Dengue Virus: Why Second Infections Are More Dangerous and How Lab Diagnosis Works
How antibody-dependent enhancement makes secondary dengue infection more severe, and which test; NS1, IgM, IgG, or PCR — to use and when.
Most viral infections follow a predictable immunological pattern: get infected once, recover, and the immune system's memory protects you from the same pathogen in the future. Dengue deliberately breaks this pattern. A person who recovers from their first dengue infection is not more protected against a second infection with a different serotype; they are, paradoxically, at significantly higher risk of the second infection becoming the severe form that causes dengue hemorrhagic fever.
The reason is a mechanism called antibody-dependent enhancement: the antibodies made against the first serotype are cross-reactive but non-neutralizing against a different serotype. Instead of blocking the second virus, these antibodies coat it and facilitate its entry into monocytes and macrophages via Fc receptors. The result is a much higher viral load, amplified inflammation, and the vascular damage that defines severe dengue.
This single mechanism explains why dengue has four serotypes (each exposure only partially changes the risk landscape), why sequential serotype exposure matters more than the absolute number of infections, why children in dengue-endemic regions have higher severe-disease rates than adults in first-exposure situations, and why a dengue vaccine that doesn't confer protection equivalent to natural infection in seronegative recipients can actually cause harm rather than prevent it. Understanding this mechanism is the key to understanding everything in this article that follows.
 Figure: Aedes aegypti mosquito is the main vector of dengue
Figure: Aedes aegypti mosquito is the main vector of dengue
Dengue is transmitted via the bite of an infected female Aedes aegypti mosquito. Globally, 2.5 billion people live in areas where dengue viruses can be transmitted. Cases of this disease are seen in tropical and sub-tropical climates worldwide, mostly in urban and semi-urban areas.
Properties
- It is composed of single-stranded RNA (SSRNA).
- It has four distinct but closely related serotypes DEN-1, DEN-2, DEN-3, and DEN-4. Subsequent infections by other serotypes increase the risk of developing severe dengue.
Structure and Family Classification
Dengue virus belongs to the family Flaviviridae, genus Flavivirus — a family that includes several other clinically important arboviruses: Japanese encephalitis virus, Zika virus, West Nile virus, and yellow fever virus. Understanding this family membership is useful because it explains shared features that appear in the diagnostic and serological sections below:
- Genome: Single-stranded, positive-sense RNA (~11 kb), encoding three structural proteins (C, prM/M, E) and seven non-structural proteins (NS1–NS5)
- Envelope: Present; icosahedral nucleocapsid enclosed by a lipid envelope with E (envelope) glycoprotein spikes
- E protein: The main surface antigen; the target of neutralising antibodies; responsible for receptor binding and membrane fusion during cell entry
- NS1 protein: Non-structural protein 1 secreted in large quantities by infected cells; detectable in blood during the acute viremic phase; the target of the NS1 antigen rapid diagnostic test
- Serotypes: Four distinct serotypes (DENV-1, 2, 3, 4) with approximately 25–40% amino acid divergence in the E protein — enough that antibodies against one serotype do not reliably neutralise others, the root cause of ADE
The flavivirus family connection also explains the cross-reactivity problem in dengue serology: IgG antibodies against dengue can produce false-positive results in tests for Zika, West Nile, or Japanese encephalitis, and vice versa. Serotyping by RT-PCR rather than serology is needed when distinguishing between co-circulating flaviviruses matters clinically.
Transmission
This disease is the most common mosquito-borne viral disease in humans. The virus is transmitted to humans through the bites of infected female mosquitoes. Aedes aegypti mosquito, a daytime feeder mosquito, is the primary vector.
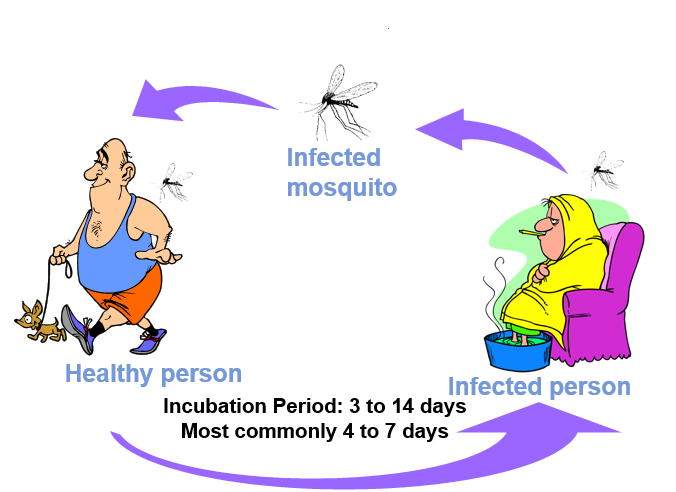 Figure: Transmission of dengue viral infection
Figure: Transmission of dengue viral infection
Aedes albopictus is a secondary dengue vector. These species are active for approximately two hours after sunrise and several hours before sunset but can bite at night in well-lit areas. This mosquito can bite people without being noticed because it approaches from behind and bites on the ankles and elbows.
Clinical Findings
The clinical disease begins 4-7 days (3-14 days) after an infective mosquito bite.
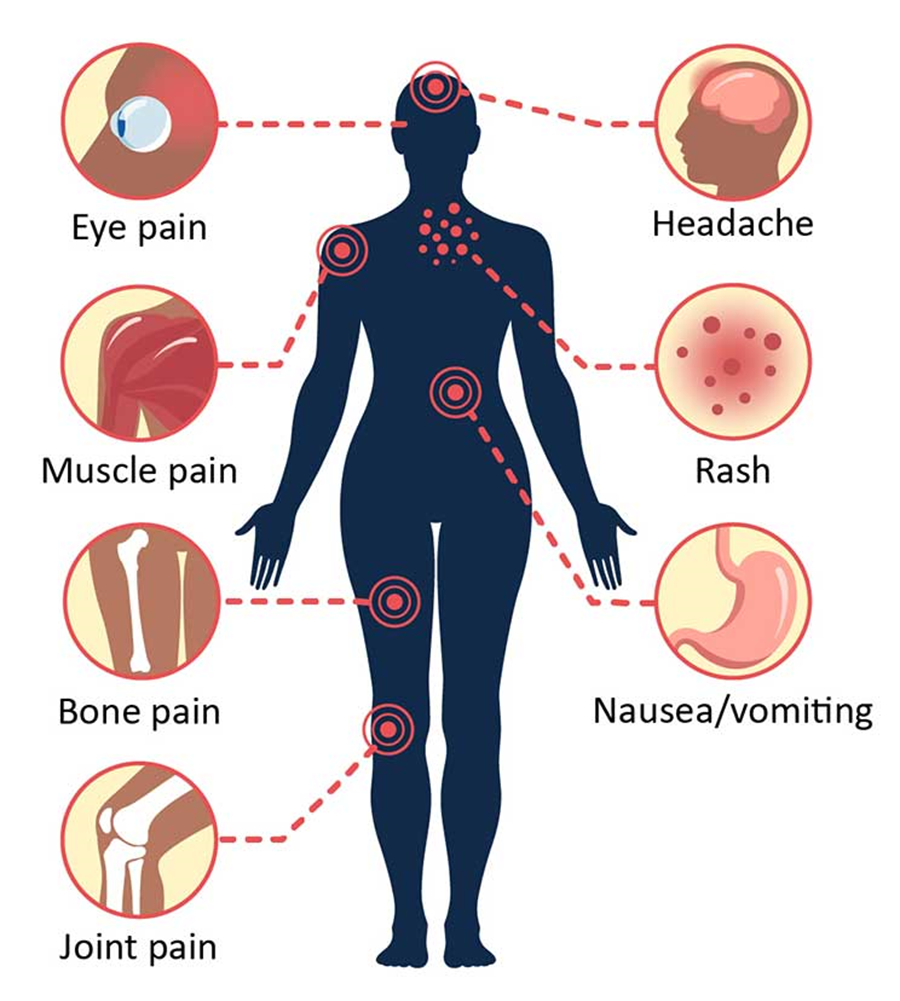 Figure: Symptoms of dengue viral infection
Figure: Symptoms of dengue viral infection
Clinical signs/ symptoms:
- Fever, malaise, chills, headache, pain behind the eyes
- Characteristic deep bone pain and myalgia
- Enlargement of lymph nodes.
- Classic dengue fever is a self-limited disease
- Secondary infection with any dengue serotype different from the first is a risk factor for severe disease due to antibody-dependent enhancement (ADE) — not just type 2 following type 1. The highest DHF risk is observed in certain sequential combinations (particularly DENV-1 followed by DENV-2 in some endemic settings), but all heterologous secondary infections carry elevated risk.
Classical dengue fever is a mild illness, but DHF and dengue shock syndrome (DSS) are severe forms of the disease. Severe dengue is a leading cause of hospitalization and death among children. Immunity after recovery is lifelong for that serotype but partial and temporary for others.
- Serious life-threatening condition
- Children mostly affected
- In those who have previously been infected by one serotype and subsequently infected by another serotype
- Antibody-dependent enhancement (ADE): The key mechanism of severe dengue. During a secondary infection with a different serotype, pre-existing IgG antibodies from the first infection bind to the new serotype virus but cannot neutralise it (the E protein is too different). These antibody-coated virus particles bind Fc receptors on monocytes and macrophages, facilitating viral entry into these cells. The result is dramatically amplified viral replication in monocytes and macrophages, producing a cytokine storm, vascular endothelial damage, increased capillary permeability, plasma leakage, and thrombocytopenia. DIC and spontaneous bleeding follow in severe cases.
- In some patients, DHF progresses to circulatory collapse (Dengue shock syndrome)
- Mortality rate: up to 10–40% if untreated or inadequately managed; with appropriate fluid resuscitation and monitoring in experienced centres, case fatality rates are typically below 1–2%.
Host Immune Response
Primary response
- IgM antibodies appear about 5 days after symptoms onset and continue to rise to 21 days and decrease gradually.
- IgG antibodies appear about 14 days after symptoms onset and persist at a low level for life.
Secondary response
- Weaker and shorter IgM response
- Rapid IgG response (usually 2 days after reinfection)
- High IgG level persists for 30-40 days
Laboratory Diagnosis
- Platelet count: significantly reduced in DHF (100X109/l)
- Haematocrit (PCV): Rise (>20% in some cases)
- White cell count and differential count: Variable; Leucopenia common with blood film may show reactive lymphocytes.
- Coagulation (in DHF)
Bleeding and clotting time is prolonged Prothrombin and thromboplastin time increased Fibrinogen levels decreased
- Serum aminotransferases and blood urea: raised
- Serum sodium and albumin reduced
- Albuminuria and Hematuria present in some patients
Laboratory diagnosis method for confirming dengue viral infection involves using one or a combination of any of the following four methods.
- Microscopy and staining
- Culture
- Serology
Detection of antigen Detection of antibody
- Molecular diagnosis
Note: These methods are used for diagnosing any infections (viral, bacterial, parasitic, or fungal). The relative importance of a particular method differs among infections. Students are expected to know the main diagnostic test(s) of the particular infection.
Sample
- Early stages of the disease: after the onset of illness, the virus can be detected in blood (serum, plasma) or tissues; methods employed are; virus isolation, nucleic acid, or antigen detection.
- Serology is the method of choice at the end of an acute phase of infection.
| Highly Suggestive | Confirmed |
|---|---|
| One of the following: IgM + in a single serum sample IgG + in a single serum sample with a HI titer of 1280 or greater | One of the following: PCR + Virus culture + IgM seroconversion in paired sera IgG seroconversion in paired sera or fourfold IgG titer increase in paired sera |
Note: For virus culture, it is important to keep blood samples cooled or frozen to preserve the viability of the virus during transport from the patient to the laboratory.
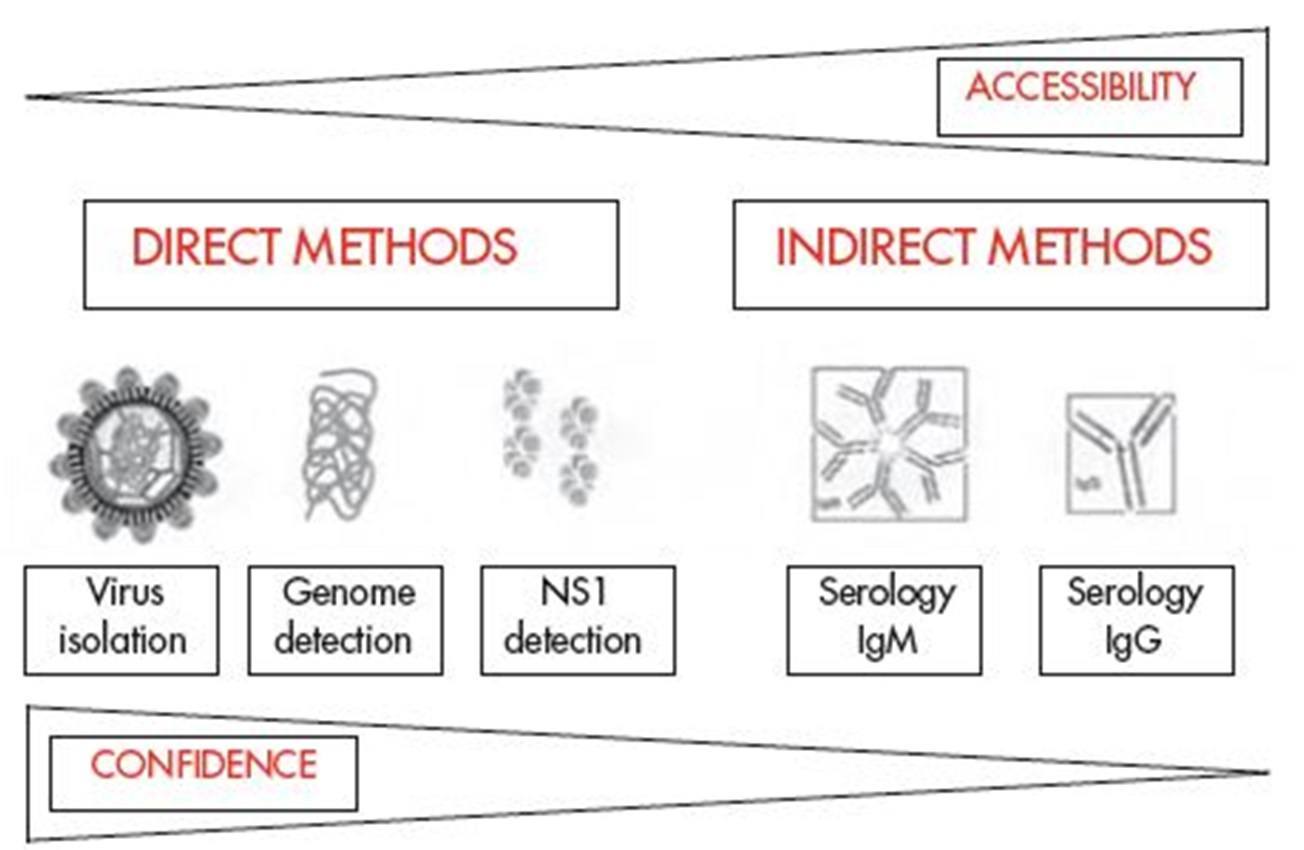 Figure: Fig 1: Comparison of dengue virus diagnostic tests according to their accessibility and confidence
Figure: Fig 1: Comparison of dengue virus diagnostic tests according to their accessibility and confidence
- Microscopy and staining: Direct visualization of the virus in the sample (using electron microscopy or via fluorescent staining technique) can be done. This is not the preferred method in diagnostic laboratories.
- Culture: Virus isolation in cell culture is difficult and is not the commonly used method in diagnostic laboratories because it is a demanding procedure (both in terms of infrastructure and technical expertise). Virus may be recovered from serum, plasma, and peripheral blood mononuclear cells. Inoculation of a mosquito cell line with patient serum, coupled with nucleic acid assays to identify the recovered virus is a commonly used approach in the research lab.
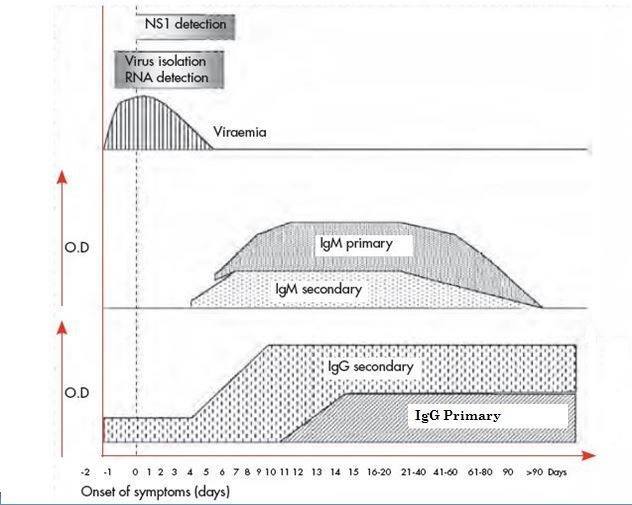 Figure: Fig 2:Approximate time-line of primary and secondary dengue virus infections and the diagnostic methods that can be used to detect infection
Figure: Fig 2:Approximate time-line of primary and secondary dengue virus infections and the diagnostic methods that can be used to detect infection
**Serological test:**Serological tests are the mainstay in the diagnosis of viral infections.
- Detection of viral antigen:
Dengue NS1 antigen detection is useful for the diagnosis of acute dengue infections up to 0-7 days of symptoms but not recommended after 7 days. NS1 antigen has been detected in the serum of DENV infected patients as early as 1-day post-onset of symptoms (DPO), and up to 18 DPO. NS1 ELISA based antigen assay is commercially available NS1 assay may also be useful for differential diagnostics between flaviviruses because of the specificity of the assay.
- Result interpretation
A positive NS1 test result confirms dengue virus infection but does not provide serotype information. A negative NS1 test result does not rule out infection. People with negative NS1 results should be tested for the presence of dengue IgM antibodies to determine possible recent dengue exposure.
Detection of anti-dengue antibodies in serum or other body fluids by ELISA or other rapid tests. Various methods(IgM/IgG ELISA, Hemagglutination Inhibition Test, or rapid diagnostic kits) are available to detect anti-dengue antibodies; IgM detection:
- Useful for the diagnosis of primary dengue infection and in distinguishing dengue from other flavivirus infections.
- IgM antibodies are detectable in 99% of patients by day 10 after the onset of illness.
- IgM levels peak about two weeks after the onset of symptoms and then decline to undetectable levels over 2–3 months.
- Sensitivity: 65–75% sensitive in a single acute serum sample collected after day 5 of illness. Before day 5, IgM sensitivity is lower; NS1 antigen detection or RT-PCR are more appropriate in the early acute phase.
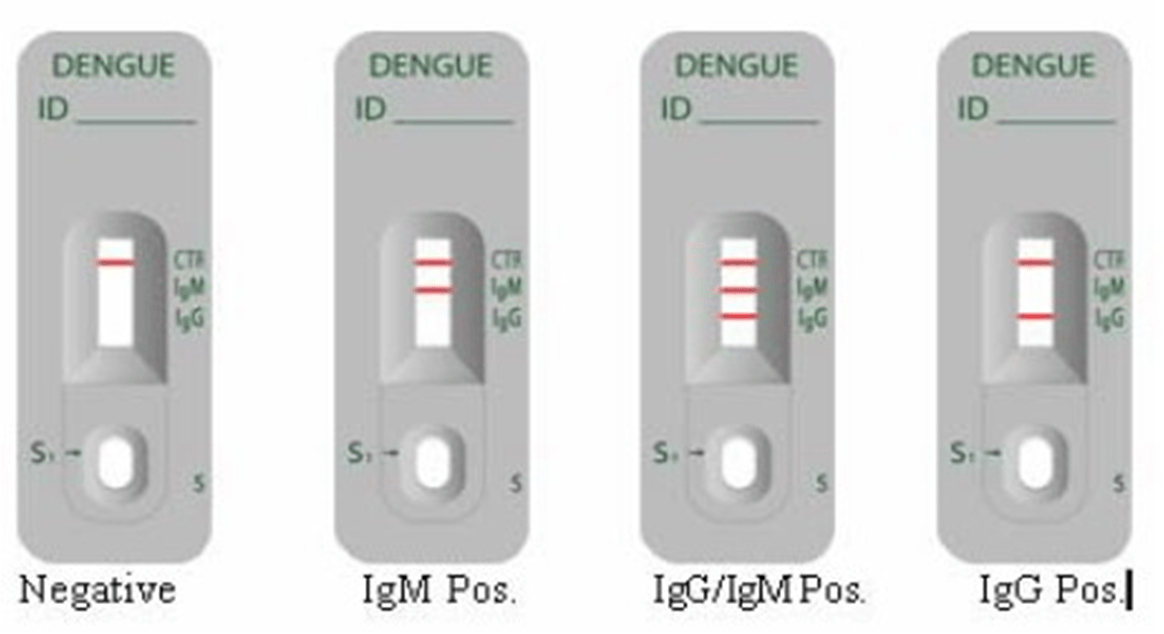 Figure: Fig 3:Rapid ICT based Test for the diagnosis of Dengue Infection
Figure: Fig 3:Rapid ICT based Test for the diagnosis of Dengue Infection
IgG detection: Tests that detect IgG are useful in diagnosing secondary disease (IgG is the dominant immunoglobulin type in secondary infection). The test is complicated by cross-reactivity of IgG antibodies to heterologous flavivirus antigens (West Nile virus, tick-borne encephalitis virus, yellow fever virus, zika virus). **Note:**To distinguish between primary and secondary dengue infections, IgM/IgG antibody ratios are now more commonly used than the hemagglutination-inhibition test (HI).
Molecular diagnosis: detection of viral RNA in plasma or serum or tissues using nucleic acid amplification test (NAAT). RT-PCR based methods for rapid identification and serotyping of dengue virus in acute phase serum are available.
Interpretation of Dengue Diagnostic Tests:
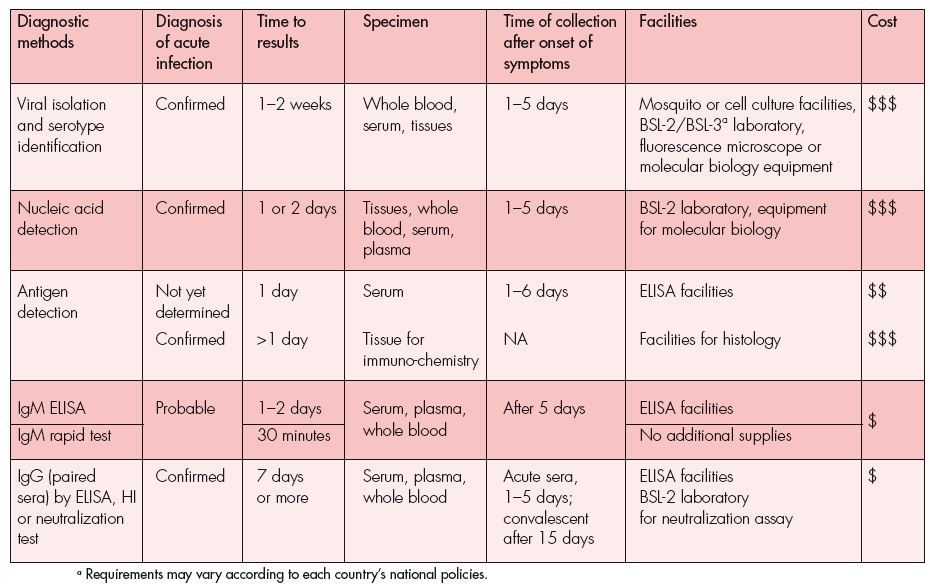 Figure: Fig 4:Summary of operating characteristics and comparative costs of dengue diagnostic methods.
Figure: Fig 4:Summary of operating characteristics and comparative costs of dengue diagnostic methods.
Treatment and Management
There is no specific approved antiviral drug for dengue. Management is supportive and based on careful clinical and laboratory monitoring:
Uncomplicated dengue fever (DF):
- Oral hydration, rest, paracetamol for fever and pain
- NSAIDs and aspirin are contraindicated — they inhibit platelet function and increase bleeding risk, both of which can worsen DHF if the patient progresses
- Monitor platelet count and haematocrit daily during the critical phase (days 3–7 of illness), when plasma leakage risk is highest
Dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS):
- Hospitalisation for careful IV fluid resuscitation — the goal is to replace plasma loss while avoiding fluid overload; this requires close monitoring of haematocrit and urine output
- Platelet transfusion is not routinely recommended unless there is active significant bleeding (not just low platelet count); prophylactic platelet transfusion is avoided
- Vasopressors in refractory shock
The critical phase and its diagnostic relevance: The critical phase (approximately days 3–7) is when plasma leakage peaks, platelet count is at its lowest, and the risk of haemorrhage and shock is highest. This is also when IgM antibodies begin to appear (detectable in most patients by day 5–10) and NS1 antigen begins to decline. Understanding this timing directly informs which diagnostic test should be ordered when — covered in detail in the Laboratory Diagnosis section above.
Dengue vaccine (Dengvaxia) — a critical teaching point: The first licensed dengue vaccine (CYD-TDV, Dengvaxia, Sanofi Pasteur) demonstrated that vaccination of dengue-seronegative individuals actually increased the risk of severe dengue on subsequent natural infection — because the vaccine generated cross-reactive, non-neutralising antibodies (essentially mimicking a primary infection and priming the ADE mechanism described above). WHO now recommends pre-vaccination serological screening to confirm prior dengue exposure before vaccination, and Dengvaxia is recommended only for seropositive individuals aged 9–45 years. This real-world vaccine complication is one of the most powerful demonstrations of the ADE mechanism's clinical significance.
How to Remember
"Four serotypes, four chances to get DHF." The fundamental risk architecture of dengue: the first infection with any serotype usually causes relatively mild disease and builds serotype-specific immunity. Each subsequent infection with a different serotype carries the ADE risk. In theory, a person could have four dengue infections, each with progressively higher ADE risk (though by the fourth, they should have broad cross-reactive immunity). In endemic regions, children sequentially exposed to multiple serotypes accumulate this risk profile over years.
NS1 early, IgM middle, IgG late — the diagnostic timeline in three phases. NS1 antigen is detectable from day 1 and declines after day 7 — it's the early acute marker. IgM appears from around day 5 and peaks at 2 weeks — it's the convalescent primary-infection marker. IgG rises rapidly in secondary infection (detectable within 1–2 days of symptom onset) and persists for life — it's the past-exposure/secondary-infection marker. If you overlay these three phases onto the clinical disease timeline (febrile phase days 1–3, critical phase days 4–7, recovery phase days 8+), the choice of diagnostic test at each visit becomes logical rather than a list to memorise.
IgM high = primary infection; IgG high from day 1 = secondary infection. In primary dengue, IgM rises first and IgG follows slowly. In secondary dengue, IgG dominates from the very beginning (anamnestic response — the immune system has seen dengue before and immediately switches to IgG production). The IgM/IgG ratio is the serological marker used to distinguish them: high IgM relative to IgG = primary; high early IgG relative to IgM = secondary and therefore higher risk of DHF.
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Family / Genus | Flaviviridae / Flavivirus |
| Genome | ss(+)RNA, ~11 kb |
| Envelope | Present; E glycoprotein spikes; NS1 secreted extracellularly |
| Serotypes | 4 (DENV-1, 2, 3, 4) — prior infection with one does not reliably neutralise others |
| Primary vector | Aedes aegypti (daytime feeder); secondary: Aedes albopictus |
| Incubation period | 3–14 days (typically 4–7 days) |
| Classic dengue fever triad | High fever + severe bone/muscle pain ("breakbone fever") + rash |
| ADE mechanism | Cross-reactive non-neutralising IgG from prior serotype facilitates viral entry into Fc-receptor-bearing monocytes → amplified replication → DHF |
| DHF hallmarks | Plasma leakage (rising haematocrit), thrombocytopenia, haemorrhagic manifestations |
| Critical phase timing | Days 3–7 of illness |
| NSAIDs/aspirin in dengue | Contraindicated — increases bleeding risk |
| NS1 antigen window | Days 0–7 (useful for early acute diagnosis) |
| IgM window | Detectable from day 5; peaks at ~2 weeks; declines by 2–3 months |
| IgG in secondary infection | Detectable within 1–2 days of symptom onset (rapid anamnestic response) |
| IgM/IgG ratio | High IgM relative to IgG = primary infection; high early IgG = secondary infection |
| RT-PCR utility | Detects and serotypes virus in early acute phase (days 1–5); not useful after day 7 |
| No specific antiviral | Treatment is supportive; careful fluid management is the cornerstone of DHF management |
| Dengvaxia restriction | Recommended only for seropositive individuals (seronegative vaccination increases DHF risk via ADE) |
Where Students Get Confused
"Prior dengue infection protects you from severe dengue." This is the reverse of reality. Prior infection with one serotype puts you at higher risk of DHF on exposure to a different serotype — precisely because of the ADE mechanism. The cross-reactive, non-neutralising IgG from the first infection enhances viral entry in the second. In a dengue-endemic area, children who have experienced a first dengue infection are at higher risk of severe disease if they encounter a different serotype — not lower risk.
"A negative NS1 test rules out dengue." It does not. NS1 sensitivity declines after day 7 and is lower in secondary infections (possibly because antibodies form immune complexes with NS1 and reduce its free detection). A negative NS1 with ongoing dengue suspicion should prompt IgM/IgG testing or RT-PCR depending on the day of illness.
"High IgG means past, resolved dengue — not current infection." In secondary dengue infection, IgG rises dramatically within the first 1–2 days of illness (anamnestic immune response). High IgG early in the febrile phase is actually a marker of secondary dengue infection and correlates with higher severe-disease risk, not simply with "past exposure." Context and timing matter for interpreting IgG results.
"Platelet transfusion should be given whenever the platelet count is low in DHF." Current WHO guidelines do not recommend prophylactic platelet transfusion for low counts alone. Platelet transfusion is reserved for patients with active significant bleeding. Over-reliance on prophylactic transfusion adds risks (transfusion reactions, fluid overload) without demonstrated benefit for uncomplicated thrombocytopenia in dengue.
"Cross-reactivity in flavivirus serology only matters for rare imported infections." In settings where dengue, Japanese encephalitis, and Zika co-circulate (South and Southeast Asia, parts of the Pacific — directly relevant to this site's India and Philippines audience), cross-reactive IgG can produce false-positive results across flavivirus serological assays. RT-PCR or plaque reduction neutralisation tests (PRNT) are needed to confirm the specific infecting flavivirus when clinical differentiation matters.
References and Further Readings:
- World Health Organization. (2023). Dengue and severe dengue: Key facts and clinical management. WHO. https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (Verify current URL in CMS before inserting.)
- Guzman, M. G., Gubler, D. J., Izquierdo, A., Martinez, E., & Halstead, S. B. (2016). Dengue infection. Nature Reviews Disease Primers, 2, 16055. https://doi.org/10.1038/nrdp.2016.55
- Paz-Bailey, G., Adams, L. E., Deen, J., Anderson, K. B., & Katzelnick, L. C. (2024). Dengue. The Lancet, 403(10427), 667–682. https://doi.org/10.1016/S0140-6736(23)01687-0
- Halstead, S. B. (2014). Dengue antibody-dependent enhancement: Knowns and unknowns. Microbiology Spectrum, 2(6), AID-0022-2014. https://doi.org/10.1128/microbiolspec.AID-0022-2014
- World Health Organization. (2018). Dengue vaccines: WHO position paper — September 2018. Weekly Epidemiological Record, 93(36), 457–476. https://apps.who.int/iris/handle/10665/274315
Frequently Asked Questions
Why is a second dengue infection more dangerous than the first?
Which dengue diagnostic test should be ordered on day 3 of illness versus day 10?
Why is aspirin contraindicated in dengue?
Why was the Dengvaxia vaccine found to be harmful in some recipients?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.