Treponemal | Yes — for life | Confirm; does not monitor treatment |
| FTA-ABS | Treponemal | Yes — for life | Confirm; most sensitive in primary |
References
- Phaosavasdi, S., Snidvongs, W., Thasanapradit, P., Ungthavorn, P., Bhongsvej, S., Jongpiputvanich, S., Vejjajiva, S., Udomsantisuk, P., Chitwarakorn, A., & Panikabutra, K. (1989). Rapid Plasma Reagin test (RPR) compared to Venereal Diseases Research Laboratory test (VDRL) for the diagnosis of syphilis in pregnancy. Journal of the Medical Association of Thailand = Chotmaihet thangphaet, 72(4), 202–206.
- Walker A. N. (1971). Rapid plasma reagin (RPR) card test. A screening method for treponemal disease. The British journal of venereal diseases, 47(4), 259–262. https://doi.org/10.1136/sti.47.4.259
- World Health Organization. (2006). The Use of Rapid Syphilis Tests. Geneva: WHO. https://www.who.int/reproductivehealth/publications/rtis/TDR_SDI_06_1/en/
- Centers for Disease Control and Prevention. (2021). Sexually Transmitted Infections Treatment Guidelines, 2021: Syphilis. MMWR, 70(4). https://www.cdc.gov/std/treatment-guidelines/syphilis.htm
- Tille, P. M. (2017). Bailey and Scott's Diagnostic Microbiology (14th ed.). Elsevier.
Frequently Asked Questions
What is the prozone phenomenon in RPR testing and how is it recognized and resolved?
Why does RPR titer monitoring matter more than a single reactive result in managing syphilis treatment?
What are the main causes of a biological false-positive RPR, and how are they distinguished from true syphilis?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.