Leishmania: Life Cycle, Types of Leishmaniasis, Pathogenesis, and Laboratory Diagnosis
Understand Leishmania species, the sandfly life cycle, three forms of leishmaniasis (visceral, cutaneous, mucocutaneous), and laboratory diagnosis — from LD bodies to rK39 RDT — with exam mnemonics.
A 28-year-old farmer from the Terai belt of Nepal presents with six weeks of fever that comes and goes irregularly, a dramatically enlarged spleen, and progressive weight loss. His haemoglobin is 7 g/dL. He has not responded to antibiotics. The clinician notices he lives in a mud-walled house in a low-lying, humid area — ideal sandfly habitat. A fingertip blood sample is applied to a rapid rK39 dipstick. A positive line appears within five minutes.
Visceral leishmaniasis — kala-azar — kills nearly 100% of untreated patients within two years. But it is also completely treatable if diagnosed correctly. This case illustrates both the clinical signature (prolonged fever + massive splenomegaly + pancytopenia + LMIC setting) and why rapid field-based serology has transformed case detection in endemic South Asia. Understanding Leishmania from organism to diagnosis is directly relevant to clinical practice across Nepal, India, Bangladesh, East Africa, and Brazil — regions that bear most of the world's burden.
What Is Leishmania?
Leishmania is an obligate intracellular protozoan parasite belonging to the order Kinetoplastida, family Trypanosomatidae. It infects and replicates within macrophages of the host's reticuloendothelial system.
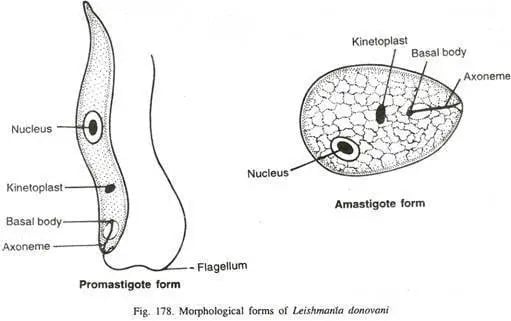
Two morphological forms:
 | Form | Host | Location | Shape |
| --- | --- | --- | --- |
| Amastigote (Leishman-Donovan body / LD body) | Human (and other mammalian hosts) | Inside macrophages | Small (2–4 μm), oval, non-flagellate; large kinetoplast visible |
| Promastigote | Sandfly vector | Midgut and salivary glands | Elongated (15–25 μm), free-living, prominent anterior flagellum |
| Form | Host | Location | Shape |
| --- | --- | --- | --- |
| Amastigote (Leishman-Donovan body / LD body) | Human (and other mammalian hosts) | Inside macrophages | Small (2–4 μm), oval, non-flagellate; large kinetoplast visible |
| Promastigote | Sandfly vector | Midgut and salivary glands | Elongated (15–25 μm), free-living, prominent anterior flagellum |
The transformation between forms — promastigote in the sandfly → amastigote in the human macrophage → promastigote in the next sandfly — is the life cycle in summary.
Life Cycle of Leishmania
Leishmania has a two-host life cycle: the sandfly (definitive host, where promastigotes develop) and the mammalian host including humans (intermediate host, where amastigotes replicate).
In the Sandfly Vector
- A female phlebotomine sandfly (Phlebotomus spp. in Old World; Lutzomyia spp. in New World) takes a blood meal from an infected host, ingesting amastigote-laden macrophages.
- In the sandfly midgut, amastigotes transform into promastigotes and multiply by binary fission.
- Promastigotes migrate anteriorly to the proboscis and salivary glands as metacyclic promastigotes (the infective form).
In the Human Host
- The sandfly injects metacyclic promastigotes into the skin during a blood meal.
- Promastigotes are phagocytosed by skin macrophages and dendritic cells.
- Inside the phagolysosome of the macrophage, promastigotes transform into amastigotes and begin multiplying.
- Infected macrophages rupture, releasing amastigotes that infect new macrophages.
- Depending on the species, amastigotes disseminate to visceral organs (VL) or remain localised to skin (CL) or mucosa (MCL).
Key life cycle fact for the exam: The definitive host is the sandfly — this is where sexual reproduction (in some Leishmania species) and development of the infective stage occur. Humans are the intermediate host where asexual multiplication of amastigotes takes place. For Indian kala-azar specifically, humans are the only reservoir — no animal reservoir exists, making it an anthroponotic infection.
Types of Leishmaniasis
Three major clinical syndromes, each caused by different Leishmania species:
1. Visceral Leishmaniasis (VL) — Kala-Azar
Causative species: Leishmania donovani (India, Bangladesh, Nepal, East Africa); L. infantum (Mediterranean, Middle East, Latin America); L. chagasi (Latin America — now considered same as L. infantum)
The parasite disseminates from the skin to visceral organs: spleen, liver, bone marrow, and lymph nodes. Amastigotes multiply within macrophages of the reticuloendothelial system throughout these organs.
Classic clinical tetrad:
- Prolonged irregular fever (weeks to months)
- Massive splenomegaly (the dominant finding — spleen can reach the pelvic brim)
- Hepatomegaly
- Progressive weight loss, weakness, anemia
Laboratory hallmark: Pancytopenia — reduced WBCs, RBCs, and platelets due to hypersplenism and bone marrow infiltration.
Post-kala-azar dermal leishmaniasis (PKDL): A skin complication occurring months to years after apparently successful treatment of VL — hypopigmented macules progressing to nodules on face and trunk. Patients with PKDL serve as a reservoir for ongoing transmission. Important in the Indian subcontinent elimination programme.
Fatality if untreated: Up to 100% within 2 years in endemic settings.
2. Cutaneous Leishmaniasis (CL) — Oriental Sore / Delhi Boil
Causative species: L. tropica (Old World: Middle East, Central Asia); L. major (Old World: Africa, Middle East); L. braziliensis, L. mexicana (New World)
Amastigotes remain localised at the site of the sandfly bite, producing a painless papule that ulcerates into a classic volcano crater ulcer — raised, indurated edges with a central depression. Lesions heal spontaneously over months to years but leave a depigmented scar. The face, arms, and legs are most commonly affected.
3. Mucocutaneous Leishmaniasis (MCL) — Espundia
Causative species: Leishmania braziliensis (South America)
Starts as cutaneous lesions but spreads lymphatically or haematogenously to the mucosal surfaces of the nose, mouth, and throat. Causes progressive, disfiguring destruction of the nasal septum and palate. Does not heal spontaneously. Associated with significant stigma and disability.
Three-disease summary table:
| Feature | Visceral (VL) | Cutaneous (CL) | Mucocutaneous (MCL) |
|---|---|---|---|
| Main species | L. donovani | L. tropica, L. major | L. braziliensis |
| Site of infection | Visceral organs (spleen, liver, BM) | Skin only | Skin + mucosae |
| Key clinical feature | Splenomegaly + pancytopenia | Painless ulcer with raised edges | Destructive nasal/oral lesions |
| Spontaneous healing? | No — fatal if untreated | Yes (most forms) | No |
| LD bodies visible in? | Bone marrow, spleen, lymph node | Skin biopsy | Mucosal biopsy |
| Serological tests useful? | Yes (rK39, DAT) | Limited | Limited |
Why It Matters: Pathogenesis
Why VL causes pancytopenia
Amastigotes multiply within macrophages of the bone marrow, suppressing normal haematopoiesis. Simultaneously, the massively enlarged spleen sequesters and destroys circulating blood cells (hypersplenism). The result — low RBCs (anemia), low WBCs (leucopenia), and low platelets (thrombocytopenia) — is pancytopenia. This is both a diagnostic clue and a treatment complication: the very drugs used to treat VL are toxic, and drug-induced haematological suppression in an already pancytopenic patient requires careful monitoring.
Why Indian kala-azar is uniquely anthroponotic
Unlike zoonotic VL (where animal reservoirs like dogs and jackals maintain transmission), Indian kala-azar (L. donovani on the subcontinent) has humans as the sole reservoir. This has two critical implications: first, early detection and treatment of human cases directly interrupts transmission; second, PKDL patients who appear cured but still carry the parasite in skin act as silent reservoirs sustaining the epidemic. The South Asian VL elimination programme depends on both active case detection and aggressive PKDL management.
Why the drugs used are dangerous
Antileishmanial drugs — historically pentavalent antimonials (sodium stibogluconate), now liposomal amphotericin B (first-line in South Asia) — are toxic. Cardiotoxicity, nephrotoxicity, and haematological suppression are real concerns. This is why diagnosis must be confirmed before treatment: the drugs are too dangerous to give empirically to asymptomatic seropositive individuals who may have latent infection rather than active disease.
Laboratory Diagnosis
Specimen Collection
| Disease form | Specimen | Notes |
|---|---|---|
| Visceral (VL) | Bone marrow aspirate (iliac crest), splenic aspirate, blood | Splenic aspirate highest sensitivity but greatest risk; bone marrow safest invasive option |
| Cutaneous (CL) | Skin slit smear or biopsy from ulcer edge | Sample from the indurated edge, not the necrotic centre |
| Mucocutaneous (MCL) | Biopsy of affected mucosal tissue |
For VL serology and molecular tests: venous blood (EDTA) or serum is sufficient — no invasive biopsy needed.
1. Microscopy — Demonstration of LD Bodies
The classic confirmatory test. Giemsa-stained aspirate from bone marrow, spleen, or lymph node is examined for amastigotes (LD bodies) inside macrophages.
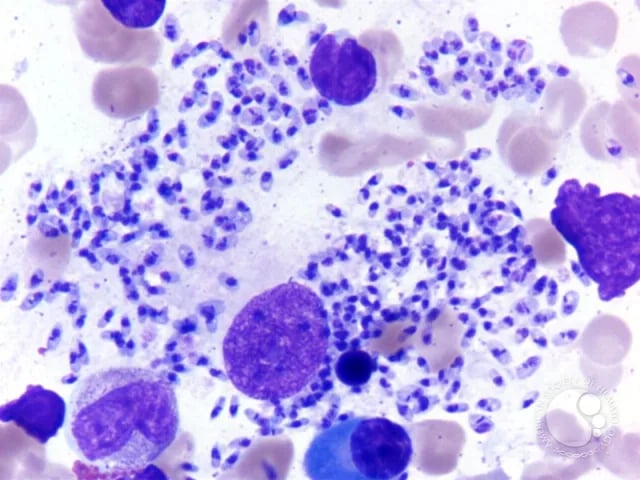 Figure: Heavy LD body infestation in bone marrow aspirate.
Figure: Heavy LD body infestation in bone marrow aspirate.
LD body morphology on Giemsa stain:
- Small oval bodies, 2–4 μm
- Large, prominent kinetoplast (a rod-shaped mitochondrial DNA structure that stains deeply — this is the diagnostic feature that distinguishes Leishmania amastigotes from other intracellular organisms)
- Found in clusters inside macrophages or free after cell rupture
Sensitivity by specimen site:
| Specimen | Sensitivity |
|---|---|
| Splenic aspirate | 93–99% — highest, but invasive and risky |
| Bone marrow aspirate | 53–86% — safer, standard in most settings |
| Lymph node aspirate | 53–65% — only if lymphadenopathy present |
| Blood buffy coat | Lower — useful in immunocompromised (HIV-VL co-infection) |
Specificity is high for all sites when LD bodies are identified — the kinetoplast is pathognomonic.
2. Culture — NNN Medium
The specimen is inoculated into NNN medium (Novy-MacNeal-Nicolle medium) — a biphasic medium with a blood agar base overlaid with Locke's saline solution. Leishmania promastigotes grow in the liquid overlay phase and can be seen motile under microscopy within 1–4 weeks.
Culture is more sensitive than microscopy but slower and requires a specialised laboratory. Used primarily for confirmation and species identification.
For NNN medium composition, preparation, and results, see: NNN Medium
3. Serological Tests
Antibody-based tests for VL (not reliable for CL or MCL — weak antibody response in localised disease).
rK39 Immunochromatographic Test (ICT) — Field Standard
The most important rapid test for VL diagnosis.
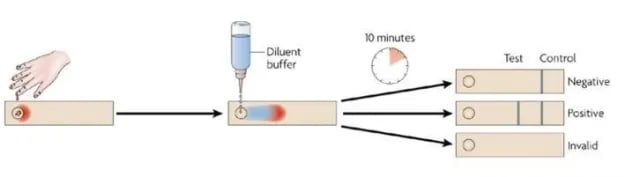 Figure: rK39 Test
Figure: rK39 Test
What is K39? K39 is a 39-amino-acid repeat epitope encoded by a kinesin-like gene, conserved on amastigotes of visceral Leishmania species. Anti-K39 IgG is produced in high titers specifically during active VL.
How it works: Recombinant K39 antigen is impregnated on a nitrocellulose strip. Patient blood or serum is applied; if anti-K39 IgG antibodies are present, they form a visible line within 5 minutes (immunochromatographic/lateral flow principle).
Performance:
- Sensitivity: 95–100% in most VL-endemic regions
- Specificity: 97–98%
- Result time: 5 minutes
- No laboratory or electricity needed — true point-of-care test
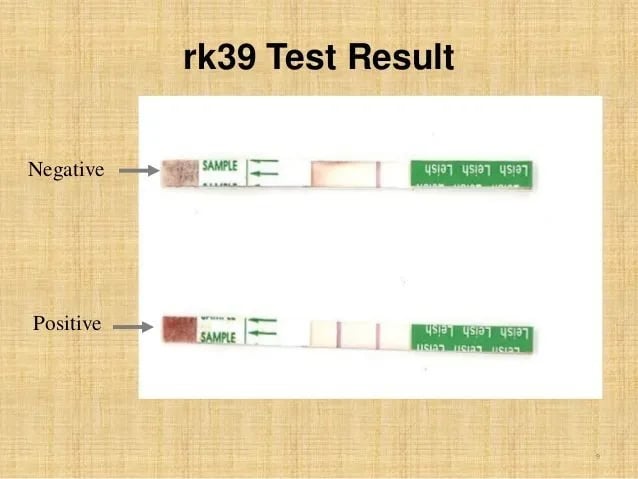 Figure: rK 39 test result for visceral leishmaniasis
Figure: rK 39 test result for visceral leishmaniasis
Critical limitation: rK39 sensitivity varies by geography. Performance is excellent on the Indian subcontinent and East Africa but lower in Brazil and the Mediterranean (where L. infantum causes VL). Additionally, anti-K39 antibodies persist for months to years after successful treatment — a positive rK39 alone cannot distinguish active from past VL in endemic areas. Clinical correlation is essential.
Direct Agglutination Test (DAT)
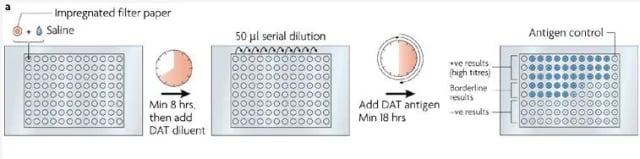 Figure: DAT Test for the diagnosis of Visceral Leishmaniasis
Figure: DAT Test for the diagnosis of Visceral Leishmaniasis
Uses trypsin-treated, formalin-fixed, Giemsa-stained promastigotes as antigen. Patient serum is serially diluted and mixed with antigen; visible agglutination at high dilutions (≥1:3200) indicates positive.
- Sensitivity and specificity comparable to rK39 in most studies
- Advantage: can detect all Leishmania species causing VL regardless of geography
- Disadvantage: requires refrigeration, longer procedure (18 hours), more technical skill; less suitable for field use than rK39
ELISA and IFA
High diagnostic accuracy but require laboratory infrastructure, electricity, and trained personnel. Used in reference laboratories and research; not suitable for field diagnosis.
Aldehyde (Formal Gel) Test — Historical
Add 1–2 drops of formalin to 1 mL patient serum. Positive result: gelation to a white opaque consistency (like hard-boiled egg white) within 3–24 hours.
Positive result reflects polyclonal hypergammaglobulinaemia (massive non-specific antibody production in active VL) — not specific to Leishmania. Sensitivity as low as 34%. Used historically as a cheap screening test; now replaced by rK39 in most endemic settings. Still taught in examinations.
Important limitation of all serology: Antibody-based tests cannot distinguish active VL from asymptomatic infection or past treated disease. A positive serology in an endemic area with no clinical signs does not warrant treatment with toxic antileishmanial drugs.
4. Leishmanin Skin Test (Montenegro Test)
Intradermal injection of killed promastigotes (0.1–0.2 mL containing 6–10 × 10⁶ promastigotes/mL). Induration ≥5 mm at 48–72 hours = positive.
What a positive result means: Cell-mediated immunity (delayed hypersensitivity) to Leishmania antigens — this develops after recovery from VL or in CL/MCL patients.
What a positive result does NOT mean: Active disease. The test is negative in active visceral leishmaniasis (the parasite suppresses cell-mediated immunity during active infection). It becomes positive only 6–8 weeks after cure.
Exam trap: A positive leishmanin test in a patient with suspected active VL argues against active VL, not for it.
Geographic variation: Positive in African kala-azar; negative in Indian and Mediterranean kala-azar (and PKDL). Positive in CL and MCL.
5. Antigen Detection
A heat-stable carbohydrate antigen of Leishmania is detectable by latex agglutination test in urine of VL patients. Useful for treatment monitoring (unlike antibody tests, antigen clears after successful treatment). Specificity is good but sensitivity is moderate (48–87%). Research-phase improvements ongoing.
6. Molecular Diagnosis (PCR)
PCR targeting kinetoplast DNA (kDNA) or ribosomal RNA genes can detect Leishmania in peripheral blood, aspirates, or skin biopsies with very high sensitivity (>95%) and can identify species. Used in reference laboratories for species identification, treatment monitoring, and diagnosis of difficult cases (immunocompromised patients, co-infections). Not yet standard in resource-limited field settings.
Diagnostic Algorithm for Suspected VL (LMIC Setting)
Suspected VL (fever >2 weeks + splenomegaly + LMIC endemic area)
↓
rK39 rapid test
↓
Positive + clinical features → Treat (confirm with BM aspirate if available)
Negative + high suspicion → Bone marrow aspirate (microscopy + culture)
Negative + low suspicion → Look for alternative diagnosis
In the Indian subcontinent elimination programme, rK39 + clinical case definition (fever >2 weeks + splenomegaly + endemic area + negative malaria test) is accepted as sufficient for treatment initiation at the primary health care level — invasive biopsy is not required unless rK39 is negative with persistent suspicion.
Epidemiology
- Endemic in >90 countries worldwide; 700,000–1 million new VL cases per year globally
- VL burden concentrated in: India, Bangladesh, Nepal (67% of global VL burden together), Sudan, Ethiopia, Brazil
- CL burden concentrated in: Afghanistan, Pakistan, Syria, Iran, Algeria, Saudi Arabia, Brazil, Peru (90% of global CL cases)
- Nepal epidemiology: Terai (lowland) districts are VL-endemic; mountainous regions >2,000 feet altitude are not affected (sandflies do not survive at altitude)
- Transmission season: Peak during and after monsoon — warm, humid conditions favour sandfly breeding
- Occupation and poverty: Strongest risk factors — agricultural workers, those living in mud-wall houses without window screens
Prevention and Control
Vector control:
- Residual insecticide spraying (DDT first choice for P. argentipes in South Asia — still susceptible; BHC as second line)
- Insecticide-treated bed nets (ITNs) — also reduce malaria and Japanese encephalitis concurrently
- Environmental management to eliminate sandfly breeding sites (cracks in walls, rubble piles)
Case detection and treatment:
- In anthroponotic VL (Indian subcontinent): treating human cases directly reduces the reservoir; active surveillance for PKDL is critical
- WHO VL elimination target for South Asia: <1 case per 10,000 population per block/upazila/union
No licensed vaccine available — multiple candidates in development.
How to Remember
The Three Forms — Mnemonic: **VCM — "Very Contagious Mucosal"**
- Visceral — L. donovani — internal organs — kala-azar
- Cutaneous — L. tropica/major — skin ulcer — oriental sore
- Mucocutaneous — L. braziliensis — destroys mucosa — espundia
LD Body Recognition
"Large kinetoplast in a Large Dong body" — LD stands for Leishman-Donovan; the kinetoplast is disproportionately large for the tiny amastigote, making it visible even at 100× oil immersion. If you see a small oval organism with a visibly large, dark rod-shaped inclusion inside a macrophage — that is your diagnostic clue.
rK39 Memory Hook
"K39 — Kala-azar's 39-amino-acid fingerprint" — K39 is unique to visceral Leishmania amastigotes. When the host makes antibodies to it, those antibodies are a specific marker of VL exposure.
Leishmanin Test Paradox
"Leishmanin is positive after, not during" — active VL suppresses CMI; the test turns positive only after recovery. A positive test means past infection or CL/MCL, not active VL.
Remembering Indian Kala-Azar Uniqueness
"India has no animal to blame" — Indian kala-azar is anthroponotic (humans are the sole reservoir). All other major VL foci have zoonotic animal reservoirs (dogs, jackals, foxes).
Where Students Actually Get Confused
1. "rK39 positive = active VL, start treatment." Not automatically. Anti-K39 IgG persists for months to years after cure. In a highly endemic area, a seropositive asymptomatic person should not be treated — the drugs are too toxic. Diagnosis requires clinical case definition + serology, not serology alone.
2. "The leishmanin test diagnoses active VL." The opposite is true. Active VL suppresses T-cell mediated immunity — the test is negative in active disease and only turns positive weeks after recovery. Positive leishmanin = past infection/cured VL or CL/MCL, not active kala-azar.
3. "Splenic aspirate is the best and safest specimen." Splenic aspirate has the highest sensitivity (93–99%) but it carries a real risk of fatal haemorrhage in a patient with thrombocytopenia — which most VL patients have. Bone marrow aspirate (sensitivity 53–86%) is the standard invasive method in most settings because it is safer.
4. "LD bodies are specific to kala-azar." LD bodies (amastigotes) are found in all three forms of leishmaniasis and in other related trypanosomatid infections. The specificity comes from the combined morphology (small oval + prominent kinetoplast + intracellular location in macrophages) and the clinical-epidemiological context.
5. "Promastigote is the form found in humans." Promastigotes are found in the sandfly vector. Humans harbour amastigotes. Promastigotes are the form that grows in NNN culture medium and in sandfly salivary glands. The infective form injected into humans during a sandfly bite is the metacyclic promastigote, which then converts to amastigotes inside human macrophages.
6. "The aldehyde test is specific for leishmaniasis." No — it detects non-specific polyclonal hypergammaglobulinaemia, which occurs in many chronic infections and inflammatory conditions. Low sensitivity (34%) and no species specificity. It is a historical test, still taught because it remains in curricula, but rK39 has replaced it in clinical practice.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Definitive host | Female phlebotomine sandfly (Phlebotomus spp. Old World; Lutzomyia spp. New World) | Sandfly = definitive (infective stage develops here) |
| Intermediate host | Humans and other mammals | Amastigotes replicate here |
| Amastigote form | Intracellular in macrophages; has prominent kinetoplast | LD body — "Large kinetoplast" |
| Promastigote form | In sandfly; elongated with flagellum | Grows in NNN medium |
| VL causative species (South Asia) | L. donovani | Kala-azar; anthroponotic on Indian subcontinent |
| CL causative species (Old World) | L. tropica, L. major | Oriental sore |
| MCL causative species | L. braziliensis | Espundia — destroys nose and mouth |
| Indian kala-azar reservoir | Humans only (anthroponotic) | "India has no animal to blame" |
| VL clinical triad | Prolonged fever + massive splenomegaly + weight loss | + pancytopenia on blood count |
| PKDL | Skin lesions after VL treatment; important transmission reservoir | Occurs months–years post treatment |
| Gold standard invasive test | Bone marrow aspirate microscopy (LD bodies) | Spleen more sensitive but dangerous |
| Best field rapid test | rK39 ICT | 5 minutes; 95–100% sensitivity in South Asia |
| rK39 limitation | Stays positive months–years after cure | Cannot confirm active vs past disease alone |
| DAT | Agglutination of fixed promastigotes; useful pan-geographic | Needs refrigeration; 18-hour procedure |
| Aldehyde test | Positive = hypergammaglobulinaemia; 34% sensitivity | Historical; non-specific |
| Leishmanin test | NEGATIVE in active VL; POSITIVE after cure | "Positive after, not during" |
| NNN medium | Culture medium; promastigotes grow in liquid overlay | Also check: [NNN medium article] |
| Altitude restriction (Nepal) | VL not found above 2,000 feet | Sandflies cannot survive at altitude |
Self-Check Questions
- A patient presents with 8 weeks of fever, gross splenomegaly, weight loss, and pancytopenia. He is from the Terai belt of Nepal. An rK39 test is positive. What is the diagnosis, and is the rK39 result alone sufficient to start treatment?
- A skin test for Leishmania (leishmanin test) returns positive in a patient you suspect has active kala-azar. Does this support or argue against active VL?
- Which Leishmania species causes destructive lesions of the nasal septum and palate, and what is the disease called?
- Why is splenic aspirate the most sensitive but not the first-choice specimen for VL diagnosis?
- A patient treated for VL 18 months ago is now asymptomatic. An rK39 test at a routine check is positive. Does this indicate treatment failure or relapse?
- What is the morphological feature that distinguishes a Leishmania amastigote from other small intracellular organisms on Giemsa stain?
- What is PKDL, why does it matter for the VL elimination programme, and when does it occur?
- Name the two forms of Leishmania and state which host each is found in.
Answers:
- Visceral leishmaniasis (kala-azar). In the Indian subcontinent elimination programme, rK39 + clinical case definition is accepted for treatment initiation, but ideally confirm with bone marrow aspirate if feasible and if clinical features are consistent. Serology alone is insufficient in endemic areas due to seroprevalence.
- Argues against — active VL suppresses CMI; leishmanin is negative during active disease and turns positive 6–8 weeks after recovery.
- L. braziliensis; mucocutaneous leishmaniasis (espundia).
- Splenic aspirate has 93–99% sensitivity but carries a risk of fatal haemorrhage in thrombocytopenic VL patients; bone marrow aspirate (53–86% sensitivity) is safer and the standard invasive procedure.
- Not necessarily — anti-K39 antibodies persist for months to years after successful treatment. Active relapse would require clinical features (fever, splenomegaly) + repeat serology correlation or parasitological confirmation.
- Prominent kinetoplast — a large, rod-shaped, deeply staining mitochondrial DNA structure visible even in the tiny (2–4 μm) amastigote.
- PKDL = post-kala-azar dermal leishmaniasis; hypopigmented skin lesions appearing months–years after VL treatment; patients carry amastigotes in skin and act as transmission reservoirs, potentially restarting the VL cycle; critically important for the South Asian elimination programme.
- Amastigote = in humans (and other mammalian hosts), inside macrophages; Promastigote = in the sandfly vector.)
References
- Maxfield, L., & Crane, J. S. (2023). Leishmaniasis. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK531456/
- Torres-Guerrero, E., Quintanilla-Cedillo, M. R., Ruiz-Esmenjaud, J., & Arenas, R. (2017). Leishmaniasis: a review. F1000Research, 6, 750. https://doi.org/10.12688/f1000research.11120.1
- Stockdale, L., & Newton, R. (2013). A review of preventative methods against human leishmaniasis infection. PLOS Neglected Tropical Diseases, 7(6), e2278. https://doi.org/10.1371/journal.pntd.0002278
- Sundar, S., & Rai, M. (2002). Laboratory diagnosis of visceral leishmaniasis. Clinical and Diagnostic Laboratory Immunology, 9(5), 951–958. https://doi.org/10.1128/cdli.9.5.951-958.2002
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- Sastry, A. S., & Bhat, S. (2014). Essentials of Medical Parasitology. Jaypee Brothers Medical Publishers.
- World Health Organization. (2023). Leishmaniasis. WHO Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/leishmaniasis
Frequently Asked Questions
What is the difference between visceral, cutaneous, and mucocutaneous leishmaniasis?
What are LD bodies and where are they found?
What is the rK39 test and how is it used for kala-azar diagnosis?
What is the leishmanin skin test and what does a positive result mean?
Why is Indian kala-azar called anthroponotic?
What is PKDL and why is it important?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.