Periodic Acid-Schiff (PAS) Staining: Principle, Procedure, and Microbiology Applications
PAS staining detects fungi in tissue biopsies, diagnoses Whipple's disease, and identifies glycogen storage disorders. Learn the principle, procedure, results, and clinical applications in microbiology and pathology.
A 52-year-old farmer presents with a two-year history of weight loss, intermittent diarrhoea, and joint pain that no rheumatologist has been able to explain. An intestinal biopsy is taken. Under the microscope, the lamina propria is packed with foamy macrophages that stain an intense magenta — PAS-positive macrophages. The diagnosis is Whipple's disease, caused by Tropheryma whipplei, and it has been missed for two years because nobody requested this stain.
In a second case: an immunocompromised patient post-transplant develops a pulmonary infiltrate. BAL is negative. A transbronchial biopsy is taken. PAS staining reveals magenta-staining hyphae with acute-angle branching — Aspergillus fumigatus invading lung parenchyma.
PAS staining is the histopathologist's workhorse for detecting organisms and substances that contain carbohydrates — fungal cell walls, parasite cyst walls, glycogen deposits, and the macrophages of Whipple's disease. Understanding when to request it and how to interpret it separates a complete clinical microbiologist from one who only works with cultures.
Periodic acid-Schiff (PAS) is a staining technique for demonstrating the carbohydrates and fungal cell wall components. PAS can detect the presence of glycogen, polysaccharides, and mucin in the tissue that is either formalin-fixed, paraffin-embedded, or frozen tissue sections. PAS is performed in the laboratory for histological studies.
Principle of Periodic acid- Schiff (PAS) Staining
The periodic acid of the stain reacts with carbohydrates in an oxidative process. In this process, the polysaccharide and the periodic acid reaction form an oxidized compound- aldehyde. Now, the aldehyde reacts with the Schiff reagent, which gives the purple-magenta color. Similarly, the appearance of the pink color suggests the presence of intracellular or extracellular mucin. In contrast, using hematoxylin or methyl green as counter-stain helps in staining the nuclei. Likewise, a light green colored counter stain is preferred to demonstrate the fungal organisms.
What structures stain PAS-positive (magenta/purple):
- Fungal cell walls — chitin and glucan polysaccharides (key microbiology application)
- Glycogen — in liver, muscle, kidney
- Mucin — in goblet cells and mucus-secreting tumours
- Basement membranes — in renal glomeruli and blood vessels
- Tropheryma whipplei — within macrophage lysosomes in Whipple's disease
- Parasite structures — Cryptosporidium oocysts, Pneumocystis cyst walls (weakly)
What does NOT stain PAS-positive:
- Bacteria (no polysaccharide cell wall component in sufficient concentration)
- Nuclei (counterstained blue/green by haematoxylin or methyl green)
- Non-carbohydrate proteins and lipids
Solutions and Reagents
0.5% Periodic Acid Solution
- Periodic acid crystals-0.5 g
- Distilled water-100 ml
To prepare 0.5% periodic acid solution mix 0.5 g periodic acid crystals in 100 ml distilled water.
Schiff’s reagent
Dissolve 5 g basic fuchsin in 900 ml boiled water. Once it is cools to 50°C add 100 ml 1M HCl to the mixture. Again add 10 g of K2S2O5 once the mixture cools down to 25°C. After completely mixing, shake the solution for 3 minutes and let it incubate for 24 hours in a dark room.
After incubation, add 5 g of activated charcoal to the mixture. Then shake the solution for 3 minutes and filter. The refiltration and retreatment of the solution are necessary if the solution is not crystal clear. Store the solution at 4°C in the foil-covered bottle. It is suitable to use the solution for 2-3 weeks if stored properly.
For testing the purity of the prepared Schiff’s reagent:
Pour 10 ml of 10% formalin into a beaker, then add a few drops of the prepared Schiff’s reagent. Then change in color is interpreted as
- The red-purple color means it is a good Schiff’s reagent.
- Deep blue-purple color means poor Schiff’s reagent (delayed reaction).
Mayer’s Hematoxylin
- Aluminum potassium sulfate (alum)- 50 gram
- Distilled water- 1000 ml
- Hematoxylin- 1 gram
- Sodium iodate- 0.2 gram
- Glacial acetic acid- 20 ml
Dissolve alum in distilled water. Add hematoxylin when alum is completely dissolved. When hematoxylin is completely dissolved, add sodium iodate and acetic acid. Then boil and cool it.
Procedure for Periodic Acid-Schiff (PAS) Staining
- Firstly remove the paraffin from the tissue sections by washing in distilled water.
- Then, place the tissue in 0.5% periodic acid solution for 5 minutes. It oxidizes the tissue.
- After that, rinse the tissue properly in distilled water.
- Then, cover it with Schiff’s reagent for 5-15 minutes which turns into light pink.
- After that, wash the stain for 5 minutes using lukewarm water, which turns it into dark pink.
- Then counter-stain the tissue using Mayer’s Hematoxylin for 1 minute.
- After that, wash it with running tap water for 5 minutes and rinse using distilled water.
- Finally, dehydrate the slide, place the coverslip and mount it using synthetic mounting media.
Troubleshooting PAS Staining
| Problem | Likely Cause | Action |
|---|---|---|
| Weak or absent magenta colour | Periodic acid too old/degraded; oxidation time insufficient | Replace periodic acid; extend oxidation to 10 minutes |
| Schiff reagent not producing magenta | Schiff reagent oxidised (should be colourless/pale yellow — discard if pink) | Replace Schiff reagent; store at 4°C in dark |
| Background too dark | Over-oxidation; counterstain too heavy | Reduce periodic acid time; reduce haematoxylin counterstain |
| Nuclei not staining | Haematoxylin too dilute or depleted | Replace haematoxylin solution |
| Fungal elements pale or missed | Tissue too thin; insufficient material | Request deeper sections; consider GMS in parallel |
Results interpretation for Periodic acid-Schiff (PAS) Staining
- Glycogen, mucin and some basement membranes-Red/ purple
- Fungi-Red/ purple
- Background-Blue
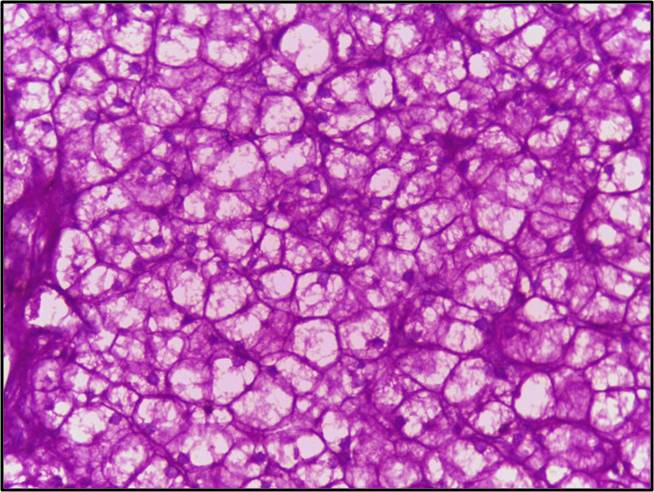 Figure: Liver biopsy of glycogen storage disorder PAS positive
Figure: Liver biopsy of glycogen storage disorder PAS positive
PAS Staining for Fungal Detection in Tissue
PAS is one of the two standard fungal tissue stains in clinical histopathology — the other being Gomori Methenamine Silver (GMS). Both stain the fungal cell wall, but they differ in what they highlight and how they are interpreted.
Fungal appearance on PAS: Cell walls and hyphae stain magenta to deep purple-red. Background tissue and nuclei stain blue (with haematoxylin counterstain) or green (with light green counterstain). The contrast makes fungal elements clearly visible even in complex tissue backgrounds.
Clinically important fungi identified by PAS in tissue:
| Organism | PAS Appearance | Key Morphological Feature |
|---|---|---|
| Aspergillus fumigatus | Magenta septate hyphae | Acute-angle (45°) branching; uniform width 2–4 μm |
| Mucor/Rhizopus (Mucorales) | Magenta non-septate hyphae | Wide-angle (90°) branching; ribbon-like, broad 6–25 μm |
| Candida albicans | Magenta pseudohyphae and yeast | Budding yeast + pseudohyphae; germ tubes in tissue |
| Cryptococcus neoformans | Magenta yeast with clear capsule halo | Narrow-based budding; capsule unstained (clear halo) |
| Histoplasma capsulatum | Small magenta intracellular yeast | 2–4 μm; within macrophages; narrow-based budding |
| Blastomyces dermatitidis | Large magenta yeast | 8–15 μm; broad-based single budding; thick wall |
| Coccidioides immitis | Magenta spherules with endospores | Large 20–60 μm spherules; endospores inside |
| Pneumocystis jirovecii | Weakly PAS-positive cysts | Oval cysts 4–6 μm; TBO or GMS more reliable |
PAS vs GMS for fungal detection — which to choose:
| Feature | PAS | GMS (Gomori Methenamine Silver) |
|---|---|---|
| Fungal staining colour | Magenta/pink | Black |
| Background | Blue/green (coloured) | Green (pale) |
| Contrast | Good | Excellent — black on pale background |
| Also stains | Glycogen, mucin, basement membranes | Fungal walls only (more specific) |
| Procedural complexity | Moderate | More complex (longer) |
| Best for | General overview; glycogen co-identification | Specific fungal detection; paucifungal specimens |
| Pathologist's choice | Both often requested together | Gold standard for difficult fungal cases |
Clinical context: In immunocompromised patients with suspected invasive fungal infection, both PAS and GMS are usually requested on tissue biopsy. PAS provides morphological context (surrounding tissue reaction, background architecture); GMS provides maximum sensitivity for fungal elements. A negative PAS does not exclude fungal infection if GMS was not also performed.
PAS Staining for Whipple's Disease
Whipple's disease, caused by the gram-positive actinobacterium Tropheryma whipplei, is one of the most famous diagnostic applications of PAS staining in the history of medicine. When George Hoyt Whipple first described the disease in 1907, he noted the characteristic foamy macrophages in the intestinal mucosa — later identified as macrophages stuffed with bacterial remnants that stain intensely PAS-positive.
Why the macrophages are PAS-positive: T. whipplei has a gram-positive cell wall rich in polysaccharides. When macrophages engulf the bacteria — but fail to destroy them (due to an impaired immune response) — the intracellular bacterial material accumulates in lysosomes. This glycoprotein-rich material reacts strongly with the PAS stain, producing the characteristic bright magenta foamy macrophages.
Diagnostic appearance:
- Lamina propria of small intestine packed with foamy PAS-positive macrophages
- Individual macrophages appear enlarged and granular/foamy under low power
- High power: magenta-staining granules within macrophage cytoplasm
- Villous architecture may be distorted or flattened
Clinical presentation to recognise: The classic triad of diarrhoea + weight loss + arthralgia in a middle-aged man. The arthralgia often precedes GI symptoms by years, leading to misdiagnosis as seronegative arthritis. CNS involvement (cognitive decline, supranuclear ophthalmoplegia) can occur in untreated disease.
Diagnosis:
- Intestinal biopsy with PAS staining is the primary diagnostic method
- PCR for T. whipplei DNA in tissue, blood, or CSF confirms diagnosis
- PAS-positive macrophages are pathognomonic — no other condition produces this pattern in the small intestinal lamina propria
Treatment: Prolonged antibiotic therapy — typically IV ceftriaxone for 2 weeks followed by oral trimethoprim-sulfamethoxazole for at least 1 year. Relapse is common if treatment is stopped early.
Modified PAS: PAS with Diastase (PAS-D)
A useful modification for distinguishing glycogen from other PAS-positive substances. Diastase (amylase) digests glycogen before PAS staining. If the magenta staining disappears after diastase treatment, the structure contained glycogen. If it persists, it is not glycogen (could be mucin, fungal cell wall, basement membrane).
When PAS-D is clinically useful:
- Distinguishing glycogen accumulation (glycogen storage disease) from mucin-producing tumours
- Confirming glycogen in hepatocytes vs other PAS-positive material
- Not typically used for fungal detection (fungal cell walls are diastase-resistant)
Other Applications of Periodic Acid-Schiff (PAS) Staining
- The periodic acid-Schiff (PAS) staining is used to detect glycogen deposits in the liver. This test is useful when a person is suspected of the glycogen storage disease.
Glycogen storage disease (GSD) is a genetic disease in which the body cannot produce enzymes to break the complex sugar glycogen into simpler forms. It affects the different parts of the body like the liver, muscles etc.
- It demonstrates the glycogen granules in the bladder, kidney, ovary, pancreas, and lung tumors.
- It is used to visualize the basement membrane present in the various tissues in the body. Likewise, PAS demonstrates the thickness of the glomerular basement membrane for detecting abnormality in renal tissues.
- PAS stain is used in the diagnosis of glandular carcinomas (adenocarcinoma).
- PAS staining detects the neutral mucins in the gastrointestinal tract and some epithelial mucins.
- PAS can be used to study the amorphous or granular globules of the pulmonary alveolar proteinosis.
Pulmonary alveolar proteinosis is a rare disorder which causes the air sacs in the lungs to become clogged with surfactant.
- PAS is used to study the skin’s eosinophilic globoid bodies or Kamino bodies.
How to Remember: PAS Staining
"PAS stains things with SUGAR in them — magenta marks the sweet stuff":
- Fungal cell walls (chitin + glucan = polysaccharides) → magenta
- Glycogen (sugar polymer) → magenta
- Mucin (glycoprotein) → magenta
- Whipple's macrophages (bacterial polysaccharides inside) → magenta
The Whipple's clinical hook: Diarrhoea + weight loss + arthralgia = biopsy + PAS. The foamy PAS-positive macrophages in the intestinal lamina propria are pathognomonic — you see it once and never forget it.
PAS vs GMS — "PAS for the picture, GMS for the fungi": PAS shows the full tissue picture with fungi staining magenta. GMS is specific — black fungi on a pale background, maximises contrast when you're hunting for sparse fungal elements.
Key Exam Facts in One Table
| Feature | Detail |
|---|---|
| Full name | Periodic Acid-Schiff staining |
| Principle | Periodic acid oxidises vicinal diols → aldehydes → react with Schiff reagent → magenta |
| PAS-positive colour | Magenta/purple-red |
| Counterstain colour | Blue (haematoxylin) or green (light green) |
| Fungi appearance | Magenta cell walls and hyphae |
| Whipple's disease appearance | Foamy PAS-positive macrophages in intestinal lamina propria |
| Glycogen | Magenta; digested by diastase (PAS-D = negative after diastase = glycogen) |
| Mucin | PAS-positive; diastase-resistant |
| Best clinical microbiology uses | Invasive fungal infection in tissue; Whipple's disease; glycogen storage disease |
| GMS comparison | GMS more specific for fungi (black staining); PAS shows context |
| Pneumocystis | Weakly PAS-positive; TBO or GMS preferred |
| Limitations | Does not stain bacteria; requires tissue biopsy; histopathology technique |
References
- (IHC World, 2011)IHC World. (2011). PAS (Periodic Acid Schiff) Staining Protocol. IHC World. http://www.ihcworld.com/\_protocols/special_stains/pas.htm
- Stain, Periodic Acid Schiff Test – Test Results, Normal Range, Cost And More. Lybrate. (2022). Retrieved 21 June 2022, from https://www.lybrate.com/lab-test/stain-periodic-acid-schiff.
- (2022). Retrieved 21 June 2022, from https://www.labce.com/spg949466_periodic_acid_schiff_pas_diagnostic_applications.aspx.
- Murray PR, Rosenthal KS, Pfaller MA. Medical Microbiology. 9th ed. Elsevier; 2020.
- Larone DH. Larone's Medically Important Fungi: A Guide to Identification. 6th ed. ASM Press; 2018.
- Dobbins WO. Whipple's Disease. Springfield, IL: Charles C. Thomas; 1987.
- Fenollar F, Puéchal X, Raoult D. Whipple's disease. N Engl J Med. 2007;356(1):55–66. https://doi.org/10.1056/NEJMra062477

Tankeshwar Acharya, MSc (Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.