Toxoplasma gondii: Life Cycle, Reactivation in AIDS, Congenital Infection, and Diagnosis
Why bradyzoite cysts hide in the brain for decades, why AIDS patients develop ring-enhancing lesions, and when maternal IgG actually protects the fetus.
A 34-year-old man with known HIV infection presents with two weeks of progressive headache, confusion, and right-sided weakness. His CD4 count is 68 cells/μL. CT brain shows multiple ring-enhancing lesions with surrounding oedema in the basal ganglia and cerebral cortex. The radiologist's differential: toxoplasmic encephalitis versus CNS lymphoma.
This presentation accounts for the majority of space-occupying brain lesions in advanced HIV disease in resource-limited settings and the reason the first-line treatment approach is to simply treat empirically for Toxoplasma and watch for response, rather than immediately proceeding to brain biopsy. The underlying biology that explains both the clinical presentation and the empirical treatment strategy is a single, remarkable property of T. gondii: the parasite can form dormant tissue cysts in the brain that persist for the lifetime of the host, completely silently, held in check only by the CD4+ T-cell immune response. When that response collapses as it does in AIDS below a CD4 count of approximately 100; the cysts rupture, tachyzoites emerge, and the resulting focal inflammation and necrosis produces exactly the ring-enhancing lesion seen above.
Understanding this one mechanism makes the rest of Toxoplasma biology coherent: why cats are the only definitive hosts, why 30–50% of the global population is chronically but silently infected, why pregnant women are warned about cat litter and undercooked meat, and why treatment is lifelong in AIDS patients rather than a time-limited course. The life cycle, clinical presentations, and diagnostic approach all follow from this central biology.
Toxoplasma gondii is a protozoan parasite of many vertebrates including humans and causes the disease Toxoplasmosis. Its name was derived from the crescent shape of the tachyzoite stage of the parasite (taxon- ‘bow’; plasma- ‘form’). The parasite was first discovered in 1908, by Charles Nicolle and Louis Manceaux at the Pasteur Institute, in the North African rodent called the gundi, hence the species name gondii.
If a pregnant mother has a history of stillbirth or miscarriage she might be tested with ‘TORCH’ panel test. TORCH is an acronym representing congenital infections caused by Toxoplasma gondii, other agents, rubella, cytomegalovirus (CMV), and herpes simplex virus (HSV).
Properties
- Obligate Intracellular parasite; reticuloendothelial cells.
- Worldwide in distribution; serologic evidence suggests more than 70% of all individuals are exposed to this pathogen but the disease itself is relatively rare.
- Most infections are benign and asymptomatic.
- Toxoplasma gondii completes its lifecycle into two hosts.
- Definitive hosts: members of family felidae (domestic cats and their relatives). The most common primary host of Toxoplasma is the cat.
- Intermediate hosts: Humans are the intermediate host. Other intermediate hosts are birds, rodents, pigs, cattle, etc.
Source of infection
 Humans can become infected with Toxoplasma gondii via any of several routes:
Humans can become infected with Toxoplasma gondii via any of several routes:
- Ingestion of oocyst (containing sporozoites). This happens when a person consumes food or water contaminated with cat feces, for example while changing the litter box of a pet cat).
- Ingestion of undercooked meat of animals harboring tissue cysts (containing bradyzoites)
- Tachyzoites stage of this parasite can be transferred from infected person to susceptible person during blood transfusion or organ transplantation. Though rare, this is another possibility.
- Tachyzoites stage of this parasite can also transmit transplacentally from mother to fetus.
Morphological Forms
Toxoplasma gondii exists in three forms. All of these stages are infectious.
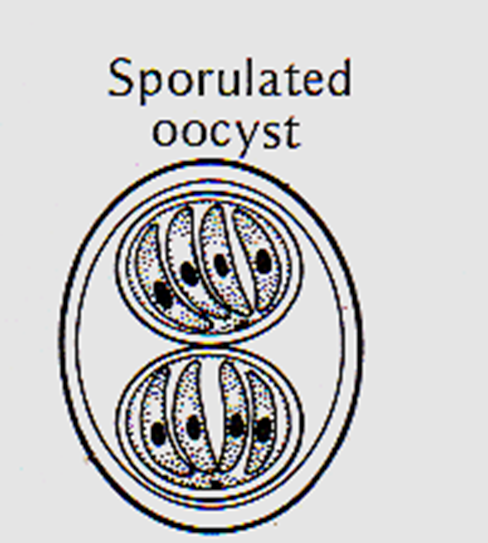
Oocyst
- Present in cat and other felines and not in humans.
- Formed by sexual reproduction.
- Oocyst shed in cat feces (contains two sporocyst, each containing 4 sporozoites). (You know right? sporozoites are infective stages of malarial parasite).
Tachyzoites
 - Crescent-shaped with a pointed anterior and a rounded posterior end.
- Crescent-shaped with a pointed anterior and a rounded posterior end.
- Multiply rapidly in any cells of the intermediate hosts and non-enteric cells of definitive hosts.
- Active multiplying form seen during the acute stage of infection.
- Enters the host cell by active penetration of the host cell membrane.
- Group of proliferating tachyzoites within a host cell are known as pseudocyst.
Bradyzoites
 - Occurs in chronic infection
- Occurs in chronic infection
- Asexual stages of the parasite
- Bradyzoites are found within the tissue cysts and multiply very slowly.
- Although the tissue cysts may develop in visceral organs such as the lungs, liver and kidneys, they are more prevalent in neural and muscular tissues, including the brain, eyes, and skeletal and cardiac muscles.
- Intact tissue cysts can persist for the life of the host and do not cause inflammatory response.
Life Cycle
An infected cat shed unsporulated oocysts in its feces for 1-2 weeks. After 1-5 days oocysts sporulate in the environment and become infective. Intermediate hosts in nature (including birds, rodents, and even humans) become infected after ingesting soil, water, or plant material contaminated with sporulated oocysts. Humans are also infected by the ingestion of raw meats, particularly pork, lamb, or venison.
This delay is clinically significant: freshly shed cat feces are not immediately infectious. A pregnant woman who changes the litter box daily (removing oocysts before sporulation can occur) is at much lower risk than one who allows feces to accumulate for several days.
Oocysts transform into tachyzoites shortly after ingestion. These tachyzoites localize in the neural and muscle tissue of intermediate hosts and develop into tissue cyst bradyzoites.
 Figure: Life Cycle of Toxoplasma gondii(image source: CDC)
Figure: Life Cycle of Toxoplasma gondii(image source: CDC)
Cats become infected after
- consuming intermediate hosts (eg. rodents, birds, or raw meat) harboring tissue cysts (3-10 days developmental cycle).
- or directly by ingestion of sporulated oocysts (19-48 days developmental cycle).
In cats, some merozoites are transformed into the sexual stages, initiating gametogony. After sexual fusion of micro and macrogametes, oocysts develop, exit from the host cell into the gut lumen, and pass out via feces.
In the human host, the parasites form tissue cysts, most commonly in skeletal muscle, myocardium, brain, and eyes; these cysts may remain throughout the life of the host.
Signs and symptoms
The clinical outcomes of T. gondii infection are determined almost entirely by the host's immune status rather than by the virulence of the organism. The tachyzoite (the rapidly multiplying form) is responsible for acute tissue destruction. Under immune pressure from CD4+ T lymphocytes and the interferon-gamma (IFN-γ) they produce, tachyzoites are forced to convert to the slow-growing bradyzoite form, which encysts in neural and muscular tissue. Once encysted, bradyzoites are effectively invisible to the immune system (particularly in the brain, an immunologically privileged site) and cause no ongoing inflammation. The host and parasite reach a stable standoff that can last for decades.
This standoff has a critical vulnerability: it depends on CD4+ T-cell surveillance. Remove the surveillance (through HIV infection, immunosuppressive therapy, or malignancy) and the standoff collapses. Cysts rupture, bradyzoites convert back to tachyzoites, and focal encephalitis develops at the cyst sites. This is why toxoplasmic encephalitis in AIDS is classified as reactivation disease, not new infection, and why empirical anti-Toxoplasma treatment works: the organism is already present, latent; the treatment targets the newly emerged tachyzoites before they cause irreversible neurological damage.
Tachyzoites of the parasite Toxoplasma gondii may be found in circulating blood. They invade cells within lymph nodes and other organs, including the lungs, liver, heart, brain, and eyes. The resulting cellular destruction accounts for the manifestation of toxoplasmosis.
- Actively proliferating tachyzoites are seen in acute phase of infection and infect adjacent cells- continually expanding focal lesion.
- Formation of tissue cyst occurs as a result of host immune reaction. In this phase, there will be no multiplication, no dissemination of the parasite.
- Immunocompromised/immunodeficient individual: Cyst rupture or primary exposure to the organism may lead to the lesion. The organisms can be disseminated via the lymphatics and the bloodstream to other tissues.
Immunocompetent Patients
Usually asymptomatic or very mild infection in approximately 90% of serologically positive individuals.
Common symptoms
- No clinical symptoms in acute infections (in 80-90% of cases)
- Cervical lymphadenopathy (10-20% cases) and
- other symptoms of generalized infection (fever, malaise, night sweats, myalgia, sore throat and maculopapular rash).
Immunocompromised Patients
Infection in immunocompromised patients can lead to severe complications depending on the presence of underlying diseases such as malignancies, AIDS, and organ transplantation. In immunocompromised patients, the central nervous system (CNS) is primarily involved
Important symptoms
Diffuse encephalopathy, meningoencephalitis, or cerebral mass lesions.
50% patients show an altered mental state, motor impairment, seizures, abnormal reflexes and other neurologic sequelae.
- These infections usually stem from reactivated latent infection, rather than newly acquired infection.
Congenital Infection
If a mother acquired infection before becoming pregnant unborn child is protected by the mother’s immunity. Mother’s blood contains IgG antibodies against T. gondii which can cross the placenta and reach the fetus.
If a mother is primarily infected with Toxoplasma during pregnancy or just before pregnancy, she can pass the infection on to the fetus. Congenital infections may be particularly severe if the mother acquires the infection during the first or second trimester of pregnancy. The mother may not have any symptoms from the infection or mild morbidity (flu-like illness) but the infant may develop serious symptoms later in life, such as blindness or mental disability.
 Figure: A girl with hydrocephalus due to congenital Toxoplasma infection
Figure: A girl with hydrocephalus due to congenital Toxoplasma infection
Time determines the fate
- If Toxoplasma crosses the placenta early (1st trimester): severe congenital infections (intracerebral calcifications, chorioretinitis, hydro- or microcephaly, convulsions, mental retardation) may occur.
- If Toxoplasma crosses the placenta later (2nd-3rd trimester): infection may be inapparent but may lead to progressive blindness in the child later in life (teens).
- Secondary Infection: Maternal antibodies (secondary infection) protect the fetus during pregnancy, even if the mother is re-exposed during pregnancy.
Laboratory Diagnosis
Diagnosis of toxoplasmosis is usually achieved by serology. Test for the presence of specific IgG or IgM is used to determine if a person has an acute infection with Toxoplasma or immunity due to prior infection. Other procedures include performing PCR, examining biopsy specimens, buffy coat cells or CSF fluid, and isolating the organism in tissue culture or in laboratory animals.
Laboratory diagnosis methods
- Serology
- Giemsa stain and examining biopsy specimens, buffy coat cells, or cerebrospinal fluid
- Isolating the organism in tissue culture or in laboratory animals.
- Molecular methods: Performing PCR
Serology
- Serological tests are often recommended as diagnostic approach of choice but the interpretation of serological tests are complex.
- Specific IgM normally develops early, within 1-2 weeks after primary infection and IgG normally develops within 4 weeks after infection. Antibodies titer may peak within 4-8 weeks of infection.
- A four fold rise in IgG antibody titer is required to support the diagnosis of acute febrile toxoplasmosis.
- All newborns from mother who are antibody positive will have passively transferred maternal IgG. Titers can be high but may not indicate infection in in the baby.
- Detection of IgM antibodies (which do not cross the placenta) provides a much more accurate indication of infection in the newborn.
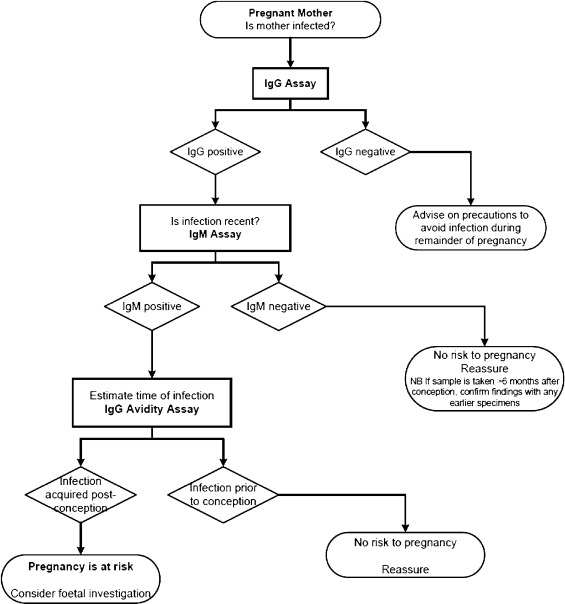 Figure: Toxoplasmosis: risk management in pregnancy (Chart source: European Journal of Obstetrics and Gynecology and Reproductive Biology)
Figure: Toxoplasmosis: risk management in pregnancy (Chart source: European Journal of Obstetrics and Gynecology and Reproductive Biology)
Sabin-Feldman Dye Test
Developed by Sabin and Feldman in 1948, this was the first quantitative serological test for toxoplasmosis and remains the historical gold standard, though it is now rarely performed outside reference laboratories.
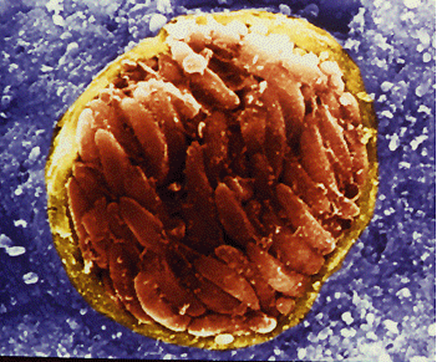
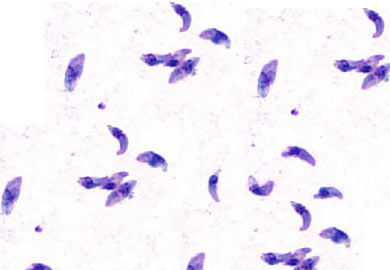 Figure: Tachyzoites of T. gondii
Figure: Tachyzoites of T. gondii
Principle: Live T. gondii tachyzoites are incubated with patient serum and complement. In the presence of specific anti-Toxoplasma antibodies, complement-mediated lysis kills the tachyzoites — dead cells fail to take up methylene blue dye (positive test, cells unstained). Without antibodies, tachyzoites survive and stain blue normally (negative test). The degree of lysis is assessed at serial serum dilutions to determine the antibody titer.
Limitations:
- Requires live, virulent T. gondii tachyzoites — a significant biohazard requiring Biosafety Level 2 conditions and regular passage in mice or cell culture
- Only available in specialist reference laboratories — not feasible for routine diagnostic use
- The use of live organisms raises ongoing animal ethics concerns regarding experimental animal use
- Technically demanding: results are operator-dependent and require experienced laboratory staff
- Has been largely superseded by ELISA-based serological methods that do not require live organisms, are safer, and are reproducible across laboratories
Clinical note: A negative Sabin-Feldman test effectively excludes Toxoplasma antibody. A positive result confirms exposure. In practice, ELISA for IgG and IgM has replaced this test in most diagnostic settings, and the Sabin-Feldman test is now used primarily as a reference confirmatory method or for research.
Microscopy
- Smears or sections stained with Giemsa or other special stains eg. PAS.
- Tachyzoites of T. gondii in the smear are cresent shaped (malarial parasite Plasmodium falciparum also has crescent shaped gaemtocytes) and in sections round to oval
- Tissue cysts are usually spherical and lack septa
Culture
T. gondii can be isolated by intraperitoneal inoculation of body fluid or tissue in infection-free laboratory mice. Peritoneal fluid and spleen smears may show the tachyzoites after 7-10 days.
Molecular methods
Detection of a specific region of DNA of Toxoplasma in the sample (eg. Blood, CSF, etc). Prenatal diagnosis of congenital toxoplasmosis from amniotic fluid.
Treatment of Toxoplasmosis
Immunocompetent adults with acquired toxoplasmosis Usually self-limiting and requires no treatment. The immune system controls the infection and drives conversion to the latent bradyzoite stage without intervention.
Toxoplasmic encephalitis in immunocompromised patients (standard regimen): The combination of pyrimethamine + sulfadiazine + leucovorin (folinic acid) is the first-line treatment:
- Pyrimethamine inhibits dihydrofolate reductase (DHFR) in T. gondii, blocking folate synthesis and therefore DNA synthesis in the parasite
- Sulfadiazine inhibits dihydropteroate synthase, an earlier step in the same folate pathway, producing synergistic blockade
- Leucovorin is added specifically to protect the host — pyrimethamine also inhibits human DHFR, causing bone marrow suppression (neutropenia, thrombocytopenia). Leucovorin (folinic acid) is already in the reduced form and can be used directly by host cells without going through DHFR, bypassing the drug's toxic effect on human cells. Toxoplasma cannot utilise folinic acid this way, so leucovorin rescues host cells without rescuing the parasite.
Duration: Acute treatment for 6 weeks, followed by lifelong secondary prophylaxis (lower-dose pyrimethamine + sulfadiazine) until immune reconstitution on antiretroviral therapy raises the CD4 count sustainably above 200.
Primary prophylaxis: HIV-positive patients with CD4 <100 receive trimethoprim-sulfamethoxazole (TMP-SMX) as primary prophylaxis against toxoplasmic encephalitis, the same drug used for PCP prophylaxis — a convenient dual coverage.
Pregnant women:
- Spiramycin is used for confirmed maternal infection before 18 weeks' gestation and before fetal infection is confirmed. It reduces the risk of transmission to the fetus but does not cross the placenta in significant concentrations to treat an already-infected fetus.
- If fetal infection is confirmed (by PCR on amniotic fluid) or after 18 weeks, pyrimethamine + sulfadiazine + leucovorin is used — noting that pyrimethamine is potentially teratogenic and is generally avoided in the first trimester.
Congenital toxoplasmosis: Infected neonates receive pyrimethamine + sulfadiazine + leucovorin for the first year of life, even if asymptomatic at birth, because untreated congenital infection can lead to progressive chorioretinitis and neurological deterioration later in childhood.
How to Remember
Tachyzoite = "tachy" = fast = acute disease; Bradyzoite = "brady" = slow = chronic/latent. The Greek prefixes do the work: tachy (fast) describes the rapidly multiplying form seen in acute infection; brady (slow) describes the slowly dividing form that hides in tissue cysts during chronic, latent infection. This prefix anchor makes the exam distinction between acute toxoplasmosis (tachyzoites) and reactivation encephalitis (bradyzoite cyst rupture → tachyzoites) a matter of understanding, not memorisation.
Cats are the only definitive host — sexual reproduction happens only in feline intestinal epithelium. The cat specificity is biological, not arbitrary. T. gondii can only complete its sexual life cycle in the intestinal epithelium of felids. All other warm-blooded hosts (including humans) are intermediate hosts where only asexual multiplication occurs. "Only in cat, only in cat gut, only producing oocysts" three levels of specificity to anchor the cat's unique role.
Freshly shed cat feces are NOT immediately infective — and this matters clinically. Oocysts shed in cat feces are unsporulated and non-infective. They require 1-5 days in the environment to sporulate and become infectious. This means: a pregnant woman who changes the litter box daily (so oocysts never have time to sporulate) is at much lower risk than one who allows the box to accumulate. This is a real public health counselling point and an exam trap.
Leucovorin rescues humans but not Toxoplasma — this is why it's added to the treatment regimen. Pyrimethamine blocks DHFR in both the parasite and the host. Leucovorin (folinic acid) is the already-reduced form of folate that bypasses DHFR — human cells can use it directly; Toxoplasma cannot. Adding leucovorin to pyrimethamine + sulfadiazine therapy is therefore selective host rescue, not a weakening of the antiparasitic effect.
Maternal IgG protects the fetus — but only if the mother was infected before, not during, pregnancy. If the mother already has IgG (from prior infection), transplacental transfer of those antibodies protects the fetus. If the mother acquires a primary infection during pregnancy, she hasn't yet made protective IgG when it matters most. This is why TORCH screening asks specifically about IgG (prior immunity = fetal protection) and IgM (current primary infection = fetal risk).
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Phylum / Class | Apicomplexa / Sporozoasida |
| Definitive host | Felids (domestic cats and relatives) only — sexual reproduction |
| Intermediate hosts | Humans, birds, rodents, pigs, cattle — asexual stages only |
| Three infectious stages | Oocyst (sporulated, from cat feces), Tachyzoite (acute, rapidly multiplying), Bradyzoite (chronic, encysted) |
| Oocyst content | 2 sporocysts × 4 sporozoites = 8 sporozoites per oocyst |
| Sporulation requirement | 1–5 days outside the host before infective — freshly shed oocysts are NOT immediately infective |
| Tachyzoite characteristic | Crescent-shaped, rapidly multiplying, seen in acute infection and dissemination |
| Bradyzoite location | Predominantly neural tissue (brain) and muscle — immune-privileged site |
| Reactivation trigger | Loss of CD4+ T-cell surveillance (CD4 <100 in HIV) → cyst rupture → tachyzoites re-emerge |
| Clinical presentation in AIDS | Ring-enhancing brain lesion(s) on CT/MRI — multiple, with surrounding oedema |
| Congenital: first trimester | Severe — intracerebral calcifications, hydro/microcephaly, chorioretinitis, mental retardation |
| Congenital: second/third trimester | Milder but progressive chorioretinitis in later life |
| Maternal IgG significance | Pre-existing IgG crosses placenta and protects fetus — primary infection DURING pregnancy is the risk |
| Key diagnostic test | IgG + IgM serology; IgM indicates recent/acute infection |
| Sabin-Feldman dye test | Antibody-mediated lysis of live tachyzoites → fail to take up methylene blue; gold standard but uses live organisms |
| Treatment | Pyrimethamine + sulfadiazine + leucovorin (acute); secondary prophylaxis lifelong in AIDS |
| Leucovorin role | Rescues host cells from pyrimethamine's DHFR inhibition; Toxoplasma cannot utilise folinic acid |
| Primary prophylaxis (AIDS, CD4 <100) | TMP-SMX (covers both Toxoplasma and PCP) |
| Pregnancy treatment | Spiramycin (before 18 weeks, no confirmed fetal infection); pyrimethamine + sulfadiazine + leucovorin (confirmed fetal infection or after 18 weeks) |
Where Students Get Confused
"Toxoplasma encephalitis in AIDS is a new infection." It is almost always reactivation of a latent infection acquired years earlier. The patient already had T. gondii cysts in their brain before their AIDS diagnosis; immune collapse allows those cysts to rupture and cause disease. This is why empirical treatment works rapidly (the organism is susceptible, already present, and predictable), and why serological testing for IgG has clinical utility — a negative IgG in an AIDS patient with a ring-enhancing lesion makes Toxoplasma much less likely (the patient has no latent infection to reactivate).
"Tachyzoites and the crescent-shaped gametocytes of Plasmodium falciparum are the same thing." The article correctly flags this potential confusion with an inline note. Both are crescent-shaped under the microscope, but they are entirely different organisms at different stages of completely different life cycles. Tachyzoites are Toxoplasma's rapidly replicating intracellular form; P. falciparum crescent-shaped gametocytes are sexual-stage malarial parasites seen in peripheral blood smears. The shape similarity is coincidence of geometry, not biological relationship.
"IgM-positive serology in a pregnant woman always means the baby is at risk." Not necessarily. IgM can persist for months to years after primary infection in some individuals. A positive IgM does not definitively distinguish recent infection from an infection acquired 6-12 months ago. This is why IgG avidity testing (measuring how tightly IgG antibodies bind to antigen — low avidity = recent infection, high avidity = older infection) is used to time the infection more precisely when the clinical question is whether infection occurred before or during pregnancy.
"Freshly shed cat feces are immediately infectious." They are not. Oocysts require 1-5 days of environmental sporulation before becoming infective. A pregnant woman who changes the litter box daily is removing oocysts before they sporulate. The risk from cats comes from allowing feces to accumulate, gardening in soil contaminated with old cat feces, or consuming unwashed produce from such soil — not from immediate contact with fresh feces.
"Leucovorin weakens the anti-Toxoplasma effect of pyrimethamine." It does not. Leucovorin (folinic acid) is the pre-reduced form of folate that bypasses DHFR entirely. Human cells can directly utilise it. Toxoplasma cannot — the parasite lacks the transport mechanism to take up folinic acid. Adding leucovorin specifically rescues host bone marrow and gastrointestinal cells from pyrimethamine's toxicity without giving the parasite any protection from the drug.
References and further readings
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- Montoya, J. G., & Liesenfeld, O. (2004). Toxoplasmosis. The Lancet, 363(9425), 1965–1976. https://doi.org/10.1016/S0140-6736(04)16412-X
- Robert-Gangneux, F., & Dardé, M. L. (2012). Epidemiology of and diagnostic strategies for toxoplasmosis. Clinical Microbiology Reviews, 25(2), 264–296. https://doi.org/10.1128/CMR.05013-11
- Sabin, A. B., & Feldman, H. A. (1948). Dyes as microchemical indicators of a new immunity phenomenon affecting a protozoon parasite (Toxoplasma). Science, 108(2815), 660–663. https://doi.org/10.1126/science.108.2815.660
- Reiter-Owona, I., Petersen, E., Joynson, D., Aspöck, H., Demar-Pierre, M., Derouin, F., Engelbrecht, F., Gross, U., Hassl, A., Holliman, R., Janitschke, K., Jenum, P. A., Naser, K., Olszewski, M., Thulliez, P., & Seitz, H. M. (1999). The past and present role of the Sabin-Feldman dye test in the serodiagnosis of toxoplasmosis. Bulletin of the World Health Organization, 77(11), 929–935. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2557769/
- Centers for Disease Control and Prevention. (2024). Toxoplasmosis (Toxoplasma infection). https://www.cdc.gov/parasites/toxoplasmosis/
Frequently Asked Questions
How is congenital toxoplasmosis diagnosed in a newborn when the mother is IgG-positive?
Why does the timing of maternal Toxoplasma infection during pregnancy affect the severity of congenital disease?
What is the treatment for Toxoplasma infection during pregnancy?
Why can toxoplasmosis reactivate years after the initial infection in immunocompromised patients?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.