Measles Virus: Structure, Pathogenesis, and Why It Erases Immune Memory
How measles spreads via CD150/SLAM, why it erases years of immune memory, and how Koplik spots diagnose it before the rash appears.
In 2019, a measles outbreak swept through communities in Samoa, killing 83 people, most of them children under five. What made the outbreak particularly devastating was not just the measles deaths themselves, but what happened in the months afterward: children who recovered began dying from infections like pneumonia and diarrheal disease that they had previously survived without difficulty. Some had been vaccinated against these other pathogens years earlier and appeared protected. After measles, that protection was gone.
This phenomenon, called measles-induced immune amnesia, is one of the most clinically important and least-taught facts about this disease. Measles virus doesn't just cause acute illness; it infects and depletes memory B and T lymphocytes, effectively wiping out years of accumulated immunological memory against other pathogens. Studies using antigen arrays have shown that measles can eliminate 11–73% of a child's pre-existing antibody repertoire. In a population with high background rates of infectious disease, this immune reset is often what actually kills; not the virus itself.
Understanding why this happens requires understanding where the virus goes after it enters the respiratory tract. Measles doesn't stay local. It actively targets and enters the very immune cells that would normally contain it, using a receptor expressed specifically on activated lymphocytes, and then spreads systemically before the immune response can catch up. That spread is what produces the pathognomonic rash, the multi-system complications, and the immune suppression that outlasts the acute illness by months.
Structure of Measles Virus
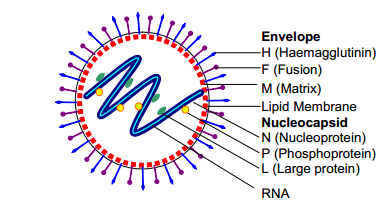 Figure: Structure of Measles Virus
Figure: Structure of Measles Virus
- Measles virus is a member of the genus Morbillivirus of the family Paramyxoviridae. Paramyxoviruses are so-called because they have an affinity for mucous membranes (Greek: myxa = mucus).
- Measles virus is a typical paramyxovirus (spherical enveloped particles that contain a non-segmented negative-strand RNA genome with a linear arrangement of genes).
- Measles virus has two glycoproteins spikes that are important in pathogenesis:
F (fusion) protein, which is responsible for the fusion of virus and host cell membranes, viral penetration, and hemolysis, and the H (haemagglutinin) protein, which is responsible for the binding of the virus to cells
- Measles virus has only one serotype i.e. Life long immunity occurs in individuals who have had the disease.
- Hemagglutinin is the antigen against which neutralizing antibody is formed.
- Infants are protected during the first six months of life ( they get maternal antibody as it passes the placenta)
Replication cycle of Measles Virus
- Adsorption to the cell surface: via Hemagglutinin. Wild-type measles virus primarily uses CD150/SLAM (signalling lymphocytic activation molecule) as its receptor on activated lymphocytes and dendritic cells, and Nectin-4 (PVRL4) on respiratory epithelial cells to facilitate systemic shedding. The CD46 receptor (a complement regulatory protein expressed on nearly all nucleated cells) is used by attenuated vaccine strains and laboratory-adapted strains, not by the wild-type virus circulating in nature. This distinction matters clinically: CD150/SLAM is expressed on activated lymphocytes — explaining why the virus specifically targets and depletes immune memory cells.
- Penetrates the cell surface and uncoats
- Virion RNA polymerase transcribes the negative-strand genome to mRNA
- Specific viral proteins are formed
- Assembly to helical nucleocapsid
- Release of the virus by budding
Transmission and Epidemiology of Measles
- Worldwide distribution, outbreaks in 2-3 years
- Measles virus is extremely infectious, most children contract the clinical disease on exposure
- Transmitted via respiratory droplets produced by sneezing or coughing during the prodromal period or direct contact with nasal or throat secretions from an infected person, which continues up to a few days after the rash appears.
- Less commonly, it is spread by airborne aerosolized droplet nuclei or by indirect contact with freshly contaminated articles.
- More serious outcomes in malnourished children, and people with deficient cell-mediated immunity.
 Figure: Health Alert Sign in a Clinic
Figure: Health Alert Sign in a Clinic
Pathogenesis
- Measles virus invades the cells lining the upper respiratory tracts i.e respiratory epithelium of the nasopharynx and spreads to the regional lymph nodes
- After 2-3 days of replication in these sites, a primary viremia widens the infection to the reticuloendothelial system where further replication takes place.
- Secondary viremia occurs and the virus enters skin, conjunctivae, respiratory tract and other organs, including the spleen, thymus, lung, liver, and kidney and further replication occurs.
- Appearances of rash (cytotoxic T cells attack measles virus-infected vascular endothelial cells in the skin).
- Formation of Multinucleated giant cells (Warthin-Finkeldey giant cells in lymphoid tissue; hallmark of measles on histology).
- Measles-induced immune amnesia: By entering memory B and T lymphocytes via CD150/SLAM, measles virus infects and destroys a significant proportion of the body's accumulated immunological memory — studies have shown depletion of 11–73% of a child's pre-existing antibody repertoire. In the 2–3 months following measles recovery, children are significantly more susceptible to other infections, including pathogens they had previously acquired immunity against. This immune suppression outlasts the acute illness and accounts for a substantial proportion of measles-attributable childhood mortality in high-burden settings.
Clinical features of Measles
 Figure: Koplik’s spot is the major diagnostic criterion for Measles Source: CDC
Figure: Koplik’s spot is the major diagnostic criterion for Measles Source: CDC
- Incubation period: 10-14 days
- Prodromal phase: Characterized by fever, conjunctivitis (causing photophobia), running nose, and coughing.
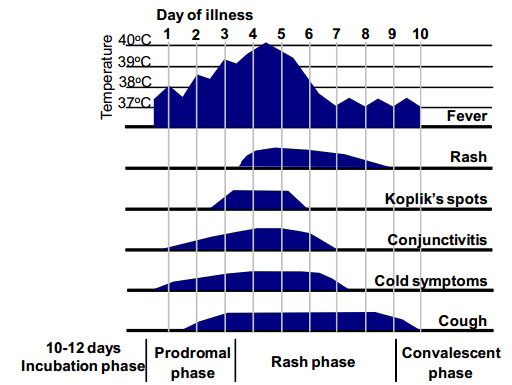 Figure: Fig: Clinical features of typical measles – time course from onset of illness
Figure: Fig: Clinical features of typical measles – time course from onset of illness
The appearance of Koplik’s spot (bright red lesions with the white, central dot) # Diagnostic feature
The appearance of Maculopapular rashes, common features of which includes:
Occurs 5‐7 days after symptoms
Lasts 3 or more days
Brownish hue
Progresses from face to body to extremities
The rash becomes confluent as it progresses
Soon after the rash appears, the patient is no longer infectious.
 Figure: A child infected with Measles Source:: CDC
Figure: A child infected with Measles Source:: CDC
Complications because of Measles infections
- Encephalitis: 1 per 1000 cases
- Subacute sclerosing panencephalitis (SSPE): A rare but universally fatal progressive encephalitis developing 7–10 years after acute measles infection, particularly in children infected before age two. The mechanism: during the acute infection, defective measles virus particles lacking a functional M (matrix) protein can persist in CNS neurons. Without functional M protein, the virus cannot assemble normally and bud out of cells — so it keeps accumulating intracellularly, slowly destroying the neuron from within. Years later, this persistent intracellular infection triggers a progressive encephalitis. SSPE is characterised by personality change, cognitive decline, myoclonic seizures, and eventually coma and death. Diagnosis is confirmed by extremely high measles antibody titers in CSF (10–100-fold higher than typical convalescent levels) and characteristic EEG patterns.
- Giant cell pneumonia
- Co-infections:
Secondary bacterial pneumonia Bacterial otitis media
- Increased risk of stillbirth in pregnant women infected with measles.
- Measles virus infection of a fetus causes fetal death
- Atypical measles develops in some people who were given killed vaccine and subsequently infected with the measles virus.
Laboratory diagnosis of measles
- Most diagnoses are made on clinical grounds; the presence of koplik’s spot provides a definitive diagnosis.
- If laboratory diagnosis is necessary, it can be done by
Isolation of virus in a cell culture A positive serologic test for measles IgM Demonstrating a rise in antiviral antibody titer of greater than four-fold. Identification of measles virus RNA from a clinical specimen by PCR
Isolation and Identification of the virus
Nasopharyngeal and conjunctival swabs, blood samples, respiratory secretions, and urine collected from a patient during the febrile period are appropriate sources for viral isolation. Monkey or human kidney cells or a lymphoblastoid cell line (B95-a) are optimal for isolation attempts. Measles virus grows slowly; typical cytopathic effects (multinucleated giant cells containing both intranuclear and intracytoplasmic inclusion bodies) take 7-10 days to develop. Shell vial culture tests are completed in 2-3 days using fluorescent antibody staining to detect measles antigens in the inoculated cultures.
However, virus isolation is technically difficult. It is not routinely performed for diagnosis as sensitivity is lower than serologic techniques.
Serology
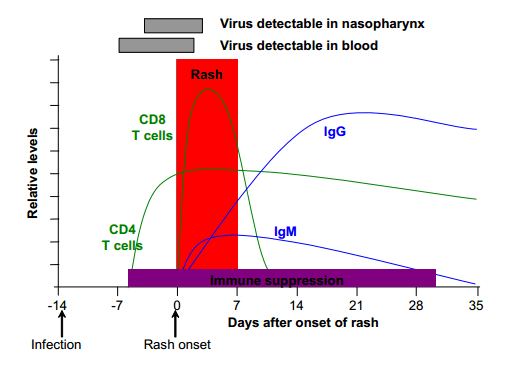 Figure: Immune responses in acute measles infection
Figure: Immune responses in acute measles infection
Serologic confirmation of measles infection depends on a fourfold rise in antibody titer between acute-phase and convalescent-phase sera (where the second serum sample is collected at least 10 days after the first, acute sample) or on the demonstration of measles specific IgM antibody in a single serum specimen drawn between 1 and 2 weeks after the onset of rash. IgM antibody levels peak after about 7-10 days and then decline rapidly, and are rarely detected after 6-8 weeks.
ELISA, HI, and neutralization tests all may be used to measure measles antibodies, though ELISA is the most practical method. IgG antibody levels peak within about 4 weeks and persist long after infection.
The major part of the immune response is directed against the viral nucleoprotein. Patients with subacute sclerosing panencephalitis (SSPE) display an exaggerated antibody response, with titers 10 to 100 fold higher than those seen in typical convalescent sera.
Haemagglutination–inhibition tests or ELISA antibody assays are the most practical, but plaque reduction neutralization tests are the most sensitive and specific. The virus has been isolated from respiratory tract secretions and rarely from urine or circulating lymphocytes during the prodromal phase of illness or within a few days after the rash onset.
Immunofluorescence staining of nasal or throat secretions or urine has been successful but is not widely available. SSPE is confirmed based on characteristic EEG patterns and demonstration of measles antibody in the cerebrospinal fluid (CSF) with an increased CSF to serum measles antibody ratio, or by the demonstration of virus in brain tissue.
Very high measles antibody titers aside from acute infection and SSPE are regularly seen in autoimmune chronic active hepatitis and occasionally in systemic lupus erythematosus.
Prevention of Measles
 Measles can be prevented with MMR vaccine. The vaccine protects against three diseases: measles, mumps, and rubella. The MMR vaccine is very safe and effective. Two doses of MMR vaccine are about 97% effective at preventing measles; one dose is about 93% effective. CDC recommends children get two doses of MMR vaccine,
Measles can be prevented with MMR vaccine. The vaccine protects against three diseases: measles, mumps, and rubella. The MMR vaccine is very safe and effective. Two doses of MMR vaccine are about 97% effective at preventing measles; one dose is about 93% effective. CDC recommends children get two doses of MMR vaccine,
- the first dose at 12 through 15 months of age, and
- the second dose at 4 through 6 years of age. Teens and adults should also be up to date on their MMR vaccination.
Vitamin A in Measles Management
The World Health Organization recommends Vitamin A supplementation for all children with measles, given as two daily doses regardless of their country of residence. Vitamin A deficiency impairs the immune response to measles and is associated with significantly higher rates of complications (particularly pneumonia and blindness) and mortality. Even in children without overt Vitamin A deficiency, supplementation at the time of illness reduces complication rates. In LMIC settings where Vitamin A deficiency is common and measles still circulates, this recommendation has a direct impact on case fatality rates.
How to Remember
The prodrome: 3Cs and a K. The classic measles prodrome is a set of four findings that appear 2–4 days before the rash: Cough, Coryza (runny nose), Conjunctivitis (the 3Cs), and Koplik spots. The 3Cs together with Koplik spots are so specific to measles that their presence alone is essentially diagnostic before any test is run. If you see "3Cs + white spots inside the mouth on a red base" in an exam question, it's measles.
Koplik spots: "the candle before dawn." Koplik spots appear on the buccal mucosa 1–2 days before the rash, are pathognomonic, and disappear as the rash develops. Think of them as a brief window of certainty: the clinician who checks the mouth at the right moment gets the diagnosis for free. They vanish once the rash arrives. This is also why the timing window for Koplik spots matters clinically — a patient presenting with established rash may no longer have them.
Rash: face down, never on palms or soles. Measles rash follows a cephalocaudal progression — starting on the face (often behind the ears at the hairline) and spreading downward to the trunk and extremities over 3 days. It becomes confluent as it spreads. A key distinguishing feature: measles rash typically spares the palms and soles (unlike secondary syphilis, Rocky Mountain spotted fever, and hand-foot-and-mouth disease, which specifically involve the palms and soles). Face-to-feet, not palms or soles — this contrast is a common exam differentiator.
SSPE: "the slow fuse." Subacute sclerosing panencephalitis develops 7–10 years after an acute measles infection, particularly in those infected before age two. The virus persists in CNS neurons with a defective M (matrix) protein that prevents normal budding, meaning the virus can't escape and keeps accumulating in the cell until it eventually destroys it. The result is a slow, progressive, universally fatal encephalitis. The long delay between infection and SSPE onset (years to a decade) is why it's often missed as a measles complication until the connection is made retrospectively.
Immune amnesia: the reason measles kills beyond the acute illness. The immune amnesia mechanism is simple enough to anchor as a principle: measles virus enters memory lymphocytes (via CD150/SLAM) and destroys them, taking years of acquired immune memory with them. What looks like a child recovering from measles is actually a child whose immune system has partially reverted to a more naive state. In practice, this means the 2–3 months after measles are a period of elevated vulnerability to other infections, even previously experienced ones.
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Family / Genus | Paramyxoviridae / Morbillivirus |
| Genome | Non-segmented, negative-sense ssRNA, ~16 kb |
| Envelope | Present; spherical, pleomorphic, 100–300 nm |
| Serotypes | One only — lifelong immunity after infection |
| Key surface glycoproteins | H (haemagglutinin — binds receptor, target of neutralising antibody); F (fusion — mediates cell fusion, syncytia formation, hemolysis) |
| Primary receptor (wild-type) | CD150/SLAM (on activated lymphocytes and dendritic cells) |
| Receptor for vaccine strain | CD46 (complement regulatory protein, ubiquitous on nucleated cells) |
| Respiratory epithelial receptor | Nectin-4 (PVRL4) — facilitates systemic shedding and transmission |
| Transmission | Respiratory droplets; airborne (highly contagious); infectious 4 days before to 4 days after rash onset |
| Incubation period | 10–14 days |
| Prodrome (3Cs + K) | Cough, Coryza, Conjunctivitis + Koplik spots |
| Koplik spots timing | 1–2 days before rash; pathognomonic; disappear as rash develops |
| Rash progression | Cephalocaudal (face → trunk → extremities); confluent; spares palms and soles |
| Immune amnesia | Destroys memory B and T lymphocytes; eliminates 11–73% of pre-existing antibody repertoire |
| CPE in cell culture | Multinucleated giant cells (Warthin-Finkeldey giant cells); intranuclear and intracytoplasmic inclusion bodies; 7–10 days |
| Confirmatory lab diagnosis | Measles-specific IgM (1–2 weeks after rash onset); fourfold antibody titer rise; PCR |
| SSPE | Delayed fatal encephalitis 7–10 years post-infection; defective M protein prevents viral budding; very high measles antibody titers in CSF |
| Treatment | Supportive; Vitamin A supplementation recommended for all measles cases in children (reduces complications and mortality) |
| Vaccine | MMR (live attenuated); dose 1 at 12–15 months, dose 2 at 4–6 years; 97% effective after 2 doses |
Where Students Get Confused
"Measles kills mainly through the acute illness." In high-income settings with good nutrition and supportive care, the acute illness is survivable for most children. In LMIC settings, measles kills substantially through immune amnesia and the secondary infections that follow, including pneumonia and diarrheal disease from pathogens the child had previously acquired immunity against. This is why measles mortality in undernourished populations is so much higher than in well-nourished ones, and why the WHO recommends Vitamin A supplementation for all measles cases in children, not just the most severe ones.
"CD46 is the measles virus receptor." This is correct for vaccine strains and laboratory-adapted strains but incorrect for wild-type measles. Wild-type virus primarily uses CD150/SLAM on activated lymphocytes and dendritic cells, and Nectin-4 on airway epithelial cells. The distinction matters because it explains why measles specifically targets immune cells (CD150/SLAM is expressed on activated lymphocytes — exactly the cells responding to the infection), whereas CD46 is expressed on nearly all nucleated cells and is what makes attenuated vaccine strains so broadly replicating.
"The rash in measles affects the palms and soles." It typically does not. Measles rash is cephalocaudal and spares the palms and soles. Diseases that specifically involve the palms and soles include secondary syphilis, Rocky Mountain spotted fever, hand-foot-and-mouth disease, and rat-bite fever. This distinction is a frequent exam trap and a real clinical differentiator.
"SSPE occurs shortly after measles infection." SSPE has a latency of 7–10 years, meaning a teenager presenting with SSPE may have had measles as an infant or toddler, with no apparent neurological issue for a decade in between. It presents with progressive personality change, cognitive decline, seizures, and eventually coma and death. The clue on examination is extremely high measles antibody titers in both serum and CSF.
"A child with measles is infectious as long as they have a rash." Not quite. The infectious period runs from approximately 4 days before rash onset until 4 days after rash appearance (the 4+4 rule). The highest viral shedding occurs in the prodromal phase — before any rash is visible — which is exactly why measles outbreaks spread so efficiently before anyone suspects measles is the diagnosis.
References
- Naim, H. Y. (2015). Measles virus. Human Vaccines & Immunotherapeutics, 11(1), 21–26. https://doi.org/10.4161/hv.34298
- Rota, P. A., Moss, W. J., Takeda, M., de Swart, R. L., Thompson, K. M., & Goodson, J. L. (2016). Measles. Nature Reviews Disease Primers, 2, 16049. https://doi.org/10.1038/nrdp.2016.49
- Mühlebach, M. D., Mateo, M., Sinn, P. L., Püschel, K., Billeter, M. A., Johnston, P. B., Cattaneo, R., Blechert, B., Christoph, T., Lieber, A., Belnoue, E., Bhatt, D. L., Bhatt, M. B., & Bhatt, N. (2011). Adherens junction protein nectin-4 is the epithelial receptor for measles virus. Nature, 480(7378), 530–533. https://doi.org/10.1038/nature10639
- Mina, M. J., Kula, T., Leng, Y., Li, M., De Vries, R. D., Knip, M., Siljander, H., Rewers, M., Chour, D. B., & Elledge, S. J. (2019). Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science, 366(6465), 599–606. https://doi.org/10.1126/science.aay6485
Frequently Asked Questions
What is measles immune amnesia and why does it matter clinically?
Why are Koplik spots diagnostically valuable?
Why does measles rash spare the palms and soles?
What causes SSPE and why does it appear years after measles?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.