Hepatitis C Virus: How It Evades Immunity and Why Treatment Changed
Why HCV's hypervariable proteins defeat both the immune system and interferon, and how direct-acting antivirals changed hepatitis C treatment.
A man in his fifties is found to have abnormal liver enzymes during a routine checkup. He has no symptoms, no history of jaundice, nothing that would have prompted him to seek care. Questioning eventually reveals a blood transfusion received decades earlier, before reliable screening existed. He has been carrying hepatitis C, silently, for thirty years, and is now found to have early cirrhosis.
This story is common with HCV specifically because the virus is built to be invisible to the immune system for decades. Its two envelope proteins, E1 and E2, sit inside hypervariable regions of the genome, regions that mutate rapidly even within a single infected person. Every time the immune system raises antibodies against one viral variant, slightly mutated versions are already circulating that those antibodies don't recognize well. The virus isn't dodging the immune response once, it's running a continuous, low-grade arms race inside a single host for years, which is exactly why most people never clear it on their own and why a vaccine has been so difficult to develop: there's no single, stable target to aim at.
This same evasion strategy explains something that used to confuse the Treatment section of articles like this one for years: HCV's NS5A protein actively interferes with the body's own interferon response, which is part of why interferon-based therapy, once the standard treatment, often failed or required long courses with severe side effects. Modern treatment doesn't try to out-compete the virus's interferon resistance at all anymore; it bypasses the problem entirely by directly blocking the viral proteins the virus depends on to replicate (covered in the Treatment section below). Understanding why the old approach struggled is what makes sense of why the field moved on from it.
Hepatitis C virus, an RNA virus, belongs to the hepacivirus genus of the family Flaviviridae. It is the most important cause of parenteral non-A, non-B hepatitis (NANBH). Most patients with hepatitis C infection develop chronic liver diseases, progressing into hepatocellular carcinoma and cirrhosis.
According to ICTV (international committee on taxonomy of viruses), hepatitis C has eight genotypes and 93 subtypes.
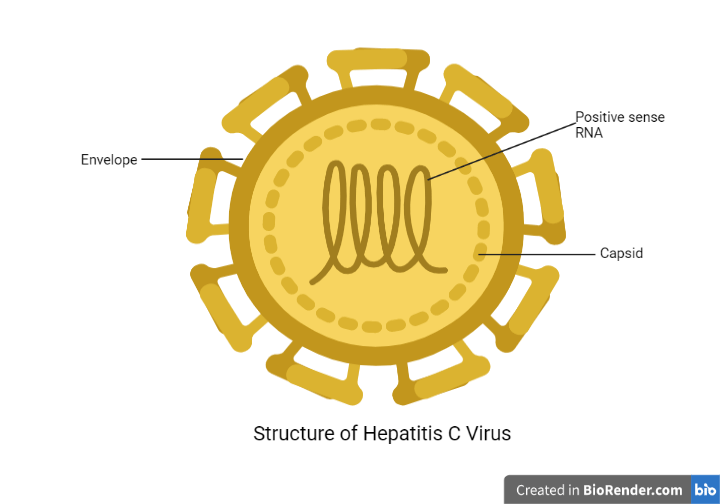 Figure: Structure of Hepatitis C virus
Figure: Structure of Hepatitis C virus
Structure of Hepatitis C
Hepatitis C belongs to the genus hepacivirus of the family Flaviviridae. It has a close resemblance to hepatitis D virus, yellow fever virus, and dengue virus. The general structure of the hepatitis C virus has the following features:
- It is a spherical, enveloped virus with a diameter of 55 nm (approximately).
- Positive sense, Single-stranded RNA of 9.6 kb is the genetic material of the virus.
- The genomic material encodes for ten structural and regulatory proteins.
- The structural proteins involve a core protein, and two envelop proteins (E1 and E2).
- The two envelop proteins undergo variation because of the hypervariable regions within the gene.
Genomic arrangement of Hepatitis C virus
- HCV has plus-strand single-stranded RNA of 9.6 kb.
- The genome has a long open reading frame (ORF) that encodes polyprotein precursors. The protein has 3010 amino acids.
- The HCV has a 341 nucleotides long 5′ untranslated region (UTR) located upstream of the ORF in the RNA. The 5′ UTR consists of 4 highly structured domains, I to IV.
- Domains II, III, and IV of 5′ UTR with the first 12 to 30 nucleotides of the core-coding region make up IRES (internal ribosome entry site).
- The IRES can directly bind to the ribosome and start the translation process.
- The virus produces polyprotein after translation cleaves during and after translation. Thus forming ten proteins; core proteins, envelope proteins (E1 and E2), and non-structural proteins (NS1 or p7, NS2, NS3, NS4A, NS4B, NS5A, and NS5B).
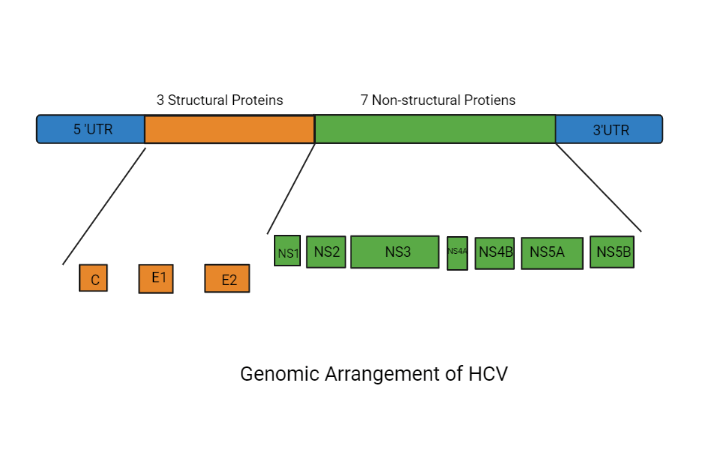 Figure: Genomic structure of HCV
Figure: Genomic structure of HCV
How to Remember
Hypervariable regions are a moving target, on purpose. E1 and E2's variability isn't sloppiness in the genome, it's a survival strategy. A useful anchor: think of the immune system as constantly photographing a suspect (the virus), but the suspect keeps changing disguises (E1/E2 mutations) faster than new photographs can be matched to old descriptions. This single idea explains chronic persistence, the difficulty of vaccine development, and why genotyping matters clinically (different genotypes can respond differently to treatment).
Why HCV resists interferon, in one sentence: NS5A jams the alarm system. Interferon works by triggering an antiviral state inside infected cells, essentially sounding a cellular alarm. NS5A specifically interferes with this signaling, which is why naturally-occurring interferon, and interferon-based drugs, often struggled to clear HCV even with prolonged treatment. This is the mechanistic reason the field moved toward direct-acting antivirals (DAAs) that don't rely on the interferon pathway at all, see the Treatment section below.
Three structural proteins, seven non-structural proteins, one long polyprotein. Rather than memorizing ten separate names, remember the shape of the strategy: HCV translates one giant polyprotein and then cuts it into pieces, the way you might bake one large sheet of dough and then slice it into ten cookies. The structural proteins (core, E1, E2) build the virus particle; the non-structural proteins (NS2 through NS5B) build the replication machinery and, not coincidentally, are exactly where modern DAAs (NS3, NS5A, and NS5B inhibitors) are designed to act.
Replication of Hepatitis C virus
The replication of the hepatitis C virus takes place in hepatocytes, and sometimes the replication may occur in monocytes, dendritic cells, and B and T lymphocytes. The steps involved in the replication are as follows:
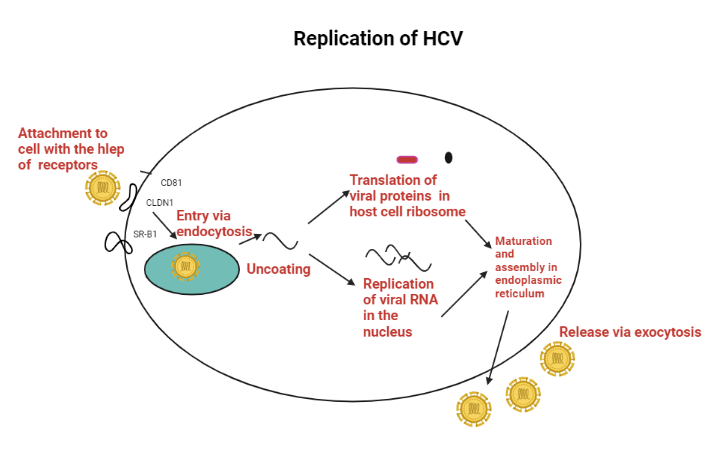 Figure: Replication of HCV
Figure: Replication of HCV
Attachment
While circulating in the bloodstream, the viral particles bind to lipoprotein. Viral cell surrounded by lipoprotein attaches to various cell receptors like CD81, SR-B1, LDL-R, EGFR, and EphA2.
Entry
After attachment, the entry of the viral particle is facilitated by clathrin-mediated endocytosis.
Uncoating
After the fusion with the cell membrane, the virus’s capsid breaks down by the mechanism triggered by the low pH of the endosome. The uncoating of the capsid releases the viral genome into the host cell cytoplasm.
Translation
The RNA translates a polyprotein precursor, cleaved into angle protein by the enzyme proteases. The translation occurs in RER (rough endoplasmic reticulum).
Replication
A replication complex is formed by non-structural and host proteins, which synthesize multiple copies of the HCV RNA genome with the help of a minus-strand RNA as a template.
Maturation and Assembly
The virus acquires E1 and E2 glycoprotein from the host cell’s ER (endoplasmic reticulum). The assembly also takes place in the ER. Lipoviral particle is formed as soon as the maturation and just before release.
Release
The release of the viral particles takes place by exocytosis. However, transmission to other cells takes place by a cell-free mechanism.
Pathogenesis of Hepatitis C
HCV is carried in the bloodstream of the infected person. Even though its natural target cells are hepatocytes, they can also target B lymphocytes. 50% of the hepatocytes may be infected during chronic hepatitis. Almost all the infected people develop persisting viremia, which is associated with a different degree of inflammation and fibrosis. Typical histopathological details in chronic hepatitis are portal inflammation, interphase hepatitis, and lobular necrosis.
Virulence factor
Hepatitis C has different factors which help the virus infect human hepatocytes and develop persistence. They are as follows:
- E2 glycoprotein initiates the attachment of the virus.
- E1 glycoprotein is thought to play a role in intra-cytoplasmic virus membrane fusion.
- It is challenging to produce vaccines against HCV because of its highly diverse but closely related genomic structures within an infected individual.
- NS5A non-structural protein produced by the HCV genome interferes with the cell's natural interferon signaling, which historically reduced the effectiveness of interferon-based therapy and contributed to the field's shift toward direct-acting antivirals that don't rely on the interferon pathway (see Treatment section below).
Transmission of Hepatitis C
Hepatitis C infection occurs only in humans. The transmission occurs from an infected person to a healthy individual in the following ways:
Parenteral transmission
Parenteral transmission of HCV infections occurs in the following ways:
- Blood transfusion was historically a major route of HCV transmission. With nucleic acid testing (NAT) now standard in well-resourced blood screening programs, residual transfusion risk has fallen substantially, though it still varies by country depending on the screening methods in use, an important consideration in settings where NAT-based screening is not yet universal.
- Needle sharing in intravenous drug users. It is the principal reason for parenteral transmission.
- Organ transplantation
Sexual Transmission
Approximately 20% of HCV infections are considered to be sexually transmitted. HIV coinfection is notably common among certain higher-risk groups, particularly people who inject drugs and certain sexual networks, though it is not accurate to say this applies to most sexually transmitted HCV cases broadly.
Incubation Period
The incubation period of HCV ranges from 2 weeks to 6 months. The average period is approximately eight weeks.
Symptoms
HCV is the causative agent of acute as well as chronic HCV infection. This lead to hepatitis-induced complications. The symptoms of hepatitis C infection are as follows:
Acute HCV infection
Most patients with acute infection are asymptomatic and do not progress to jaundice. The symptoms in those symptomatic patients are mild. The symptoms are as follows:
- Fever
- Fatigue
- Decreased appetite
- Nausea
- Vomiting
- Abdominal pain
- Dark urine
- Joint pain
- Less than 25% of symptomatic patients develop jaundice.
Chronic HCV infection
Most chronic cases are asymptomatic but can present non-specific symptoms like fatigue or malaise.
Further Complications
Cirrhosis and hepatocellular carcinoma are the further complications of HCV infections.
It takes up to 20 years for the infections to progress to cirrhosis. The progression occurs in approximately 20% of cases. Patients with cirrhosis risk developing secondary liver failure, portal hypertension, and other complications.
Hepatocellular carcinoma is another complication of HCV. It progresses after approximately 30 years of chronic HCV infection and cirrhosis. It occurs in 1-5% of people with cirrhosis.
Diagnosis of Hepatitis C Infection
Sample collection and transport
Blood serum is the sample of choice. Collect 15ml blood in a vial free of the anticoagulant. Transport the sample as soon as possible. Once you receive the sample, allow it to clot and centrifuge it. It results in the separation of serum from the blood.
In case of delay in transporting the sample, refrigerate it at 4℃.
Sample Processing
There are multiple ways of processing serum samples. The conventional method of laboratory diagnosis of diseases is the observation of viruses by electron microscopy and the culture of viruses. However, culturing and electron microscopic observation are suitable only for research purposes.
Thus, the most convenient way to diagnose HCV infection is antigen, antibody, and nucleic acid detection.
Antigen Detection
Detection of the core antigen of HCV is done by using ELISA (enzyme-linked immunosorbent assay) and CLIA (chemiluminescence immunoassay).
Antibody Detection
Antibodies against core, envelope, NS3 and NS4 proteins are seen in acute infection only after 6-8 weeks of initial infection and persist throughout life. RDT (rapid detection test kit) kit, ELISA, and EIA are used to detect antibodies. But recombinant immunoblot assay that uses recombinant HCV antigen is the most specific test for detection.
Nucleic Acid Detection/ Molecular Diagnosis
PCR (polymerase chain reaction) detects HCV nucleic acid (RNA) from the serum sample. It is the most specific test for diagnosing acute HCV infection because it detects the presence of the virus, corrects false-positive cases, and identifies the genotype.
Other Tests
Before starting antiviral therapy, performing a liver biopsy is recommended. However, it is not applicable for laboratory diagnosis.
Treatment, Prevention, and Control of Hepatitis C Infection
Treatment of symptoms is the only measure necessary during acute infection in most cases. For chronic infection, the current global standard of care is direct-acting antivirals (DAAs), oral medications that directly target the NS3/4A protease, NS5A protein, or NS5B polymerase needed for viral replication. DAA regimens (such as sofosbuvir-based combinations) achieve cure rates above 95%, with treatment courses typically lasting 8-12 weeks and far fewer side effects than older regimens.
PEGylated interferon plus ribavirin was the standard chronic treatment before DAAs became widely available, but it required much longer courses, achieved lower cure rates, and caused significant side effects, partly because of HCV's interferon-resistance mechanisms (see Virulence Factor section above). It is now considered legacy treatment, reserved for settings where DAAs remain inaccessible.
Vaccines are not available, and immunoglobulin does not help prevent transmission. Screening blood transfusions, organ transplants, and avoiding needle-sharing and unprotected sexual contact with HCV-positive individuals remain the primary ways to prevent infection.
Where Students Get Confused
"HCV is treated with interferon, full stop." This is now outdated, and the article's own structure used to reflect the confusion: it states elsewhere that NS5A makes the virus interferon-resistant, while still listing PEGylated interferon plus ribavirin as the standard chronic treatment. The modern reality is that direct-acting antivirals (DAAs) have replaced interferon-based therapy as the global standard of care, achieving cure rates above 95% with far fewer side effects and shorter treatment courses. Interferon-based regimens are now considered legacy treatment, used only where DAAs are unavailable.
"A positive anti-HCV antibody test confirms active infection." It doesn't, on its own. Antibodies persist for life even after the infection clears (spontaneously or with treatment), so a positive antibody test only confirms exposure at some point. Confirming active, current infection requires detecting HCV RNA by PCR, which is also the test that determines whether someone has actually cleared the virus after treatment.
"Since most chronic HCV is asymptomatic, it's a relatively mild infection." The absence of symptoms is exactly what makes HCV dangerous, not reassuring; silent, ongoing viral replication and inflammation over years to decades is what leads to cirrhosis and hepatocellular carcinoma, often diagnosed only once advanced liver disease is already present, as in the case in the clinical hook above.
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Family / Genus | Flaviviridae / Hepacivirus |
| Genome | Positive-sense, single-stranded RNA, ~9.6 kb |
| Envelope | Present; spherical, ~55 nm |
| Genotypes | 8 genotypes, ~93 subtypes (ICTV) |
| Key envelope proteins | E1, E2 (hypervariable regions drive immune escape) |
| Attachment receptors | CD81, SR-B1, LDL-R, EGFR, EphA2 |
| Interferon resistance mechanism | NS5A interferes with interferon signaling |
| Chronicity | Majority of infections become chronic |
| Average incubation period | ~8 weeks (range 2 weeks-6 months) |
| Time to cirrhosis | Up to ~20 years (in ~20% of chronic cases) |
| Time to hepatocellular carcinoma | ~30 years after chronic infection/cirrhosis (1-5% of cirrhotic patients) |
| Acute diagnostic marker | Anti-HCV antibodies (detectable after 6-8 weeks); HCV RNA by PCR detects infection earlier |
| Current standard treatment | Direct-acting antivirals (DAAs) — cure rates >95% |
| Vaccine availability | None |
References
- Bajpai, M., Gupta, E., & Choudhary, A. (2014). Diagnosis of Hepatitis C. Asian Journal of Transfusion Science, 8(1), 19–25. https://doi.org/10.4103/0973-6247.126685
- Chevaliez, S., & Pawlotsky, J. M. (2006). HCV genome and life cycle. In Hepatitis C Viruses: Genomes and Molecular Biology. Horizon Bioscience. https://www.ncbi.nlm.nih.gov/books/NBK1630/
- Dustin, L. B., Bartolini, B., Capobianchi, M. R., & Pistello, M. (2016). Hepatitis C virus: life cycle in cells, infection and host response, and analysis of molecular markers influencing the outcome of infection and response to therapy. Clinical Microbiology and Infection, 22(10), 826–832. https://doi.org/10.1016/j.cmi.2016.08.025
- Parija, S. C. (2012). Textbook of Microbiology and Immunology (2nd ed.). Elsevier.
- World Health Organization. (2024). Hepatitis C. WHO Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/hepatitis-c
Frequently Asked Questions
Is interferon still used to treat hepatitis C?
Why is there no vaccine for hepatitis C, when there is one for hepatitis B?
Can someone have hepatitis C for years without knowing it?
Does a positive hepatitis C antibody test mean someone currently has the infection?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.