Quantitative Buffy Coat (QBC) Test: Principle, Procedure, Results, and Applications
Learn how the QBC test uses acridine orange and fluorescence microscopy to diagnose malaria, filariasis, and visceral leishmaniasis — with procedure, results interpretation, and comparison with thick smear and RDT.
A night-duty technician in a busy hospital laboratory receives twelve blood samples at once — all from febrile patients, all marked urgent, all suspected malaria. Preparing and reading twelve thick smears takes skill, time, and a well-trained eye. The Quantitative Buffy Coat test offers an alternative: a small capillary tube pre-loaded with stain and anticoagulant, a five-minute centrifugation, and fluorescent parasites that glow visibly against a dark background — readable in under five minutes per tube.
QBC was developed specifically to address the gap between microscopy's accuracy and the speed and throughput demands of high-burden malaria settings. It is also one of the few diagnostic platforms that serves three different parasitic diseases on a single principle — malaria, lymphatic filariasis, and visceral leishmaniasis. Understanding how and why it works, where it outperforms thick smear, and where it falls short, is essential for any student or laboratory scientist working in tropical or subtropical medicine.
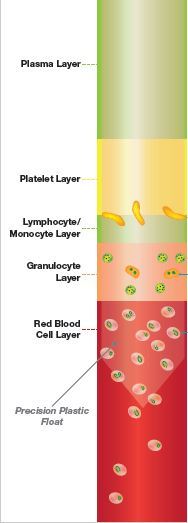 Figure: QBC Test System
Figure: QBC Test System
The acridine orange stains all nucleic acid-containing cells and the associated fluorescence is observable under blue-violet light through a microscope.
According to the manufacturer, QBC Malaria Test is 5.5 to 7% more sensitive than Giemsa thick films. It can detect as little as 1 parasite per μL of blood and establish diagnosis earlier than thick film in 47% of low parasitemia (<10 parasites per μL) cases.
QBC is established as an effective tool for diagnosing blood parasites that cause malaria, filariasis, and visceral leishmaniasis.
Why Use QBC?
Thick and thin blood smear microscopy remains the gold standard — it detects the parasite, identifies the species, and quantifies parasitaemia. But it has limitations in specific scenarios:
- It requires a trained microscopist comfortable with Giemsa morphology
- Sensitivity drops in low parasitaemia infections where very few parasites circulate
- Reading a well-made smear takes 20–30 minutes per sample
QBC addresses the first two problems directly. Its fluorescent signal is visually easier to detect than the subtle morphological differences on a Giemsa smear, and its concentration step (centrifugation) physically accumulates parasites into a narrow band — improving sensitivity for low-level infections.
When QBC has a real clinical advantage:
- Low parasitaemia: QBC detects as few as 1 parasite/μL, compared to 10–20 parasites/μL for thick smear. In early infection or partially treated cases, QBC may be positive when thick smear is negative.
- High-throughput screening: In field epidemiology or outbreak settings, multiple tubes can be processed in a single centrifuge run.
- Screening without specialist microscopists: The fluorescent signal is less subjective than morphological identification on Giemsa and can be read more quickly after basic training.
When QBC has real limitations (see Advantages and Limitations section below).
Principle
Acridine orange binds deoxyribonucleic acids and ribonucleic acids. The malaria parasite binds acridine orange in the nucleus and the cytoplasm and emits green and red fluorescence when excited by blue light (at 460 nm) allowing the detection and examination of parasite morphology by fluorescent microscopy. The nuclei of the parasites emit yellowish-green fluorescence whereas the cytoplasm exhibits bright red fluorescence.
RBCs are not stained by the dye, hence remain inconspicuous under fluorescent light (dark background) while the brightly fluorescent parasites are easily seen. The outlines of stained parasites are well preserved and the general morphology is similar to that in specimens stained by the Giemsa stain.
Sample collection: Blood sample can be collected in either capillary finger-prick or phlebotomy in an ethylenediamine tetraacetate (EDTA) containing vials.
About the QBC tube
The QBC glass capillary tube (Becton Dickinson) is 75 mm in length and 1.677 mm in diameter. The tubes are internally coated with EDTA and heparin at the fill end and with acridine orange stain and potassium oxalate at the other end.
Procedure
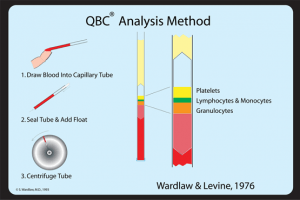 Figure: QBC analysis Method
Figure: QBC analysis Method
- Draw samples of blood ( 55 µl) into the QBC tube by capillary action.
- Rotate the tubes for 10 seconds to dissolve the contained residues in the blood.
- Insert a close-fitting cylindrical insert or plastic float {having a specific gravity (1.055) i.e midway between that of plasma (1.028) and red blood cells (1.090)} inside acridine orange-coated capillary tube.
- Centrifuge tubes at 12,000 g for 5 minutes. After centrifugation blood components and malaria parasites separate based on density and concentrate in distinct layers. Note: The float by virtue of its density settles on top of the centrifuged packed red cells. It occupies 90% cross-sectional area of the tube which aids in the expansion of the centrifugally separated cell layers. It is surrounded by three discernible and now measurable layers of the buffy coat.
- Insert the centrifuged QBC Malaria test into the Paraviewer. Position the tube so the closure end extends over the depressed area of the holder.
- The area surrounding the float just beneath the buffy coat was examined under oil immersion. Individual cells within this layer were easily seen by microscopy; the malaria parasites staining green (DNA) and orange (RNA) under blue-violet light.
- The entire circumference of the tube was examined systematically while moving away from the buffy coat through the erythrocyte layer.
- Each tube was examined until parasites were detected or for a maximum of 5 minutes.
Results/Analysis
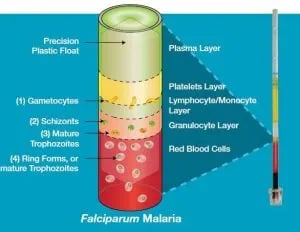 Figure: Falciparum malaria in QBC Test
Figure: Falciparum malaria in QBC Test
If a sample contains P. falciparum malaria parasites:
- Crescent-shaped gametocytes (1) will appear near the interface of the lymphocyte/monocyte and platelet layers.
- A small number of (2) schizonts and (3) mature trophozoites may appear in the granulocyte layer.
- Ring-shaped (4) immature trophozoites will appear throughout the red blood cell layer, with a concentration near the interface with the granulocyte layer.
Other parasites species, including P. vivax, will also concentrate during centrifugation, but exhibit different characteristics.
Results for P. vivax and Other Species
Unlike P. falciparum, which sequesters its mature forms in deep capillaries, P. vivax (and P. malariae, P. ovale) circulate all stages in peripheral blood. On QBC:
- Trophozoites of P. vivax distribute throughout the RBC layer and fluoresce green-yellow
- Enlarged RBCs (characteristic of P. vivax) may be visible as larger fluorescent forms compared to P. falciparum rings
- Schüffner's dots are not reliably visible on QBC — this is one reason species differentiation is harder on QBC than on Giemsa thin smear
- Gametocytes of P. vivax are round and concentrate in the lymphocyte layer (unlike the crescents of P. falciparum which have a characteristic position near the platelet layer)
Critical point: QBC can confirm the presence of malaria parasites and give a probable species identification based on layer position and morphological impressions — but definitive species identification requires a Giemsa-stained thin smear. This is not a limitation unique to QBC; it is the standard workflow: QBC (or thick smear) for detection → thin smear for confirmation of species.
QBC for Other Parasitic Infections
The opening paragraph correctly states that QBC diagnoses malaria, filariasis, and visceral leishmaniasis. Here is what each application involves.
Lymphatic Filariasis (Wuchereria bancrofti, Brugia spp.)
Blood for filarial diagnosis must be collected at night (between 10 p.m. and 2 a.m.) to coincide with nocturnal periodicity of microfilariae in peripheral blood — this timing rule applies to QBC exactly as it does to thick smear.
After centrifugation, microfilariae concentrate just above the buffy coat layer (granulocyte–lymphocyte interface), where they fluoresce brilliantly with acridine orange under UV light. Their characteristic sinuous, actively motile form is often visible even without species identification.
Advantage over thick smear for filariasis: The concentration step dramatically increases sensitivity for low microfilarial density infections. QBC has been shown to be more sensitive than thick smear for detecting microfilariae, particularly in early or treated infections.
Limitation: Species identification of microfilariae on QBC is unreliable — the fluorescence reveals the worm's DNA but not the morphological features (sheath characteristics, nuclear column pattern) needed to distinguish W. bancrofti from Brugia malayi. A conventional Giemsa-stained thick smear or membrane filtration is needed for species identification.
Visceral Leishmaniasis (Kala-Azar)
In visceral leishmaniasis, Leishmania amastigotes (LD bodies) infect monocytes and macrophages. After QBC centrifugation, these infected cells concentrate in the buffy coat layer (lymphocyte/monocyte zone). Acridine orange stains the kinetoplast and nucleus of the amastigote, producing bright fluorescence that can be detected under UV.
Important limitation: QBC for VL is less well-validated than for malaria and filariasis. The sensitivity is lower than bone marrow aspirate microscopy or rK39 serology in most studies. QBC is not a replacement for standard VL diagnostic workup — its role is as an adjunct when other specimens are unavailable or when a rapid screen is needed before proceeding to invasive sampling.
Summary of QBC Applications
| Disease | Parasite detected | Layer in QBC tube | Timing of sample |
|---|---|---|---|
| Malaria (P. falciparum) | Gametocytes, rings, schizonts | Buffy coat / RBC interface | Any time (during fever preferred) |
| Malaria (P. vivax, others) | All stages | RBC layer (see Results section) | Any time |
| Lymphatic filariasis | Microfilariae | Just above buffy coat | Night collection (10 pm–2 am) |
| Visceral leishmaniasis | Amastigotes in monocytes | Buffy coat (monocyte layer) | Any time |
Advantages and Limitations of QBC
| Advantages | Limitations |
|---|---|
| Higher sensitivity than thick smear for low parasitaemia (detects 1 parasite/μL) | Requires fluorescence microscope and UV light source — expensive and not universally available |
| Detects earlier in infection — positive in 47% of low parasitaemia cases where thick smear is negative | Proprietary system (Paraviewer, specific QBC tubes) — ongoing reagent costs |
| Faster to read per sample once set up | Cannot reliably provide definitive species identification — thin smear still required |
| Less subjective than Giemsa morphology — easier to train staff | Cannot quantify parasitaemia accurately (no WBC or RBC counting method) |
| Pre-coated tubes reduce staining preparation time | Species layer positions can overlap — P. vivax and P. falciparum differentiation unreliable in mixed infections |
| Multiple tubes processed in one centrifuge run | "Gentrification" error in field settings — centrifuge speed inconsistency affects layer separation |
| Applicable to malaria, filariasis, and VL on the same platform | For filariasis: species ID not possible; for VL: lower sensitivity than bone marrow aspirate or rK39 |
| QBC malaria result available in ~10–15 minutes total | UV lamp requires maintenance; fluorescence fades if reading is delayed |
How QBC Compares to Other Malaria Diagnostic Methods
| Feature | Thick/Thin Smear | QBC | RDT (e.g. rK39, HRP-2) |
|---|---|---|---|
| Sensitivity | ~10–20 parasites/μL | ~1 parasite/μL | ~100–200 parasites/μL (variable) |
| Species ID | Yes (thin smear) | Probable only | Limited (T1/T2 format) |
| Parasitaemia quantification | Yes | No | No |
| Equipment needed | Light microscope | Fluorescence microscope + centrifuge | None |
| Skill required | High (Giemsa morphology) | Moderate | Minimal |
| Time to result | 30–60 minutes | 10–15 minutes | 5–15 minutes |
| Cost per test | Low | Moderate–high | Moderate |
| Field suitability | Yes (where microscopy available) | Limited (equipment) | Yes (true point-of-care) |
| Treatment monitoring | Yes (parasitaemia count) | No | pLDH-based only |
| Non-malaria parasites | With specific stains | Yes (filariasis, VL) | No |
Bottom line for clinical practice:
- RDT for rapid first-line screening of malaria in field settings
- Thick smear for confirmation, species ID, and parasitaemia quantification
- QBC where sensitivity for low parasitaemia is the priority and fluorescence microscopy is available
- Thin smear always required when definitive species identification matters clinically.
Where Students Actually Get Confused
1. "QBC replaces thick smear." No. QBC is more sensitive for detecting low parasitaemia, but it cannot replace thick smear for two specific functions: definitive species identification and parasitaemia quantification. In severe falciparum malaria, knowing that parasitaemia is 8% (severe, may need IV artesunate) vs 0.5% (uncomplicated) is a critical clinical distinction that QBC cannot provide. QBC and thick smear are complementary.
2. "Acridine orange stains malaria parasites specifically." Acridine orange stains all nucleic acid-containing cells — it is not malaria-specific. WBCs, platelets with DNA content, and any nucleated cell will fluoresce. What makes parasite identification possible is the combination of: the fluorescence pattern (green nucleus, red-orange cytoplasm), the characteristic morphology of parasitic forms, and their specific location in the centrifuged layers. A technician unfamiliar with the expected layer positions can confuse WBC fragments or cellular debris with parasites.
3. "QBC works the same for filariasis and malaria." The principle (acridine orange + centrifugation + fluorescence) is the same, but the critical difference is timing of sample collection. For malaria, collect at any time (preferably during fever). For lymphatic filariasis, collect strictly between 10 pm and 2 am to coincide with nocturnal periodicity of microfilariae. Missing this window for filariasis gives a false-negative result — the parasites are simply not in peripheral blood at other times.
4. "The float sinks to the bottom during centrifugation." The float (specific gravity 1.055) is specifically designed to settle between plasma (1.028) and packed RBCs (1.090) — it sits just above the buffy coat after centrifugation. This is the key engineering insight of QBC: by occupying 90% of the tube's cross-sectional area at that position, it physically expands the buffy coat layer, making it much easier to see and examine under the microscope. It does not sink to the bottom.
5. "QBC can identify mixed malaria infections reliably." Mixed infections (e.g. P. falciparum + P. vivax co-infection) are notoriously difficult to detect on QBC because the layer positions of different species overlap and the morphological differentiation under fluorescence is less precise than on Giemsa. Mixed infections are better identified on Giemsa thin smear after QBC has screened positively.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Stain used | Acridine orange (pre-coated in QBC tube) | Binds DNA + RNA → fluorescence |
| Excitation wavelength | 460 nm (blue-violet light) | UV/blue light → green + red glow |
| Nucleus fluorescence colour | Yellowish-green (DNA) | Green = genetic material |
| Cytoplasm fluorescence colour | Bright red-orange (RNA) | Red = cytoplasm |
| RBC appearance | Dark (no fluorescence) | Unstained background = easier contrast |
| Centrifugation speed | 12,000 g for 5 minutes | High speed, short time |
| Float specific gravity | 1.055 | Between plasma (1.028) and RBCs (1.090) |
| Float function | Expands buffy coat layer to 90% cross-section | Makes parasites visible and locatable |
| Detection threshold | 1 parasite/μL | 10–20× more sensitive than thick smear |
| P. falciparum crescent gametocytes | Near lymphocyte/monocyte–platelet interface | Crescents float high |
| P. falciparum ring forms | Throughout RBC layer, concentrated near granulocyte interface | Rings throughout |
| Filariasis: microfilariae location | Just above buffy coat | Worms concentrate at top of cell layer |
| Filariasis: sample timing | Night collection (10 pm–2 am) | Nocturnal periodicity |
| VL: amastigote location | Buffy coat (monocyte layer) | LD bodies in monocytes |
| Species ID possible? | Probable only — thin smear required for definitive ID | QBC detects; smear identifies |
| Parasitaemia quantification | Not possible on QBC | Use thick smear WBC count method |
| Key limitation | Fluorescence microscope required; expensive proprietary system | Not a true field test |
Self-Check Questions
- A thick blood smear is negative in a patient with clinical features strongly suggestive of malaria. Why might a QBC test be positive in the same patient?
- A laboratory receives a blood sample labelled "rule out filariasis." The sample was collected at 10 a.m. The QBC test is negative. Can you confidently exclude filariasis?
- What is the function of the plastic float in the QBC tube, and what is its specific gravity?
- QBC shows a positive fluorescent signal in the buffy coat layer. The patient's clinical picture is consistent with kala-azar. What is the next most appropriate diagnostic step?
- Why can't QBC replace the thin blood smear in confirmed malaria cases?
- A QBC tube shows bright fluorescent forms in the RBC layer as well as crescent-shaped forms near the lymphocyte layer. Which Plasmodium species is most likely?
Answers:
1. QBC detects as few as 1 parasite/μL via physical concentration; thick smear sensitivity is ~10–20 parasites/μL. In low parasitaemia infections (early disease, partially treated cases), QBC detects parasites below the thick smear threshold.
2. No — the sample was collected outside the nocturnal periodicity window (10 pm–2 am). Microfilariae of W. bancrofti are not present in peripheral blood in significant numbers during the day. Repeat with night-time sample before excluding filariasis.
3. The float expands the buffy coat layer to 90% of the tube's cross-sectional area, physically separating and enlarging the zone where parasites concentrate; specific gravity = 1.055, which sits between plasma (1.028) and packed RBCs (1.090).
4. QBC is not a validated stand-alone test for VL. Proceed to bone marrow aspirate for LD body microscopy ± culture, and/or rK39 rapid test — these are the standard confirmatory investigations.
5. The thin smear is required for: (a) definitive species identification based on RBC morphology and parasite stage, and (b) parasitaemia quantification — critical for assessing severity and guiding treatment intensity in falciparum malaria. QBC cannot provide either reliably.
6. P. falciparum — crescent-shaped gametocytes near the lymphocyte/platelet interface are pathognomonic for P. falciparum; ring forms throughout the RBC layer are consistent.
References
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- Wongsrichanalai, C., Barcus, M. J., Muth, S., Sutamihardja, A., & Wernsdorfer, W. H. (2007). A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT). American Journal of Tropical Medicine and Hygiene, 77(6 Suppl), 119–127. https://www.ncbi.nlm.nih.gov/books/NBK1695/
- Long, G. W., Jones, T. R., Rickman, L. S., et al. (1994). Acridine orange diagnosis of Plasmodium falciparum: evaluation after experimental infection. American Journal of Tropical Medicine and Hygiene, 51(5), 613–616. https://doi.org/10.4269/ajtmh.1994.51.613 (This is the source for the "47% earlier detection in low parasitaemia" and "1 parasite/μL" figures cited in the article)
- Snounou, G., Viriyakosol, S., Jarra, W., Thaithong, S., & Brown, K. N. (1993). Identification of the four human malaria parasite species in field samples by the polymerase chain reaction and detection of a high prevalence of mixed infections. Molecular and Biochemical Parasitology, 58(2), 283–292. https://doi.org/10.1016/0166-6851(93)90050-8
- Makler, M. T., Palmer, C. J., & Ager, A. L. (1998). A review of practical techniques for the diagnosis of malaria. Annals of Tropical Medicine and Parasitology, 92(4), 419–433. https://doi.org/10.1080/00034983.1998.11813307
- Rickman, L. S., Long, G. W., Oberst, R., et al. (1989). Rapid agglutination testing for detection of Plasmodium falciparum antigens. Annals of Internal Medicine, 111(12), 1001–1003. (Background on pre-QBC fluorescence malaria diagnostics)
- Saxena, R., Bhatt, A., Sharma, R., Oommen, A., & Garg, K. (2007). Usefulness of quantitative buffy coat blood parasite detection system in diagnosis of malaria. Medical Journal of the Armed Forces India, 63(3), 247–249. https://pubmed.ncbi.nlm.nih.gov/17664839/
- World Health Organization. (2016). Malaria microscopy quality assurance manual (Version 2). WHO. https://www.who.int/publications/i/item/9789241549394
Frequently Asked Questions
What is the principle of the QBC test for malaria?
How sensitive is the QBC test compared to thick blood smear?
Can QBC be used to diagnose filariasis?
What is the purpose of the plastic float in the QBC tube?
Why can't QBC replace the thin blood smear?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.