Hospital and Laboratory Waste Management: Classification, Segregation, Treatment, and Disposal
A complete guide to hospital and laboratory waste management — WHO classification into 9 types, colour-coded segregation, treatment methods (autoclave, incineration, chemical), laboratory-specific waste streams, sharps safety, needlestick injury protocol, and disposal.
In 2014, during the West Africa Ebola outbreak, a healthcare worker in Sierra Leone was infected after improperly discarded personal protective equipment contaminated their skin during removal. The waste was not from a patient contact — it was from the disposal process itself.
Hospital and laboratory waste carries biological, chemical, radioactive, and physical hazards that do not disappear when they leave the patient or the bench. Approximately 15–25% of healthcare waste is considered hazardous — capable of causing infection, chemical burns, radiation injury, or physical harm. When improperly managed, it creates risks for healthcare workers, waste handlers, the surrounding community, and the environment.
For a microbiologist, a medical officer, a public health professional, or a hospital infection control team member, waste management is not peripheral to clinical work — it is part of it. This article provides a comprehensive framework for hospital and laboratory waste management based on WHO guidelines applicable across all healthcare settings, from high-resource hospitals to district-level facilities.
Hospital and laboratory waste management is becoming a significant problem in most countries of the world. Due to its infectious and toxic nature, the waste bears numerous health and safety hazards. Health care activities, like diagnosing, treating, and immunizing humans or animals or while conducting research produce hospital waste. Likewise, the waste generated from industry laboratories, educational institutes, hospitals, and laboratories is laboratory waste.
As K. Park states in his landmark Textbook of Preventive and Social Medicine: "Let the waste of the 'sick' not contaminate the lives of 'the healthy'" — a principle that defines the entire purpose of healthcare waste management. (Park K. Park's Textbook of Preventive and Social Medicine. 26th ed. Jabalpur: Bhanot Publishers; 2021.)
The Scale of the Problem
Global burden:
- A typical hospital in a low- or middle-income country generates 0.5–3.0 kg of waste per bed per day
- Of this, approximately 75–90% is non-hazardous (equivalent to municipal waste)
- 10–25% is hazardous — infectious, chemical, radioactive, or sharps
- WHO estimates that in 2000, approximately 21 million hepatitis B infections, 2 million hepatitis C infections, and 260,000 HIV infections resulted globally from unsafe injection practices, most involving reuse of syringes and needles — a waste management and sharps safety failure
In low- and middle-income countries (LMICs), specific challenges include:
- Inadequate segregation infrastructure (shared bins, no colour-coded system)
- Unreliable electricity supply affecting autoclave function
- Limited access to properly maintained incinerators
- Open dumping or burning — releasing dioxins, furans, and heavy metals
- Insufficient training of waste handlers
- Weak regulatory enforcement
Why microbiology laboratories are high-risk: Microbiology laboratories generate waste that is disproportionately hazardous relative to its volume. Every culture plate, every broth tube, every used swab, every pipette tip that has contacted a specimen is potentially infectious. Unlike clinical waste from wards (which is often contaminated with small quantities of organisms from patients), laboratory waste may contain high concentrations of a single pathogen deliberately grown to detectable levels — making proper decontamination before disposal essential, not optional.
Sources of waste
The following things generates hospital and laboratory waste:
- Government and private hospitals
- Nursing homes and clinics
- Laboratories of different educational institutes and industries
- Primary health care centers
- Blood bank and collection center
- Mortuaries
- Medical research and training center, etc.
Category of waste
Hospital and laboratory wastes can be broadly classified into three groups:
- Non-hazardous waste covers 80% or more of total waste and includes general office/ kitchen waste.
- Infectious waste covers 10-15% of total waste, including sharp objects and anything contaminated with blood, bodily fluids, or body parts.
- Non- infectious but hazardous waste covers 5% of total waste, including X-ray film developer, chemical dyes, pharmaceutical, toxic, and nuclear waste, batteries, used oils, spent solvents, or mercury items.
The municipality or public authority manages the non-hazardous waste, whereas hospitals and laboratories manage infectious and hazardous waste.
WHO has classified hospital waste in to nine types, based on which waste is segregated into either recycling or incineration.
- General waste: no risk to human health. E.g. Office paper, wrappers, general sweeping wastes, etc.
- Pathological waste: human tissue or fluid. E.g. Body fluid, body tissue, body parts.
- Sharps: sharp waste items. E.g. needles, scalpels, knives, etc.
- Infectious waste: can transfer bacterial, viral, or parasitic diseases. E.g. laboratory waste, used cotton or gauze, tissue swabs, bandages, suture materials, etc.
- Chemical waste: chemicals used in treatment or diagnosis, e.g. laboratory reagents, disinfectants, X-ray film developer, etc.
- Radioactive waste: unused liquid from radiotherapy or lab research, contaminated glassware, etc.
- Pharmaceutical: expired or outdated drugs
- Pressurized container: gas cylinder, aerosol cans, etc.
- Genotoxic waste: waste containing cytotoxic drugs used in cancer therapy
As per CDC, Atlanta under US classification, Pathological and Sharp waste also belong to ‘INFECTIOUS WASTE’.
The types and nature of hospital waste depend upon the service available in the hospital and the nature of the hospital.
WHO Recommended Colour-Coded Segregation System
WHO recommends colour-coded segregation at the point of waste generation. While specific colour assignments vary between countries, the following system is widely adopted and recommended in WHO guidelines:
| Container colour | Waste type | Contents | Treatment/Disposal |
|---|---|---|---|
| Yellow (with biohazard symbol) | Infectious and pathological waste | Anatomical waste, cultures, blood-soaked materials, patient contact waste, isolation waste | Incineration (preferred) or autoclave then landfill |
| Red (with biohazard symbol) | Highly infectious waste | Microbiological laboratory waste with BSL-2/3 organisms, blood bags, body fluids | Incineration or high-temperature autoclave |
| White/Translucent (with biohazard symbol, puncture-proof) | Sharps | Needles, syringes, lancets, scalpels, broken glass | Sharps container; encapsulation or incineration |
| Blue/White | Pharmaceutical waste | Expired or unused medications, cytotoxic drugs | Return to pharmacy; incineration; never crush and flush |
| Black | General non-hazardous waste | Office paper, packaging, food waste, general sweeping | Municipal waste collection |
| Brown | Chemical waste | Laboratory reagents, disinfectants, X-ray developer | Licensed chemical waste disposal contractor |
| Lead-lined | Radioactive waste | Radioactive materials, contaminated items | Decay in storage; licensed radioactive waste disposal |
Important note on country-specific variation: The colour codes above follow WHO recommendations but are not universally standardised. India, the UK, USA, Australia, and other countries have their own national systems that may differ. Always verify the specific colour-coding system in use in your country and institution. The critical principle is universal: segregate at the point of generation, using clearly labelled containers with internationally recognised symbols (biohazard, cytotoxic, radioactive).
Minimum requirement in any setting: Even where a full colour-coded system is not possible, at minimum maintain three streams: (1) sharps in a puncture-proof container, (2) infectious/pathological waste separate from (3) general waste. This minimum segregation prevents the most dangerous mixing — sharps in general waste bags and infectious waste in municipal streams.
Laboratory-Specific Waste Management
Microbiology and clinical chemistry laboratories generate distinct waste streams that require specific management protocols beyond general hospital waste guidance.
Microbiological Waste Streams
| Waste type | Examples | Required treatment before disposal |
|---|---|---|
| Cultures and stocks | Agar plates, broth cultures, stocks of known pathogens | Autoclave at 121°C for 30–60 minvin (not 15 min — lab volumes require longer) before discarding; place in biohazard bag after autoclaving |
| Liquid infectious waste | Used broth, contaminated liquid media, discarded specimens | Add sodium hypochlorite (bleach) to 1% final concentration; allow 30 min contact time; then dispose to drain if no gross particulate matter |
| Sharps from laboratory | Lancets, broken glass slides, Pasteur pipettes, capillary tubes, broken culture vessels | Never discard in general waste — use puncture-proof sharps container regardless of size |
| Solid non-sharp infectious waste | Used swabs, contaminated gloves, wipes, packaging that contacted specimens | Yellow biohazard bag; autoclave or incinerate |
| Chemical waste | Formalin, phenol, xylene, stains (crystal violet, safranin), acid-alcohol | Chemical waste container; never mix chemical categories; never pour concentrated chemicals down drain |
| Used reagents and kits | Expired reagents, used ELISA kits, rapid test kits | Check Safety Data Sheet (SDS) for each; many require chemical waste disposal |
| Radioactive waste (nuclear medicine, research labs) | ³²P, ¹²⁵I-labelled materials | Store in lead-lined container until decay; document and follow radiation protection authority guidelines |
Decontamination Before Disposal — The Critical Step
Decontamination must occur before any microbiological waste leaves the laboratory. This is the single most important laboratory-specific waste management principle.
Decontamination options for laboratory waste:
1. Autoclaving (preferred for solid infectious waste):
- Use a gravity or pre-vacuum autoclave at 121°C
- Time: 30–60 minutes for laboratory waste (not the 15-minute cycle used for media preparation — laboratory waste containers are denser and require longer heat penetration)
- Use autoclave indicator tape on every load — external tape confirms temperature exposure; biological indicators (Geobacillus stearothermophilus spore strips) should be used weekly to verify sterilization efficacy
- Bag waste in autoclave-safe biohazard bags before loading — standard plastic bags melt; purpose-designed polypropylene autoclave bags are required
- After autoclaving: biohazard bags turn grey/black (colour indicator); waste can now be disposed of as general waste in most regulatory frameworks
2. Chemical disinfection (preferred for liquid infectious waste):
- Sodium hypochlorite (bleach): 10,000 ppm (1% available chlorine) for blood, high-risk body fluids, and cultures of known pathogens; 1,000 ppm (0.1%) for general infectious liquid waste
- Contact time: minimum 30 minutes
- Prepare fresh daily — hypochlorite degrades rapidly, especially in sunlight
- Do NOT use on acid, ammonia-containing waste, or urine without checking compatibility first (chlorine gas may be released)
- Glutaraldehyde (2%): effective for instruments and surfaces; longer contact time (20–30 minutes); skin/respiratory irritant — use in well-ventilated area
- Formaldehyde: effective broad-spectrum disinfectant; carcinogenic — avoid where alternatives exist
3. Incineration:
- Required for pathological waste (tissues, body parts), cytotoxic waste, and certain chemical waste
- Not all laboratories have access to properly functioning incinerators
- In resource-limited settings where incineration is unavailable: double-bag in yellow biohazard bags, label clearly, and store in a secure designated area until collection by a licensed healthcare waste contractor or until transport to a functioning facility is possible
Biosafety Level Considerations
The required level of decontamination depends on the biosafety classification of organisms worked with:
| BSL Level | Representative organisms | Minimum decontamination before disposal |
|---|---|---|
| BSL-1 | Non-pathogenic E. coli, Bacillus subtilis | Autoclave or chemical disinfection |
| BSL-2 | Most clinical pathogens (S. aureus, E. coli O157, M. tuberculosis in routine labs, Salmonella, HIV, HBV) | Autoclave (121°C, 60 min); incinerate sharps; no liquid cultures down drain without disinfection |
| BSL-3 | M. tuberculosis (concentrated cultures), Brucella, Coxiella, arboviruses | All waste autoclaved before leaving the laboratory; double-bag; incineration preferred; documented decontamination record |
| BSL-4 | Ebola, Marburg, Lassa | All waste autoclaved within the facility before any movement; specialist disposal |
For most clinical microbiology laboratories (BSL-2 work): The non-negotiable rule is that no undecontaminated biological waste leaves the laboratory. Every culture plate, every used swab, every specimen container that has been opened must be autoclaved or chemically disinfected before disposal.
Sharps Safety and Needlestick Injury Management
Sharps injuries are the leading cause of occupational bloodborne pathogen transmission in healthcare settings. WHO estimates that 2 million needlestick injuries occur annually among healthcare workers worldwide, with the majority in LMICs where safety-engineered devices are less available.
Prevention: The Four Rules of Sharps Safety
1. Never recap needles by two-handed technique. Recapping is the most common cause of needlestick injury. If recapping is necessary (e.g., during a procedure), use the one-handed scoop technique or a needle recapping device. Never reach for a needle with your other hand.
2. Dispose of sharps immediately at the point of use. Sharps containers must be within arm's reach of every procedure location. Walking across a room with an exposed needle, or setting down an exposed needle to dispose of later, dramatically increases injury risk.
3. Never overfill sharps containers. Fill only to the indicated three-quarter (¾) mark. Seal and replace. Attempting to push items into an overfull container is a primary cause of injury.
4. Never remove sharps from a container once deposited. Sharps containers are one-way. Never attempt to retrieve a dropped item. Never compress contents.
Sharps Container Disposal
| Setting | Method |
|---|---|
| High-resource hospital | Sealed containers collected by licensed medical waste contractor; incinerated or encapsulated |
| Resource-limited setting (no contractor) | Encapsulation — fill ¾ full, add cement/sand/plaster to immobilise sharps, seal, bury in secure pit |
| Field or outbreak setting | Needle destroyers (electric or manual) destroy needle at point of use; hub collected separately |
Post-Exposure Protocol: What To Do After a Needlestick Injury
This is the most important practical guidance for any healthcare worker. Every staff member should know these steps before they need them.
Immediate first aid (within seconds):
- Do not panic — remove the sharp carefully
- Encourage bleeding by gentle pressure — do not squeeze vigorously or suck the wound
- Wash immediately and thoroughly with soap and running water for at least 2 minutes
- Apply antiseptic (70% alcohol or iodine) after washing
- Do not apply caustic agents or inject antiseptics into the wound
Report immediately (within minutes to hours):
- Report to the designated occupational health officer, infection control team, or supervisor immediately — do not delay
- Document: time, date, type of sharp, body part injured, depth of injury, source patient (if known)
- The source patient's blood should be tested (with consent) for HIV, HBV, HBsAg, and HCV
- Baseline blood sample from the injured worker should be taken and stored
Post-exposure prophylaxis (PEP) — the time-critical step:
| Pathogen | PEP available? | Timing | Duration |
|---|---|---|---|
| HIV | Yes — antiretroviral PEP | Must start within 72 hours; ideally within 2 hours | 28 days of 3-drug ART regimen |
| HBV | Yes — HBIG + HBV vaccine (if unvaccinated or non-responder) | Within 24 hours; ideally within 12 hours | Single HBIG dose; complete vaccine series |
| HCV | No PEP available | Monitor with PCR at 4–6 weeks post-exposure | If infection confirmed, refer for early antiviral treatment |
The most important message: HIV PEP is effective but time-critical. Every hour of delay reduces efficacy. Every institution that handles blood and body fluids must have a clear PEP protocol with 24-hour access to antiretroviral medications. If your facility does not have this in place, establishing it is a priority for the infection control team.
Follow-up testing:
- HIV: test at baseline, 6 weeks, 3 months, and 6 months post-exposure
- HBV: test at 3 months if HBsAg positive source; check HBsAb 1–2 months after vaccine completion
- HCV: HCV RNA at 4–6 weeks; anti-HCV at 6 months
Spill Management in the Microbiology Laboratory
Spills of infectious material require immediate, systematic decontamination. Every microbiology laboratory must have a written spill management protocol and the materials readily available.
Small spill (culture tube, petri dish — no aerosol generated):
- Alert colleagues; avoid the area immediately around the spill
- Put on gloves, lab coat, and eye protection
- Cover spill with paper towels or absorbent material
- Apply disinfectant (10,000 ppm hypochlorite) to the outside of the paper towels first, then work inward
- Allow 30 minutes contact time
- Remove paper towels into biohazard waste bag; wipe area with fresh disinfectant
- Remove PPE and wash hands
Large spill or spill in biosafety cabinet:
- If aerosols may have been generated, evacuate the room immediately; close the door; allow 30 minutes for aerosols to settle before re-entering
- If in BSC, keep the cabinet running; do not open the sash; allow 5–10 minutes, then decontaminate within the cabinet using the procedure above
- Report to supervisor; document in the incident log
Spill of hazardous chemicals:
- Never use water on chemical fires or concentrated acid/alkali spills — check the Safety Data Sheet (SDS) first
- Use appropriate neutralising agent (sodium bicarbonate for acids, boric acid for alkalis)
- Strong oxidising agents (perchloric acid, concentrated nitric acid) require specialist response — do not attempt to manage alone
Protecting Waste Handlers: The Often-Forgotten Risk Group
Healthcare waste handlers — the workers who collect, transport, and dispose of hospital waste — are at significant occupational risk yet are frequently overlooked in institutional safety programmes.
Key protective measures:
- PPE for waste handlers: Heavy-duty puncture-resistant gloves (not clinical examination gloves), closed-toe boots, fluid-resistant apron, and eye protection during bag sealing and transport. Face mask when handling infectious waste with potential aerosol.
- Vaccination: All waste handlers who contact potentially infectious waste should receive HBV vaccine series, confirmed with post-vaccination anti-HBs testing. Tetanus vaccination should also be current.
- Training: Annual training on waste categories, segregation, safe handling, what to do if a bag breaks or a sharp is encountered unexpectedly, and the post-exposure protocol.
- Incident reporting: A no-blame incident reporting system that waste handlers can access. Many needlestick injuries in waste handlers go unreported because of fear of consequences. Anonymous reporting and guaranteed access to PEP encourages reporting.
- Bag integrity: Infectious waste bags should never be more than ¾ full, should be tied securely with a single knot, and should never be compacted or manually pushed down.
Hospital and Laboratory Waste Management (Tips and Steps)
A waste management system is a systematic collection, sorting, storing, transporting, and disposal of waste produced by an organization. A significant idea to the success of the system is waste minimization. Hospital and laboratory personnel should be encouraged to generate less waste.
Some tips on How to Manage Waste
- Implement the principle of 3R; Reduce, Reuse and Recycle.
- Keep devices up to date.
- Try to avoid purchasing chemicals in bulk quantities
- Recycle and reuse as many materials as possible. Chemical agents like xylene, formalin, and ethyl alcohol can be distilled, filtered, or recycled.
- Reduce the size and number of containers if not used.
- Store all hazardous waste in the appropriate storage container with proper labeling.
- Regularly train employees in safety procedures because only verbal briefing is not sufficient. Give training for adding waste to and removing from storage containers and types of hazardous and infectious wastes.
Steps of Waste Management
Waste Segregation
The nature of hospital and laboratory waste determines how it will be managed. Therefore, the first step of waste management is the segregation of waste.
Waste segregation is implemented at the point of generation of waste. Different types of waste are kept in separate color-coded and well-labeled bags or containers. Color codes for different types of waste are different country-wise. However, the use of red, yellow, white, blue, and back bins is common. Labeling each bin with symbols, like, as the symbol of biohazard and cytotoxicity is necessary. Regular cleaning and disinfection of the garbage bin are very important.
The nature of waste in different bins is shown in the figure.
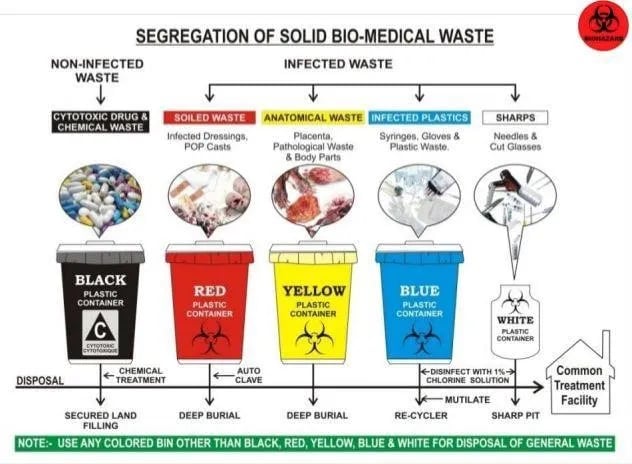 Figure: Image source:https://www.juniordentist.com/management-and-handling-of-dental-hospital-waste-color-coding-for-waste-disposal.html
Figure: Image source:https://www.juniordentist.com/management-and-handling-of-dental-hospital-waste-color-coding-for-waste-disposal.html
Storage and Transportation of Waste
Waste should not be stored for a more extended period in the generation area. It should be transported in a sealed container for treatment and disposal.
Waste Treatment
Chemical Treatment
Chemical treatment applies to all types of waste except body parts and body fluids. Users should wear protective clothes, gloves and goggles while working with chemicals. Chemicals used in disinfection can vary according to the type of waste; some examples are bleach, sodium hypochlorite, chlorine, etc.
Microwave irradiation
It is effective for all except large metals and body parts. A frequency of 2450 MHz with a wavelength of 12.24 cm destroys most microbes. The water of the waste heats, which eliminates the infectious component.
Autoclaving
It is applied to sterilize dressings, gloves, syringes, specific instruments, discarded culture plates, and culture media. Plastics and sharp instruments should not be included in autoclaves. A temperature of 121°C under 15 lb/square inch pressure is effective enough for sterilization.
Encapsulation
It is recommended for the safe disposal of sharp objects. The waste is collected in a puncture-proof container. After it becomes a three-quarter full mortar, material like cement, plastic foam, or clay is poured. After it gets dry, it is disposed of.
Incineration
Incineration is applied only for most hazardous waste that cannot be reused or recycled or can’t be disposed of at the landfill site. An incinerator’s high temperature and dry oxidation process reduce organic, combustible waste to inorganic waste in reduced volume and weight. Finally, ash is generated and disposed of in the sanitary landfill.
Waste that can’t be incinerated is:
- Pressurized containers
- Halogenated plastics
- Waste with high content of heavy metals
- Radioactive waste
Types of Incinerator
- Single-chambered incinerator
Here, the waste is burnt at 300-400°C. This type of incinerator may not achieve proper sterilization due to low temperature.
- Double-chambered incinerator
In this type of incinerator, the waste is burnt in the primary chamber at 800°C, whereas volatile gas is in the second chamber at 1000°C +/- 50°C.
- Pyrolytic Incinerator
The anaerobic combination is conducted in doubled chambered pyrolytic incinerator at 900-1200°C. Waste transforms into combustible liquid and gases, which can be used as fuel for pyrolysis. It reduces operating costs. Compared to the common incinerators, pyrolytic incineration has a high energy recovery rate, less pollution, and is cost-effective.
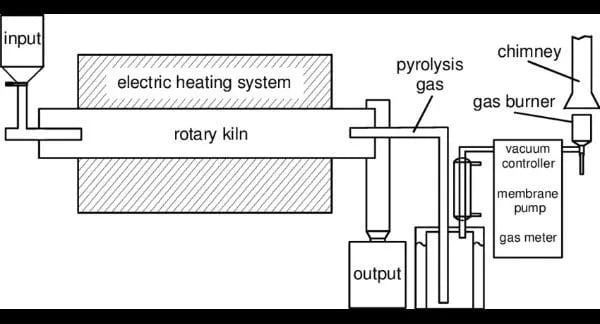 Figure: Figure: Pyrolysis of the waste using Rotary KilnFigure source:https://www.researchgate.net/figure/Scheme-of-the-laboratory-rotary-kiln-system_fig2_267992380
Figure: Figure: Pyrolysis of the waste using Rotary KilnFigure source:https://www.researchgate.net/figure/Scheme-of-the-laboratory-rotary-kiln-system_fig2_267992380
Incineration has certain disadvantages, like, emitting toxic gases, carcinogens, and toxins like dioxins, furans, and mercury. Fabric filters are fitted in the chimneys of the incinerator chamber to minimize such emissions.
Plasma technology
It is a new technique that uses a gas cloud generated by ionizing an inert gas. As a result, a high temperature, up to 3000°C, is produced, destroying pathogens in the waste. The final product is then disposed of in the landfill.
Though plasma technology is expensive to run, it has certain advantages such as:
- No harmful products are released
- The final volume is reduced
- Heat energy produced can be recycled to lower the operation cost.
However, hospital and laboratory waste is often incinerated or autoclaved.
Waste Disposal
After proper treatment of waste, it is now safe for its disposal.
Landfilling
Landfilling is the oldest technology, but still, several low-income countries rely on it. The main idea is decomposing waste into harmless substances through long-term storage. Unfortunately, the problem of infiltration arises; as a result, toxic, pathogenic, or radioactive materials have access to soil and water resources.
Open dumps should be avoided due to public health risks.
Sanitary landfill: Sanitary landfill with an anti-seepage system has been developed to overcome the harmful effects of a general landfill. It is covered with clay, high-density polyethene, a gas collection system and output pipelines. But, disinfection and reduction of waste are necessary before landfilling.
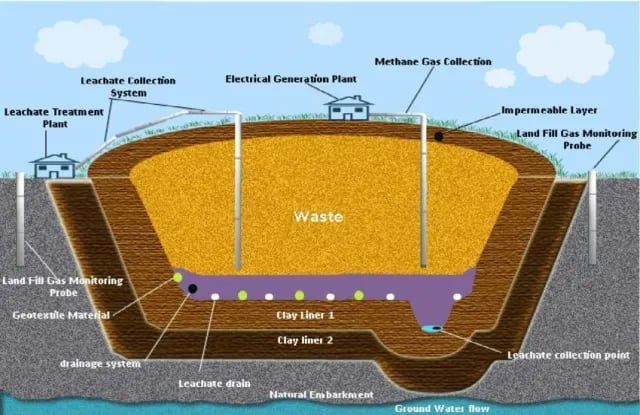 Figure: Figure: Modern Sanitary Landfill as a replacement of open dumping siteFigure source:https://www.researchgate.net/figure/A-modern-sanitary-landfill-designed-to-replace-Avu-and-Ihie-open-dumpsites_fig1_270762454
Figure: Figure: Modern Sanitary Landfill as a replacement of open dumping siteFigure source:https://www.researchgate.net/figure/A-modern-sanitary-landfill-designed-to-replace-Avu-and-Ihie-open-dumpsites_fig1_270762454
Liquid waste is disposed of in sewage drains
Proper waste management depends on good planning, funding, administration, and commitment at the policy level. If waste management is implemented correctly, it will benefit both individuals and the environment. Conversion technologies may apply to plastic or lignocellulose fraction, cotton, paper, etc., to convert them into fuel/material production, combining with the municipal waste.
It is wise for hospitals and laboratories to collaborate with local municipalities for waste management. Apart from state and local agencies, waste can also be governed by various international agencies.
Choosing a Treatment Method: Practical Decision Framework
| Waste type | Preferred treatment | Alternative (resource-limited) | Not suitable |
|---|---|---|---|
| Microbiological cultures and stocks | Autoclave (121°C, 60 min) | Chemical disinfection (10,000 ppm hypochlorite) | Open burning; general landfill |
| Pathological waste (tissue, body parts) | Incineration | Deep burial in lined pit (if no incinerator) | Autoclave; open dumping |
| Sharps (needles, lancets) | Incineration after containment | Encapsulation; needle destroyer | General waste bags; recapping |
| Pharmaceutical waste | Incineration; return to manufacturer | Encapsulation in concrete | Sewage; open burning |
| Chemical waste (laboratory reagents) | Licensed chemical disposal contractor | Neutralise where safe; controlled incineration | Drain (undiluted); open burning |
| Liquid infectious waste (broth, specimens) | Chemical disinfection + drain | Autoclave in sealed container | Untreated drain disposal |
| General non-infectious waste | Municipal collection | Municipal collection | No change needed |
| Cytotoxic/genotoxic waste | High-temperature incineration (>1000°C) | Return to pharmacy | Standard autoclave; landfill |
How to Remember
The waste management chain — every link matters:
Generate less → Segregate correctly → Store safely → Decontaminate before disposal → Dispose appropriately
Breaking any link in this chain creates a hazard. The most common failures are at segregation (mixing infectious with general waste) and decontamination (discarding cultures without autoclaving).
The three non-negotiable rules for any healthcare setting:
- Sharps in sharps containers, always. Never in general waste bags. Never recapped two-handed. Changed at ¾ full.
- Infectious waste decontaminated before disposal. Autoclaved or chemically disinfected. Never discarded as general waste.
- Know your post-exposure protocol before you need it. HIV PEP must start within 72 hours. Every minute of delay after a needlestick injury matters.
A practical memory framework — the waste hierarchy:
| Priority | Action | Why |
|---|---|---|
| 1st | Reduce | Less waste generated = less risk, less cost |
| 2nd | Reuse (where safe) | Autoclaved instruments, recyclable non-infectious materials |
| 3rd | Recycle | Paper, certain plastics — non-infectious only |
| 4th | Treat | Autoclave, incinerate, chemically disinfect |
| 5th | Dispose | Only after treatment; appropriate method for waste type |
The resource-limited setting minimum standard: When full compliance is not achievable, prioritise in this order:
- Sharps segregation and safe disposal (highest injury/infection risk)
- Decontamination of microbiological cultures before disposal
- Pathological waste separation from general waste
- Colour-coded segregation for remaining streams
References
- World Health Organization. (2014). Safe Management of Wastes from Health-Care Activities (2nd ed.). Geneva: WHO. https://apps.who.int/iris/handle/10665/85349
- World Health Organization. (2018). WHO Best Practices for Injections and Related Procedures Toolkit. Geneva: WHO.
- Park, K. (2021). Park's Textbook of Preventive and Social Medicine (26th ed.). Jabalpur: Bhanot Publishers.
- Centers for Disease Control and Prevention (CDC). (2019). Workbook for Designing, Implementing, and Evaluating a Sharps Injury Prevention Program. Atlanta: CDC. https://www.cdc.gov/niosh/topics/bbp/sharps.html
- Prüss-Üstün, A., Rapiti, E., & Hutin, Y. (2005). Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers. American Journal of Industrial Medicine, 48(6), 482–490.
- Windfeld, E. S., & Brooks, M. S. L. (2015). Medical waste management — a review. Journal of Environmental Management, 163, 98–108. https://doi.org/10.1016/j.jenvman.2015.08.013
- Mathur, P., Patan, S., & Shobhawat, S. (2012). Need of biomedical waste management system in hospitals — an emerging issue — a review. Current World Environment, 7(1), 117–124.

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.