Francisella tularensis: Properties, Pathogenesis, Lab Diagnosis
Francisella tularensis: Properties, Pathogenesis, Lab Diagnosis
Francisella tularensis causes life-threatening infections in animals (rabbits, hares, and rodents) and people (zoonotic disease). It is also known as ‘Rabbit Fever’ or ‘Deer Fly fever.’
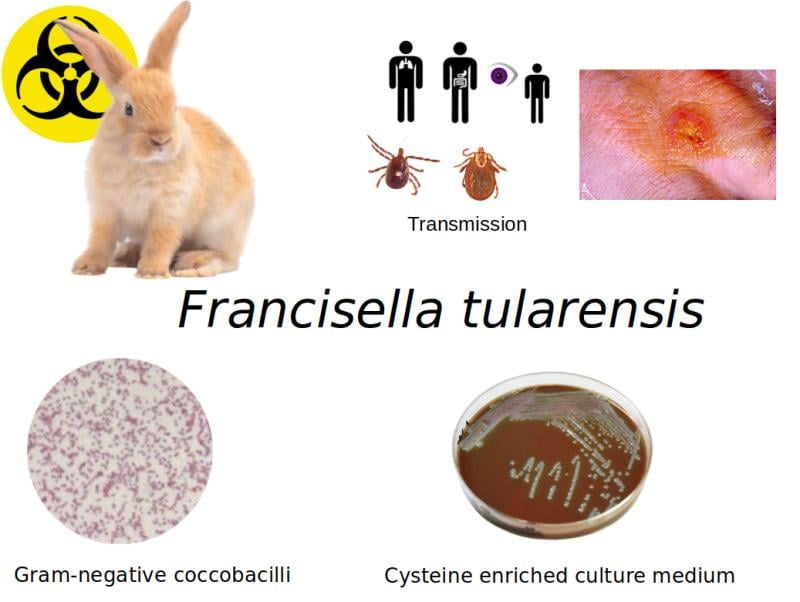 Figure: Francisella tularensis basic feature
Figure: Francisella tularensis basic feature
Properties ofFrancisella tularensis
- Causes highly infectious (as few as 10 organisms can cause disease and the organism can enter the human body through skin, eyes, mouth, or lungs) but treatable (can be treated successfully with antibiotics).
- Agent of bioterrorism: Because of its highly infectious nature F. tularensis is currently classified as a category A agent of bioterrorism.
- Bacterial culture of tularemia should be carried out in a biosafety level 3 (BSL3) laboratory.
- Gram-negative coccobacillus
- Non-motile
- Non-spore forming
- Facultative intracellular bacteria
- Aerobic
- Fastidious bacteria (requires cysteine enriched medium for growth)—Cysteine enriched chocolate agar, BCYE agar, and CHAB agar (cysteine heart agar with blood).
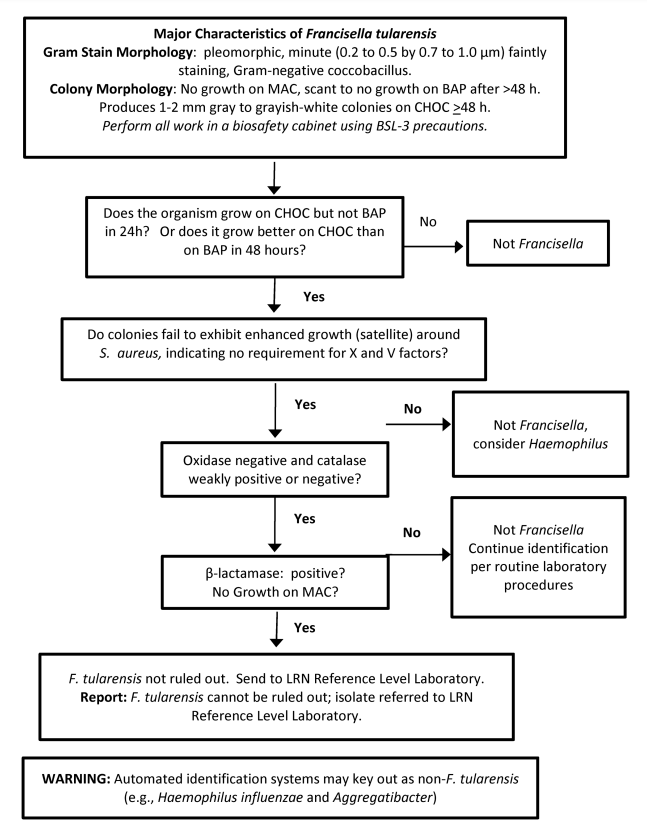 Figure: Francisella tularensis identification flow chart Image source: Laboratory Response Network (LRN)
Figure: Francisella tularensis identification flow chart Image source: Laboratory Response Network (LRN)
Pathogenesis
Mode of Transmission
Source: It persists in contaminated environments, insects, and animal carries.

 ### Transmission routes
### Transmission routes
- Bite of blood-sucking insects such as tick and deer fly
- Skin contact with infected animals
- Ingestion of contaminated water
- Inhalation of contaminated aerosols or agricultural and landscaping dust
- Laboratory exposure: In the cases of unanticipated events, laboratory workers may get exposed and acquire infection with F. tularensis while subculturing positive broth blood cultures, performing Gram’s staining, or examining agar plates
Prevalence
F. tularensis has four subspecies: tularensis, holarctica, novicida, and mediasiatica. The first three species are found in North America whereas subspecies mediasiatica is found in central Asia. Subspecies tularensis is the most common and the most virulent among all. It has been isolated only from North America, which accounts for more than 70% of cases.
Increasing number of cases due to other subspecies have been reported from the Scandinavian countries, Eastern Europe and Siberia.
Virulence Factors
Once F. tularensis is engulfed by immune cells (macrophages) that routinely kill bacteria, it replicates and evades parts of the immune system using an array of virulence factors:
 - Capsule (anti-phagocytic in nature)
- Capsule (anti-phagocytic in nature)
- The outer membrane (LPS layer) helps to thwart innate immune response as it evades recognition by Toll-Like receptors (TLR)
- Type IV Pili (adherence)
- Acid phosphatase: Prevents the fusion of phagosome with the lysosome.
- Siderophores: acquisition of iron
Clinical Manifestations
Tularemia symptoms usually appear within 3-5 days of infection, but may also appear up to 15 days later. Tularemia is characterized by various clinical syndromes depending on how the person was infected.
Main forms of the disease are:
Ulceroglandular tularemia
It is the most common form, (75-85% of total cases), characterized by an ulcerative lesion at the site of inoculation, with regional lymphadenopathy (armpit or groin.)
Glandular tularemia
It presents with swollen lymph nodes (without ulcer)
Pulmonary tularemia
- It can result from aerosol inhalation (laboratory workers) or can spread to the lungs following bacteremia if other forms of tularemia are left untreated.
- Symptoms include cough, chest pain, and difficulty breathing.
- Most serious forms of tularemia
Oropharyngeal tularemia
It occurs following the ingestion of contaminated undercooked meat. It is characterized by membranous pharyngitis with cervical lymphadenopathy.
Oculo-glandular tularemia
This form occurs when the bacteria enter through the eye. It is characterized by purulent conjunctivitis with preauricular lymphadenopathy.
Typhoid-like illness
It presents with the standard, nonspecific febrile (fever) symptoms, but without a known route of infection (via the skin, eye, ingestion, or inhalation)
Laboratory Diagnosis
Difficult to diagnose because it’s a rare disease with nonspecific signs and symptoms. Diagnosis may rely on epidemiologic evidence (e.g., history of mowing the lawn in an endemic area)
Specimen
Ulcer scrapings, lymph node biopsy, gastric washings, sputum, and blood.
Culture
Isolation is very difficult as F. tularensis is highly fastidious
It needs special media such as:
- BCG agar (blood cysteine glucose agar)
- CHAB agar (cysteine heart agar supplemented with 9% heated sheep blood).
 Figure: F. tularensis in cysteine enriched chocolate agar
Figure: F. tularensis in cysteine enriched chocolate agar
Specimens are inoculated onto the media and incubated at 37oC for 2-4 days aerobically as F. tularensis is an obligate aerobe.
Colonies are blue-gray, round, smooth, and slightly mucoid with small zone of alpha-hemolysis.
Safety precautions such as biosafety level III must be used to handle clinical specimens to avoid the risk of laboratory-acquired infections.
Identification
- F. turalensis is a small gram-negative coccobacillus with bipolar appearance, non-motile and capsulated.
- It is weakly catalase positive, oxidase negative and H2S positive
- It produces acid but no gas from glucose, maltose and mannose.
- Direct fluorescent antibody tests can be done with commercially available antisera, directly from the culture colonies for subsequent identification.
Antibody detection
It is the mainstay of diagnosis as isolation is difficult. Agglutination test (latex and tube agglutination) and ELISA formats are available.
Molecular Diagnosis
PCR assay has been used to detect F. tularensis specific genes encoding the outer-membrane proteins. It can also differentiate subspecies.
Prevention & Treatment
Steps to prevent tularemia include:
- Using insect repellent
- Wearing gloves when handling sick or dead animals
- Avoiding mowing over dead animals
Treatment
Streptomycin, gentamicin, doxycycline, and ciprofloxacin are used to treat tularemia. Treatment usually lasts 10 to 21 days depending on the stage of illness and the medication used.
References
- Madigan Michael T, Bender, Kelly S, Buckley, Daniel H, Sattley, W. Matthew, & Stahl, David A. (2018). Brock Biology of Microorganisms (15th Edition). Pearson.
- Color Atlas and Textbook of Diagnostic Microbiology, Koneman, 5th edition

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.