Listeria monocytogenes: Properties, Virulence Factors, Pathogenesis, and Lab Diagnosis
Listeria monocytogenes is a psychrotolerant, facultative intracellular food-borne pathogen. Learn its cold enrichment, differential motility, virulence factors (InlA/B, listeriolysin O, ActA actin tails), intracellular lifecycle, three-barrier crossing, listeriosis clinical syndromes, lab diagnosis (CAMP test, culture), and ampicillin treatment.
In 2011, a listeriosis outbreak linked to whole cantaloupes from a Colorado farm killed 33 people and hospitalised 147 across 28 US states — the deadliest foodborne illness outbreak in the United States in nearly 90 years. The contamination occurred during post-harvest handling and packing; the cantaloupes were not cooked before consumption. Many victims were elderly, immunocompromised, or pregnant.
Listeria monocytogenes is responsible for one of the most clinically severe foodborne diseases despite relatively low incidence. While Salmonella and Campylobacter infect millions annually, listeriosis is far rarer — but its case fatality rate is approximately 20–30%, compared to less than 1% for most other foodborne pathogens. This lethality reflects two biological features that make L. monocytogenes uniquely dangerous:
- It grows in the refrigerator at 4°C — the temperature most people assume eliminates bacterial risk in stored food.
- It lives inside host cells, protected from antibodies, complement, and many antibiotics — making it disproportionately dangerous in people with impaired cell-mediated immunity.
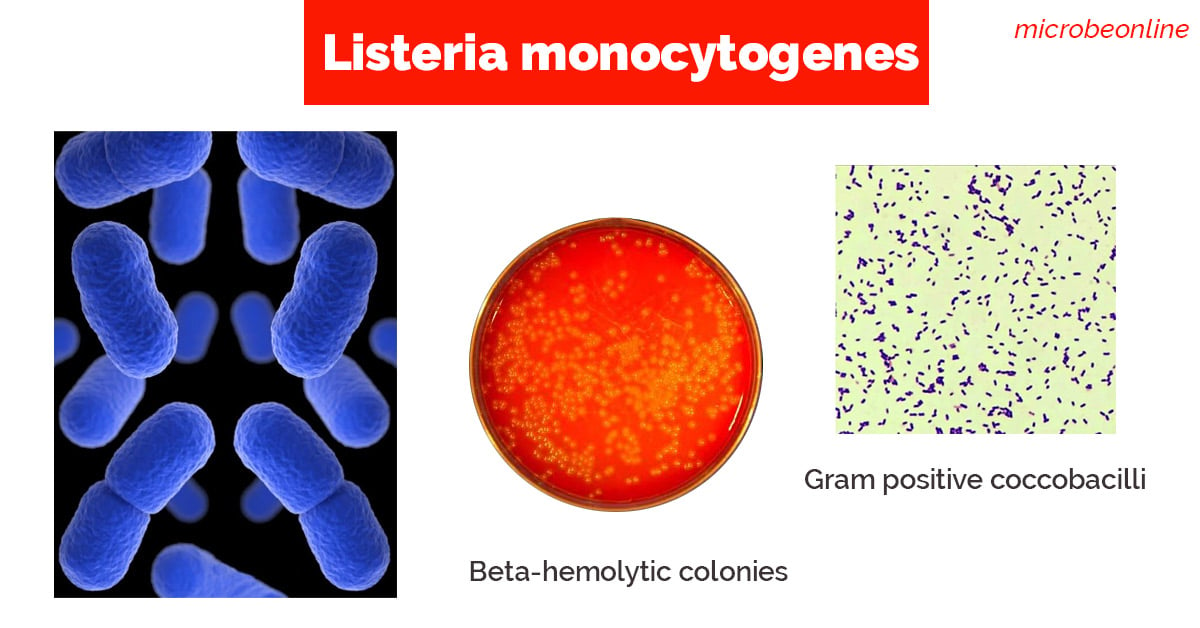 Figure: Listeria monocytogenes in Gram staining and Culture
Figure: Listeria monocytogenes in Gram staining and Culture
General Properties
Listeria monocytogenes is a facultative intracellular, Gram-positive coccobacillus with several distinctive properties that set it apart from other food-borne pathogens:
- It shows tumbling type of motility at 25°C but non-motile at 37°C (called differential motility, which is due to the temperature-dependent flagella expression).
- Unlike most other harmful bacteria, L. monocytogenes grow slowly on foods stored in a refrigerator (4°C). It is commonly found in stored foods especially aged soft cheeses, packaged meats, milk, and cold salads.
- Growth improves if the specimen is refrigerated at 4°C and cultured at frequent intervals, this procedure is called cold enrichment.
- It shows a positive CAMP test when streaked at a right angle to beta-hemolytic Staphylococcus aureus(enhanced arrowhead hemolysis).
- Beta-haemolytic on blood agar — narrow zone of hemolysis; this is the key visual identification feature that distinguishes L. monocytogenes from non-pathogenic Listeria species and from similar-appearing organisms like Enterococcus
- Catalase-positive, oxidase-negative — distinguishes from streptococci (catalase-negative) and Gram-positive rods
- Temperature range: 1–45°C; grows at refrigerator temperatures (psychrotolerant); optimal 30–37°C
- Salt tolerance: Grows in up to 10% NaCl — relevant to growth in processed meats and cheeses
High-risk foods for Listeria contamination:
| Food category | Examples | Risk note |
|---|---|---|
| Soft cheeses | Brie, Camembert, feta, queso fresco | Unpasteurised or post-pasteurisation contamination; not cooked before consumption |
| Ready-to-eat deli meats | Sliced ham, salami, hot dogs | Processing equipment contamination; may not be reheated |
| Smoked fish | Smoked salmon, gravlax | Cold-smoked; not fully cooked |
| Raw sprouts | Alfalfa, bean sprouts | Soil contamination; not cooked |
| Refrigerated paté | Liver paté, meat spreads | Long refrigerator shelf life allows multiplication |
Epidemiology and High-Risk Groups
L. monocytogenes is ubiquitous in the environment — found in soil, water, vegetation, animal feces, and silage. Human infection occurs almost exclusively through ingestion of contaminated food. Unlike most foodborne pathogens:
- Incubation period is long — 1–70 days (median ~21 days); patients may not connect illness to a specific meal
- Infectious dose is uncertain — immunocompromised individuals may be infected by much lower doses than healthy adults
- Small proportion of infections become invasive — most healthy adults clear the organism at the gut level; invasive disease requiring hospitalisation occurs almost exclusively in the high-risk groups below
High-risk groups:
| Group | Risk and mechanism | Clinical manifestation |
|---|---|---|
| Pregnant women | T-cell immunity naturally suppressed during pregnancy | Usually mild flu-like illness in mother; severe fetal disease — premature labour, stillbirth, neonatal sepsis, neonatal meningitis |
| Neonates | Immature immune system; maternal–fetal transmission | Early-onset (≤7 days): septicaemia, granulomatosis infantiseptica; late-onset (>7 days): meningitis |
| Elderly (>65 years) | Declining cell-mediated immunity | Bacteraemia, meningitis, meningoencephalitis |
| Immunocompromised | HIV/AIDS, transplant, chemotherapy, corticosteroids | Bacteraemia; CNS disease; mortality up to 30% |
| Healthy adults | Rarely invasive; high-dose exposure | Febrile gastroenteritis (self-limiting); no invasive disease |
The immune system clue: The pattern of who gets invasive listeriosis (pregnant, neonates, elderly, immunosuppressed) points directly to the pathogenesis: L. monocytogenes depends on cell-mediated immunity for clearance. Anyone whose cell-mediated immunity is compromised is vulnerable. This is why listeriosis is considered an AIDS-defining illness and why transplant recipients are warned about soft cheeses.
Transmission
Listeria monocytogenes can be found in a variety of dairy products, vegetables, fish, and meat products. Unlike most other harmful bacteria, it can grow on foods stored in a refrigerator. Consumption of food contaminated with Listeria monocytogenes is the primary mode of transmission of listeriosis. Listerosis can also be transmitted from mother to fetus if infection occurs during pregnancy.
AsL. monocytogenes is able to cross the placenta, listeriosis is a major cause of perinatal and neonatal disease, typically resulting in abortion.
Pathogenesis: The Intracellular Lifecycle
The pathogenesis of listeriosis is defined by the organism's extraordinary ability to invade non-phagocytic cells, escape the phagosome, replicate in the cytoplasm, and spread directly to adjacent cells — all without ever being exposed to the extracellular immune environment.
The lifecycle in six steps:
1. INTERNALISATION (InlA/InlB)
L. monocytogenes attaches to E-cadherin (via InlA) and Met receptor (via InlB)
on intestinal epithelial cells → bacteria are engulfed into a membrane vacuole
↓
2. PHAGOSOME ESCAPE (Listeriolysin O + Phospholipases)
LLO creates pores in the vacuolar membrane
PlcA and PlcB digest the membrane → bacteria escape into the cytoplasm
(before lysosomal fusion — bacterium avoids intracellular killing)
↓
3. INTRACELLULAR REPLICATION
Bacteria multiply freely in the nutrient-rich cytoplasm
PrfA (master regulator) coordinates virulence gene expression
↓
4. ACTIN TAIL FORMATION (ActA)
ActA on bacterial surface nucleates host actin filaments
Rocket-like F-actin tails form → bacteria propelled at 11 μm/minute
↓
5. CELL-TO-CELL SPREAD
Bacteria propelled to cell surface → protrusion into adjacent cell
Engulfed in double-membrane vacuole in new cell
↓
6. DOUBLE VACUOLE ESCAPE (LLO + PlcB again)
Same mechanism — LLO and PlcB lyse double membrane → new cycle begins
Why this lifecycle is clinically unique: At no point in steps 3–6 does L. monocytogenes re-enter the extracellular environment. It spreads from cell to cell entirely within host cells — protected from:
- Antibodies (cannot reach intracellular bacteria)
- Complement (same)
- Many antibiotics (poor intracellular penetration)
This is why cell-mediated immunity (CD8+ T cells and NK cells) is the primary defence against Listeria, not antibody-mediated immunity. Immunosuppression of cell-mediated immunity (pregnancy, steroids, AIDS, transplant) = vulnerability.
Virulence Factors
PrfA — The Master Regulator
All L. monocytogenes virulence genes are co-regulated by PrfA (Positive Regulatory Factor A), a transcriptional activator encoded within LIPI-1 (Listeria Pathogenicity Island 1):
- Activates expression of hly (LLO), actA, plcA, plcB, inlA, inlB, and other virulence genes
- Expression is temperature-regulated — upregulated at 37°C (host temperature), low at environmental temperatures
- Mutations in prfA abolish virulence — strains without functional PrfA cannot cause disease
- PrfA is the single most important target for understanding Listeria virulence gene regulation
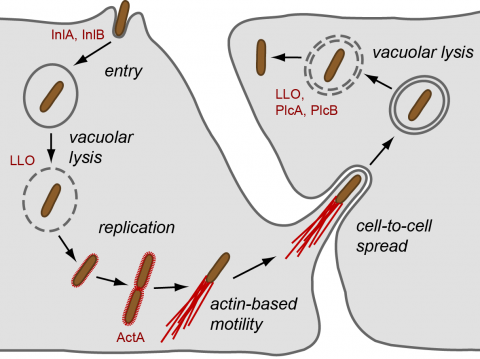 Figure: Listeria cell cycle (Image source:Pasteur Institute)
Figure: Listeria cell cycle (Image source:Pasteur Institute)
Internalin A and B (InlA and InlB) — Invasion Proteins
Internalin A (InlA):
- Surface protein; binds E-cadherin on intestinal epithelial cells
- Mediates entry across the intestinal epithelium — the first barrier crossing
- Also mediates placental invasion — E-cadherin is expressed on syncytiotrophoblasts; explains maternal-fetal transmission
- Species specificity: InlA binds human and guinea pig E-cadherin but NOT murine E-cadherin — explains why standard mouse models underestimate listeriosis risk
Internalin B (InlB):
- Binds Met receptor (hepatocyte growth factor receptor) and complement component C1q receptor
- Mediates entry into hepatocytes and other cell types not expressing E-cadherin
- Contributes to hepatic invasion and haematogenous spread
Listeriolysin O (LLO) — The Phagosome Escape Factor
LLO is a cholesterol-dependent cytolysin (CDC) — the same family as streptolysin O (S. pyogenes), pneumolysin (S. pneumoniae), and perfringolysin (C. perfringens):
- Creates pores in the phagosomal membrane at low pH → bacteria escape to cytoplasm before lysosomal fusion
- pH-dependent activation (active at pH 5–6 of phagosome; less active at neutral cytoplasmic pH) — prevents bacterial self-destruction in cytoplasm
- Beta-hemolysis on blood agar is the laboratory manifestation of LLO activity — the narrow hemolysis zone around colonies is diagnostic
- LLO is also active in the double-membrane vacuole during cell-to-cell spread (with PlcB)
Actin Assembly-Inducing Protein (ActA) — The Motility Engine
ActA is the uniquely Listeria-specific virulence factor that enables intracellular motility:
- Surface protein expressed on the bacterial pole
- Nucleates host actin monomers via the Arp2/3 complex — same mechanism as cell migration
- Produces rocket-like F-actin tails propelling bacteria at up to 11 µm/minute
- Enables bacteria to be propelled through the cytoplasm and into adjacent cells — direct cell-to-cell spread with no extracellular exposure
 Figure: Actin filament and intracellular spread of Listeria monocytogenes.
Figure: Actin filament and intracellular spread of Listeria monocytogenes.
Phospholipases C (PlcA and PlcB)
Two distinct phospholipases act sequentially in phagosome escape:
- PlcA (PI-PLC): Phosphatidylinositol-specific; cleaves GPI-anchored proteins on phagosomal membrane; acts early in single-membrane phagosome escape
- PlcB (PC-PLC): Broad-range; essential for escaping the double-membrane vacuole during cell-to-cell spread; acts with LLO in the second escape step
Virulence Factor Summary
| Factor | Function | Barrier/Step |
|---|---|---|
| PrfA | Master regulator of all virulence genes | Controls everything |
| InlA | Binds E-cadherin → intestinal epithelial entry; placental crossing | Intestinal + placental barriers |
| InlB | Binds Met/C1q → hepatocyte and diverse cell entry | Hepatic invasion |
| LLO | Pore formation → single-membrane phagosome escape; double-membrane escape | Step 2 + Step 6 |
| ActA | Actin tail formation → intracellular motility; cell-to-cell spread | Steps 4–5 |
| PlcA | PI-specific membrane cleavage; early phagosome disruption | Step 2 |
| PlcB | Broad-range; double-membrane vacuole disruption | Step 6 |
Three Barriers: Why Listeria Reaches the Brain and Placenta
L. monocytogenes can cross three host tissue barriers that most bacteria cannot:
| Barrier | Mechanism | Clinical consequence |
|---|---|---|
| Intestinal epithelium | InlA binds E-cadherin on enterocytes; transcytosis | Systemic bacteraemia |
| Blood-brain barrier | InlA + InlB enable crossing of brain capillary endothelium; "Trojan horse" in monocytes | Meningitis, meningoencephalitis, brain abscess |
| Placenta (fetoplacental barrier) | InlA binds E-cadherin on syncytiotrophoblasts | Fetal infection: abortion, stillbirth, neonatal sepsis |
The "Trojan horse" mechanism: L. monocytogenes also uses infected circulating monocytes and macrophages as vehicles to cross the blood-brain and placental barriers — the bacteria are transported inside the immune cells that were supposed to destroy them.
Diseases
Listeriosis is one of the most serious foodborne diseases. Clinical manifestation of listerosis depends on the age of the patient and other underlying conditions such as pregnancy, immunosuppression, etc.
Depending on the immune status of the person and the part of the body affected, listeriosis can cause variety of symptoms ranging from milder flu-like illness to convulsion and death.
- Pregnant women: It affects both the mother and the fetus. Mother mostly experiences mild illness (flu-like symptoms) but it causes severe disease in the fetus or newborn baby (such as abortion, preterm delivery, newborn death, and neonatal meningitis).
- People other than pregnant women: Fever, muscle aches, headache, stiff neck, confusion, loss of balance, and convulsions.
Most people with invasive listeriosis require hospital care, and about one in five people with the infection die.
Laboratory Diagnosis
Sample: CSF, blood, feces or placental tissue or any other tissue specimens depending on the suspected disease and/or clinical presentation.
**Direct wet mount:**Listeria monocytogenes exhibits characteristic end-over-end tumbling motility when incubated in nutrient broth at room temperature for 1 to 2 hours. Presumptive identification of L. monocytogenes can be done by observation of such motility by direct wet mount.
Alternatively, suspected colonies of L. monocytogenes can be stabbed into a tube of semisolid agar and incubated at 25°C for 18 hours. Characteristics umbrella-shaped motility pattern is seen after overnight incubation.
Gram staining: Regular, short, gram-positive rods or coccobacilli occurring in pairs (resembles streptococci).
Cold enrichment
Cold enrichment is done for the isolation of Listeria monocytogenes from the placenta, tissues as well as specimens from heavily contaminated sources such as feces. The specimen is inoculated into a nutrient broth or trypticase soy broth and incubated at 4°C for one month and subcultured weekly.
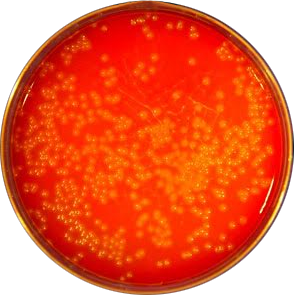 Figure: Beta-hemolytic colonies of L. monocytogenes
Figure: Beta-hemolytic colonies of L. monocytogenes
Culture: Listeria monocytogenes can be cultured on conventional media incorporating sheep, horse or rabbit blood. Listeria monocytogenes produces round, smooth, translucent colonies with a narrow zone of beta-hemolysis. Colonies are small and give blue-green color under reflective light.
Other characteristics that helps in the identification of this bacteria are:
- Catalase positive
- Voges-Proskauer-positive
- Esculin positive: L. monocytogenes is able to hydrolyze esculin in the presence of 40% bile. Esculin hydrolysis is indicated by the blackening of the medium.
- CAMP test positive
- L. monocytogenes shows a shovel-shaped (arrowhead) enhancement of beta-hemolysis when streaked perpendicular to a Staphylococcus aureus streak — the hemolysis narrows toward the Staph streak (arrowhead shape). This is the positive CAMP test for Listeria.
- By contrast, Streptococcus agalactiae (GBS) shows a bow-tie (rectangular) enhancement of hemolysis in the CAMP test. The different shape of hemolysis enhancement distinguishes the two organisms.
Molecular diagnosis
Detection of Listeria monocytogenes DNA in CSF and tissue (fresh or paraffin blocks)
Commercial methods
- AccuPROBE Listeria monocytogenes Culture Identification kit: Rapid DNA probe test, which utilizes the technique of nucleic acid hybridization for the identification of Listeria monocytogenes isolated from culture.
- Matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) method
- GeneQuence for Listeria monocytogenes
Treatment
L. monocytogenes is intrinsically resistant to all cephalosporins — an important clinical point because cephalosporins are often used empirically for bacterial meningitis before the causative organism is known.
Drug of choice: Ampicillin (or amoxicillin)
- L. monocytogenes is consistently susceptible to ampicillin
- For severe invasive disease (meningitis, bacteraemia): Ampicillin + gentamicin (synergistic combination; gentamicin achieves intracellular activity)
- For penicillin-allergic patients: Trimethoprim-sulfamethoxazole (co-trimoxazole) — alternative for invasive listeriosis
- Duration: 2–3 weeks for bacteraemia; 3–6 weeks for CNS involvement
Empirical meningitis treatment — critical point: Standard empirical bacterial meningitis treatment (third-generation cephalosporin ± dexamethasone) does NOT cover Listeria. In patients at risk for listeriosis (elderly, immunocompromised, pregnant), ampicillin must be added to empirical meningitis treatment. Failure to add ampicillin when treating a high-risk patient with bacterial meningitis is a potentially fatal omission.
No vaccine available. Prevention relies entirely on food safety — avoiding high-risk foods in high-risk groups, adequate cooking, and proper refrigerator hygiene.
How to Remember
Listeria is defined by two unique properties — remember both:
- Grows at 4°C (the refrigerator temperature) → infects refrigerated ready-to-eat food
- Intracellular lifecycle → cell-mediated immunity is the only defence → dangerous in pregnancy, immunosuppression, elderly
The intracellular lifecycle as a logical chain: InlA/B (get in) → LLO + PlcA (escape phagosome) → ActA (make actin rocket) → spread to next cell → LLO + PlcB (escape double membrane) → repeat
Every step has a named virulence factor. Each step explains the next.
The CAMP test shape distinction: Listeria CAMP = Arrowhead (narrows toward Staph streak) GBS CAMP = Bow-tie (broadens toward Staph streak) Think: Listeria = Lance (pointed arrowhead)
The antibiotic trap — cephalosporins do NOT work: Empirical meningitis treatment with cephalosporins misses Listeria. High-risk patient + meningitis + empirical treatment = always ADD ampicillin. This is one of the most tested clinical pharmacology points about Listeria.
The differential motility trick: 25°C: motile (tumbling) — flagella expressed 37°C: non-motile — flagella suppressed The motility test is run at 25°C (room temperature), not 37°C (incubator temperature). Testing at the wrong temperature gives a false non-motile result.
Three barriers, three outcomes: Intestinal barrier → bacteraemia Blood-brain barrier → meningitis/encephalitis Placental barrier → fetal death / neonatal sepsis
References and further readings
- Procop, G. W., & Koneman, E. W. (2016). Koneman’s Color Atlas and Textbook of Diagnostic Microbiology(Seventh, International edition). Lippincott Williams and Wilkins.
- Tille, P. (2017). Bailey & Scott’s Diagnostic Microbiology(14 edition). Mosby.
- Listeria (Listeriosis)| Listeria | CDC. https://www.cdc.gov/listeria/
- Smith GA et al. (1995). The two distinct phospholipases C of L. monocytogenes have overlapping roles in escape from a vacuole and cell-to-cell spread. Infection and Immunity, 63(11), 4231.
- Wei Z et al. (2005). L. monocytogenes phosphatidylinositol-specific phospholipase C has evolved for virulence. PNAS, 102(36), 12927. doi:10.1073/pnas.0501725102
- Swaminathan B & Gerner-Smidt P. (2007). The epidemiology of human listeriosis. Microbes and Infection, 9(10), 1236–1243. https://doi.org/10.1016/j.micinf.2007.05.011 7. Cossart P. (2011). Illuminating the landscape of host-pathogen interactions with the bacterium Listeria monocytogenes. PNAS, 108(49), 19484–19491. https://doi.org/10.1073/pnas.1112371108

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.