Japanese Encephalitis Virus: Why It Targets the Thalamus and How to Diagnose It
How JEV crosses from a mosquito bite to the thalamus, why it causes a Parkinsonian syndrome, and why CSF IgM is the key diagnostic test.
A child in rural Nepal presents in August with sudden high fever, altered consciousness, and involuntary movements that look almost like Parkinson's disease; tremors, cogwheel rigidity, masklike facies. The working diagnosis before laboratory results: Japanese encephalitis. The family wants to know how a mosquito bite caused their child's brain to stop working the way it should.
Japanese encephalitis virus (JEV) infects tens of millions of people every year across Asia and the western Pacific and the vast majority never know it. Fewer than one in 200 JEV infections causes any clinical disease; most are completely asymptomatic. But when JEV does reach the brain, the consequences are severe: approximately 20-30% of clinical cases die, and 30–50% of survivors are left with permanent neurological or psychiatric complications. That combination — rare clinical disease but devastating outcomes when it occurs — is what makes JEV the leading cause of vaccine-preventable encephalitis worldwide.
Understanding JEV requires two things beyond the clinical checklist: knowing how the virus travels from the mosquito bite site to a specific region of the brain (not random JEV has a particular tropism that explains the clinical presentation directly), and understanding why children bear the burden of disease in endemic areas while adults are largely protected. Both are answered by the pathogenesis section below.
 Figure: mosquito
Figure: mosquito
The virus is maintained in an enzootic cycle between mosquitoes and amplifying vertebrate hosts (mainly pigs). The highest risk months for JE transmission are August, September, and early October.
Properties of JE Virus
- member of the family flaviviruses
- Related to dengue, yellow fever, Zika, and West Nile viruses — all Flaviviridae. This shared family membership produces cross-reactive antibodies that can complicate serological diagnosis in areas where multiple flaviviruses co-circulate, a clinically important point for Nepal, India, and the Philippines where both JEV and dengue are endemic
- +ve stranded SS RNA Virus
- linear non-segmented genomes
- icosahedral shaped
- envelope is present
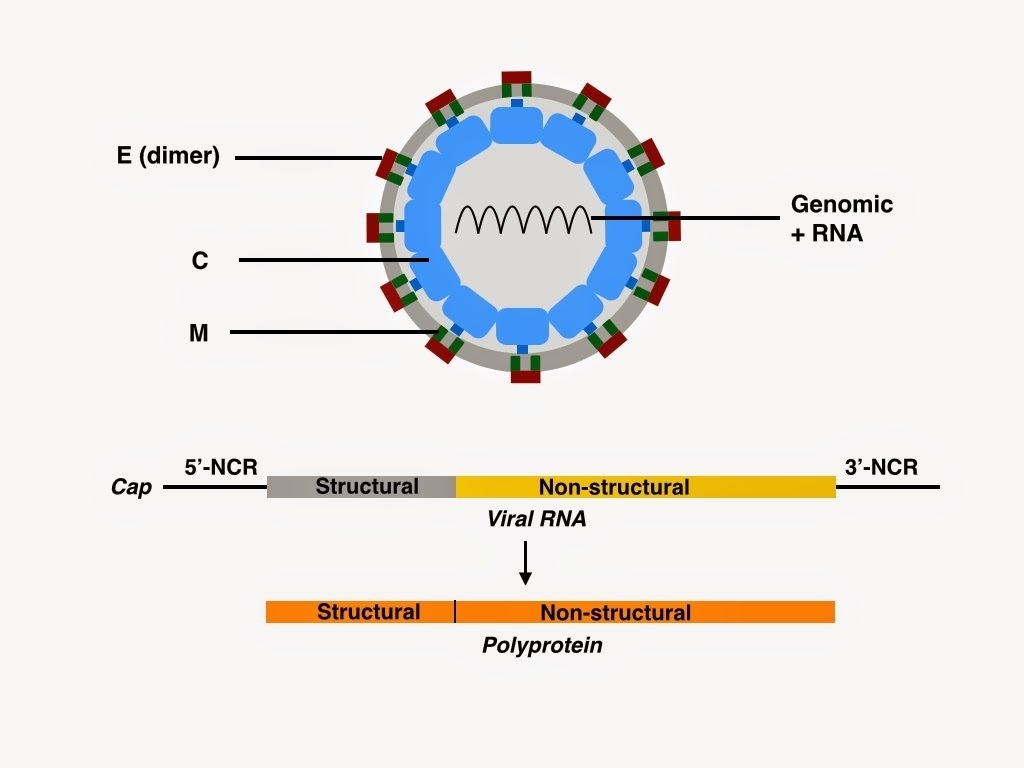 Figure: Structure of Japanese encephalitis virus (JEV)
Figure: Structure of Japanese encephalitis virus (JEV)
Transmission Cycle of Japanese Encephalitis Virus
- Domestic pigs and wild birds are reservoirs of the virus
- Virus exists in a transmission cycle between mosquitoes, pigs, and/or water birds (enzootic cycle).
- Spread by the bite of infected mosquitoes, primarily Culex spp (Culex tritaeniorhynchus).
- Human are incidental dead-end hosts. JE virus can not spread directly from person to person. Humans once infected do not develop enough concentration of the JE virus in their bloodstream to infect feeding mosquitoes.
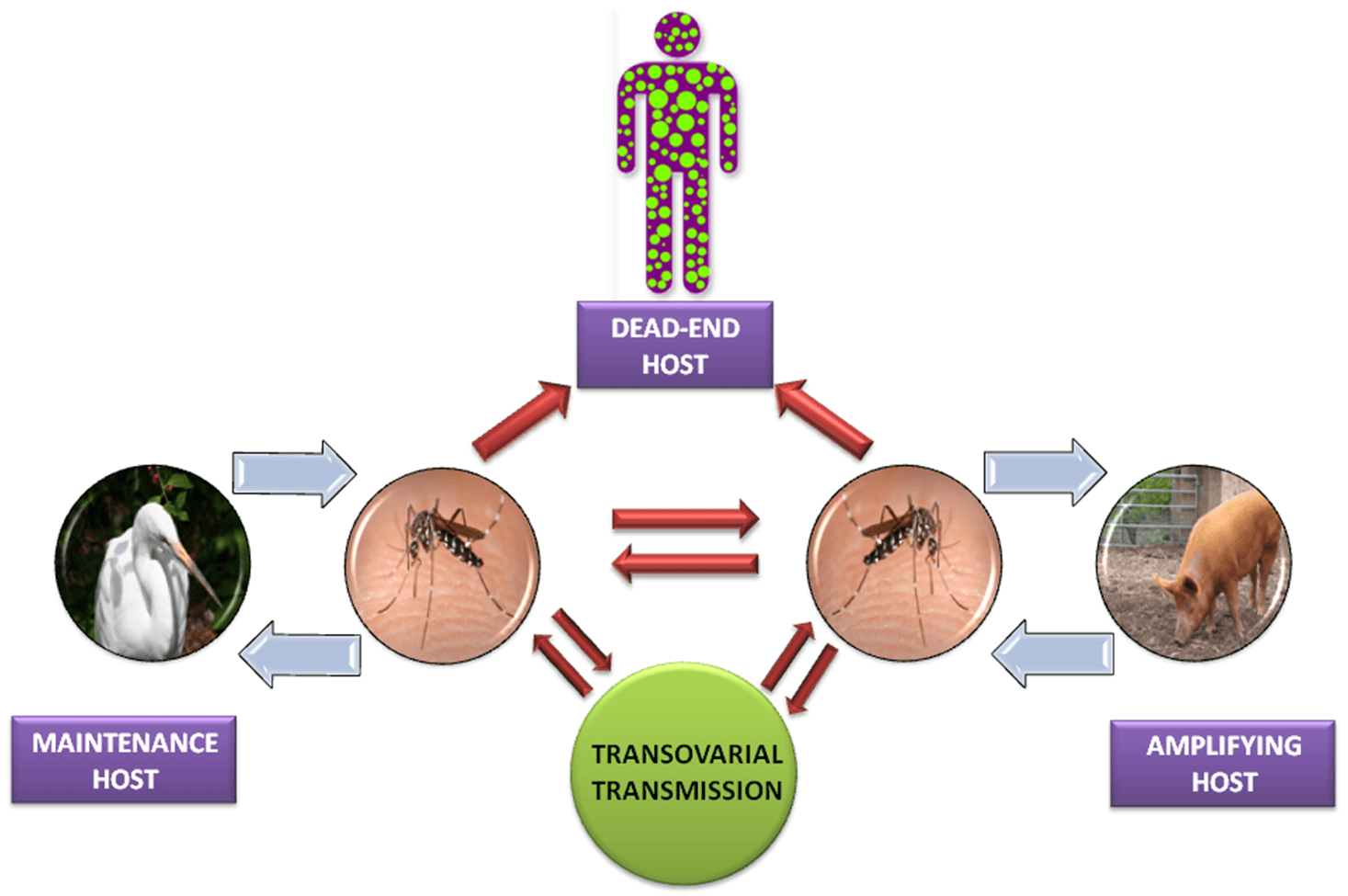 Figure: Fig: Japanese Encephalitis Virus Life Cycle
Figure: Fig: Japanese Encephalitis Virus Life Cycle
Population at risk
- People with weakened immune systems (HIV, taking immunosuppressant drugs)
In endemic countries:
- Primarily affects children, because adults in endemic areas have typically acquired protective immunity through years of repeated subclinical JEV exposure during childhood. Children are immunologically naïve to JEV and lack this accumulated protection.
- Transmission principally occurs in rural agricultural areas or periurban settings often associated with rice farming and pig farming — pigs are key amplifying hosts (see transmission cycle above).
- Transmission is seasonal, and the human disease usually peaks in summer and fall.
- Seasonal transmission varies with monsoon rains and irrigation practices
- Travelers are at increased risk if extensive outdoor or nighttime exposure in rural areas during periods of active transmission.
Pathogenesis of JE Virus Infection
From mosquito bite to bloodstream
When an infected Culex mosquito bites a human, JEV is deposited in the skin. The virus first replicates locally in Langerhans cells (dendritic cells in the skin), which then carry virus to regional lymph nodes. Local lymph node replication amplifies viral load, producing an initial viremia. In most people, the innate immune response and early adaptive immune response contain this viremia before it reaches levels sufficient to cross the blood-brain barrier — this is why over 99% of JEV infections remain subclinical or produce only mild febrile illness.
Crossing the blood-brain barrier
In the minority of infections where viremia is not contained, circulating virus can cross the blood-brain barrier. The exact mechanisms of CNS entry are not fully characterised, but likely involve:
- Direct infection of cerebrovascular endothelial cells allowing virus to enter the parenchyma
- Infection of peripheral neurons (olfactory, cranial nerve endings) with retrograde axonal transport to the CNS
Once inside the CNS, JEV has a particular tropism for neurons — it is directly cytopathic to neuronal cells, causing necrosis and neuroinflammation.
Why the thalamus and basal ganglia?
JEV does not cause diffuse, uniform encephalitis. It preferentially affects the thalamus, basal ganglia, midbrain, pons, and medulla — structures involved in motor coordination, arousal, and autonomic function. This is not fully explained but likely reflects the density of neuronal receptors for viral entry in these deep brain structures. The clinical consequence of this specific neuroanatomical tropism is the Parkinsonian syndrome characteristic of JE: JEV infecting the basal ganglia (the dopaminergic circuit that controls movement coordination) produces tremors, cogwheel rigidity, and masklike facies — the same structures affected in Parkinson's disease, damaged by a completely different mechanism. On MRI, bilateral thalamic lesions are a near-pathognomonic imaging finding for JE and distinguish it from many other causes of encephalitis.
Why children are primarily affected in endemic areas
Adults in JE-endemic regions have typically accumulated protective immunity through repeated subclinical JEV infections during childhood — each asymptomatic exposure builds antibody responses that prevent viremia from reaching levels sufficient for CNS invasion on subsequent exposures. Children in the same regions are immunologically naïve to JEV and have no such protection. This epidemiological pattern is consistent with other neurotropic viruses in endemic areas (poliovirus, VZV) where the burden of clinical disease falls disproportionately on children who haven't yet acquired natural immunity.
Travelers to endemic areas, regardless of age, are in the same immunologically naïve position as children in those areas — which is why JE vaccination is recommended for travelers who will have significant rural or outdoor exposure during transmission season.
Clinical Feature (sign/symptoms)
Most human infections are asymptomatic or result in only mild symptoms. <1% of people infected with JE virus develop clinical disease, out of which 20-30% may die (CFR of 20-30%).
Symptoms start to appear after 5-15 days of the mosquito bite. Common symptoms of JE are;
sudden onset of headache
high fever
vomiting
seizures (common in children)
disorientation
paralysis
tremors and
convulsions and
coma
The classical description of JE includes Parkinsonian syndrome with masklike facies, tremor, cogwheel rigidity, and choreoathetoid movements. 30%–50% of people with encephalitis develop permanent neurologic or psychiatric sequelae.
Laboratory Diagnosis of Japanese Encephalitis
Japanese encephalitis (JE) should be considered in a patient with evidence of a neurologic infection (e.g., meningitis, encephalitis, or acute flaccid paralysis) who has recently traveled to or resided in an endemic country in Asia or the western Pacific. Diagnosis of JE is based on a combination of clinical signs and symptoms and specialized laboratory tests of blood or CSF.
Magnetic resonance imaging (MRI) of the brain can be done to see JE-virus-associated abnormalities in the thalamus (appearance of thalamic lesions), basal ganglia, midbrain, pons, and medulla.
Laboratory diagnosis of JE is generally accomplished by testing serum or cerebrospinal fluid (CSF) to detect virus-specific IgM antibodies.
Sample
CSF and serum
- CSF is drawn by spinal tap (lumbar puncture at the level of L4-L5).
- Should be performed in all suspected patients unless absolutely contraindicated
- Typical CSF picture Nonspecific pleocytosis (leukocytosis) with a predominance of lymphocytes
Slightly elevated protein level (normal-15-50 mg/dl) Normal glucose (40-100 mg/dl) level (meningitis: Low)
Serology
- Detection of IgM antibody against JE virus by IgM capture ELISA in CSF
- Should be performed by using a JE virus–specific IgM-capture ELISA on CSF or serum.
- JE virus–specific IgM can be measured in the CSF of most patients by 4 days after onset of symptoms and in serum by 7 days after onset.
- A ≥4-fold rise in JE virus–specific neutralizing antibodies between acute- and convalescent-phase serum specimens.
- Points to consider in serological tests Interpretation:
Vaccination history Date of onset of symptoms information regarding other flaviviruses known to circulate in the geographic area
Polymerase chain reaction (PCR)
Amplification of JE virus nucleic acid from CSF or brain tissue can be done using PCR methods. Viremia in humans is transient and low level. So virus isolation and nucleic acid amplification tests from blood are insensitive and should not be used for ruling out a diagnosis of JE.
CSF Culture
Limited value in case of viral encephalitis and is not recommended for routine clinical application. Isolation of JE virus in the CSF by co-culturing in phytohemagglutinin P-stimulated peripheral blood mononuclear leukocytes (rarely done).
Treatment of JE Infection
There is no approved specific antiviral drug for Japanese encephalitis. Treatment is entirely supportive and focuses on managing the neurological complications:
- Seizure management: anticonvulsants (benzodiazepines acutely; phenytoin or levetiracetam for ongoing seizure prophylaxis in severe cases)
- Cerebral edema: mannitol or hypertonic saline; elevating the head of the bed; avoiding hypotonic fluids
- Fever management: paracetamol; active cooling in severe hyperthermia
- Secondary infection prevention: nursing care to prevent aspiration pneumonia and pressure sores in comatose patients
- Intensive care: patients with respiratory failure or refractory status epilepticus may require mechanical ventilation
The absence of specific antiviral therapy makes prevention through vaccination the cornerstone of JE control. Early diagnosis and prompt supportive care improve outcomes; the high rates of death and neurological sequelae in JE largely reflect delayed presentation, inadequate intensive care resources, and the intrinsic severity of brainstem/thalamic involvement in severe cases.
JE Vaccine
- Approved for people 2 months of age and older
- Given as a 2-dose series, with the doses spaced 28 days apart.
- Booster dose- may be given to anyone who was vaccinated > one year ago and is still at risk of exposure
- Recommended for: Travelers to Asia (visit rural areas or engage in outdoor activities, visit during peak season)
- Laboratory workers at risk of exposure
How to Remember
The enzootic cycle: pigs amplify, mosquitoes transmit, humans are a dead end. The three-actor cycle is worth anchoring precisely because it's slightly different from dengue's vector-human-vector cycle. Pigs (and wading birds) are the amplifying hosts — they develop high-level viremias that infect feeding mosquitoes. Humans are incidental dead-end hosts who don't develop high enough viremia to infect mosquitoes. The implication: you can't get JE from another person, and culling pigs and vaccinating pigs are legitimate public health tools for reducing human JE burden in endemic areas.
Thalamic lesions on MRI + Parkinsonian features + rural Asia/Pacific exposure = JE until proven otherwise. This combination is the clinical recognition pattern. No other common cause of encephalitis in this region produces bilateral thalamic MRI abnormalities combined with a Parkinsonian movement disorder. Connect the neuroanatomy (basal ganglia and thalamus = motor coordination, arousal circuits) to the clinical presentation, and you won't need to memorise this separately.
CSF IgM is the gold standard, blood PCR is not. Unlike dengue where NS1 and blood PCR are early acute tests, JEV viremia in humans is transient and low-level — the virus is effectively cleared from blood before neurological symptoms appear. By the time a patient presents with encephalitis, blood is the wrong specimen. CSF IgM ELISA is the definitive test. This is the exact opposite of dengue's diagnostic approach and is one of the highest-yield exam distinctions between the two diseases.
JE and dengue share a family — and share a serological problem. Both are Flaviviruses with cross-reactive antibodies. In settings where both co-circulate (Nepal, India, Philippines, most of Southeast Asia — the site's primary audience), a positive dengue IgG can produce a false-positive JE IgG, and vice versa. CSF testing and clinical context are essential to differentiate; serum serology alone in a co-endemic area must be interpreted cautiously. The dengue article covers the flavivirus cross-reactivity issue in more detail.
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Family / Genus | Flaviviridae / Flavivirus (same family as dengue, Zika, West Nile, yellow fever) |
| Genome | ss(+)RNA, ~11 kb; non-segmented |
| Envelope | Present (icosahedral nucleocapsid + lipid envelope with E glycoprotein) |
| Serotypes | One (monotypic — single vaccination confers lifelong protection) |
| Primary vector | Culex tritaeniorhynchus (night-biting); other Culex spp. also involved |
| Amplifying hosts | Domestic pigs and wading birds (develop high viremia, infect mosquitoes) |
| Human host type | Incidental dead-end host (viremia too low to infect feeding mosquitoes) |
| Transmission season | Peak: August–October (monsoon, rice-farming, mosquito breeding season) |
| % infections causing clinical disease | <1% |
| Case fatality rate (clinical disease) | 20–30% |
| Neurological sequelae in survivors | 30–50% |
| Age group primarily affected in endemic areas | Children (adults have acquired immunity from subclinical childhood exposure) |
| Classic clinical triad | Fever + altered consciousness + movement disorder (Parkinsonian features) |
| CNS tropism | Thalamus, basal ganglia, midbrain, pons, medulla |
| Characteristic MRI finding | Bilateral thalamic lesions |
| CSF picture | Lymphocytic pleocytosis, slightly elevated protein, normal glucose |
| Gold standard diagnostic test | IgM capture ELISA on CSF |
| Blood PCR utility | Low — viremia is transient and low-level by the time symptoms appear |
| Treatment | Supportive only (no specific antiviral) |
| Vaccine | Approved from 2 months of age; 2-dose series, 28 days apart |
Where Students Get Confused
"JEV viremia in humans is like dengue — blood tests should be used for early diagnosis." They're different. In dengue, blood PCR and NS1 antigen are the early acute tests because dengue produces significant viremia during the febrile phase. JEV produces a transient, low-level viremia in humans that is typically undetectable by the time neurological symptoms appear. The virus has already reached the CNS by then. Blood is the wrong specimen for JE diagnosis; CSF is the right specimen.
"JE encephalitis is diffuse, like most viral encephalitides." JEV has specific tropism for the thalamus, basal ganglia, and brainstem — not diffuse cortex. This is why JE produces movement disorders (Parkinsonian features) rather than primarily cortical symptoms (aphasia, focal weakness). The bilateral thalamic MRI lesions are near-pathognomonic and should be actively sought in any patient presenting with encephalitis in an endemic area.
"A positive dengue IgG test in a patient with encephalitis confirms dengue encephalitis, not JE." In regions where dengue and JE co-circulate, cross-reactive flavivirus antibodies mean that dengue IgG serology cannot exclude JE and vice versa. A febrile patient from Nepal or the Philippines with encephalitis and positive dengue IgG needs CSF testing for JE IgM before dengue encephalitis is accepted as the diagnosis. Clinical picture (Parkinsonian features, thalamic MRI changes, rural/agricultural exposure during mosquito season) should drive test selection.
"Adults in endemic areas are equally at risk as children." They are not. Adults in JE-endemic areas have largely acquired protective immunity from years of subclinical JEV exposure during childhood. The clinical disease burden falls predominantly on children under 15 who haven't yet accumulated this immunity. Travelers of any age lack this acquired immunity and are at similar risk to endemic-area children.
References
- Ghosh, D., & Basu, A. (2009). Japanese encephalitis — a pathological and clinical perspective. PLoS Neglected Tropical Diseases, 3(9), e437. https://doi.org/10.1371/journal.pntd.0000437
- Yun, S. I., & Lee, Y. M. (2014). Japanese encephalitis: the virus and vaccines. Human Vaccines & Immunotherapeutics, 10(2), 263–279. https://doi.org/10.4161/hv.26902
- Campbell, G. L., Hills, S. L., Fischer, M., Jacobson, J. A., Hoke, C. H., Hombach, J. M., Marfin, A. A., Solomon, T., Tsai, T. F., Tsu, V. D., & Ginsburg, A. S. (2011). Estimated global incidence of Japanese encephalitis: a systematic review. Bulletin of the World Health Organization, 89(10), 766–774. https://doi.org/10.2471/BLT.10.085233
Frequently Asked Questions
Why are children more affected by Japanese encephalitis than adults in endemic countries?
Why is blood PCR not useful for diagnosing JE, when it is useful for dengue?
What makes bilateral thalamic lesions on MRI significant in a patient with encephalitis?
Why can JE serology cross-react with dengue tests?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.