Sickle Cell Anemia and Malaria: Protection, Risk, and the Evolutionary Paradox
Why does sickle cell trait protect against malaria while sickle cell anemia worsens it? Understand the HbAS advantage, the Duffy antigen, and other genetic factors — with exam-ready mnemonics.
In the malaria belt of sub-Saharan Africa, a geneticist once posed a puzzle that changed how we think about natural selection: why would a mutation that causes a deadly blood disorder persist in the population at such high frequency? The answer is malaria. Carrying one copy of the sickle gene — sickle cell trait (HbAS) — offers significant protection against dying from Plasmodium falciparum. But carrying two copies — sickle cell anemia (HbSS) — makes malaria more dangerous, not less. This is one of the most elegant examples of balancing selection in human biology, and it is a recurring exam favourite precisely because the answer is counterintuitive: the same gene protects and harms, depending on how many copies you carry.
What Is Sickle Cell Anaemia?
Sickle cell anemia is an autosomal recessive haemoglobinopathy caused by a point mutation in the beta-globin gene — a single nucleotide substitution (A→T) that replaces glutamic acid with valine at position 6 of the beta-globin chain. This produces haemoglobin S (HbS) instead of normal haemoglobin A (HbA).
Under low-oxygen conditions, HbS polymerises, distorting the RBC from its normal biconcave disc shape into a rigid crescent (sickle) shape. Sickled cells are:
- Inflexible — they obstruct capillaries, causing vaso-occlusive crises
- Fragile — they haemolyse prematurely, causing chronic haemolytic anemia
- Adhesive — they bind to endothelium, promoting thrombosis
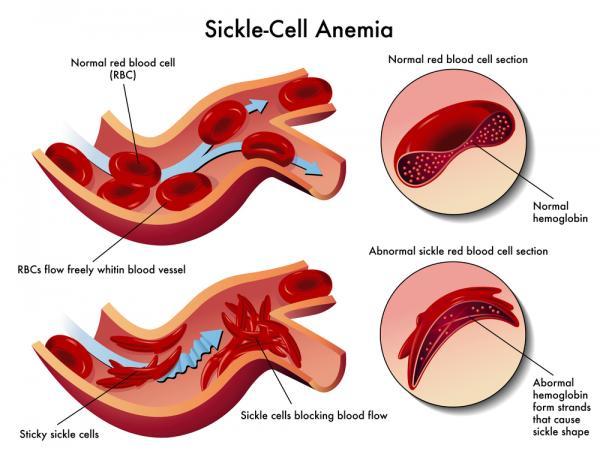 Figure: Sickle Cell Anemia
Figure: Sickle Cell Anemia
Three clinically important phenotypes:
| Genotype | Haemoglobin type | Clinical status |
|---|---|---|
| HbAA | Normal haemoglobin | Normal; no sickling |
| HbAS | Sickle cell trait | Carrier; usually asymptomatic; protected against severe malaria |
| HbSS | Sickle cell anemia | Full disease; chronic haemolysis, crises; worsened by malaria |
The Central Paradox: Does Sickle Cell Protect Against Malaria?
The answer students most commonly get wrong is a flat "yes." The correct answer is it depends on genotype.
HbAS (sickle cell trait) → Protection against severe malaria
Individuals with sickle cell trait carry one normal and one sickle beta-globin allele. They produce both HbA and HbS, do not develop sickle cell anemia, and lead clinically normal lives. However, HbAS confers substantial protection against severe and complicated P. falciparum malaria — particularly against cerebral malaria and severe malarial anemia. Field studies across multiple African populations have consistently shown that HbAS reduces the risk of severe malaria by approximately 90%.
HbSS (sickle cell anemia) → Increased risk and worse outcomes
Individuals with two copies of the sickle mutation have the full disease. They suffer from malaria and suffer badly. Malaria is one of the commonest triggers of sickle cell crisis in Africa — fever, dehydration, and acidosis all precipitate sickling. The same mutation that evolved because HbAS protects against malaria actively harms those with HbSS.
This is the exam trap: the protection is for the heterozygote, not the homozygote.
How Does HbAS Protect Against Malaria? (Postulated Mechanisms)
The precise mechanism remains incompletely understood — this is an active area of research. Several non-mutually exclusive mechanisms have been proposed:
1. Impaired parasite growth under low oxygen tension When P. falciparum begins replicating inside an HbAS erythrocyte, it consumes oxygen. As oxygen tension drops, the RBC begins to sickle. The sickled cell environment impairs parasite nutrition and growth. Additionally, the sickled cells are recognised and destroyed more rapidly by the spleen, eliminating the parasites before they complete erythrocytic schizogony.
2. Enhanced innate immunity HbAS erythrocytes show reduced expression of ICAM-1 and other cytoadherence receptors on their surface. This impairs the ability of P. falciparum-infected RBCs to sequester in deep capillaries — one of the key mechanisms of cerebral malaria. In essence, HbAS partially disrupts the PfEMP1-mediated cytoadherence that makes falciparum so deadly.
3. Enhanced acquired immunity Some evidence suggests HbAS individuals develop faster and more effective acquired immunity to malaria with repeated exposure, possibly because the slower parasite growth allows more time for immune priming.
4. Heme oxygenase-1 (HO-1) induction HbS haemolysis releases free haem, which induces HO-1 production. HO-1 has anti-inflammatory and cytoprotective effects that may reduce the severity of malaria-related inflammation without affecting parasite clearance.
Other Genetic Factors That Influence Malaria Susceptibility
Sickle cell is not the only genetic protection against malaria. This is frequently tested as a table-fill or matching question:
| Genetic factor | Mechanism of protection | Species affected |
|---|---|---|
| HbAS (sickle cell trait) | Impaired parasite growth; enhanced immunity; impaired cytoadherence | P. falciparum |
| HbC (haemoglobin C) | Reduces PfEMP1 surface expression on infected RBCs | P. falciparum |
| Alpha and beta thalassaemia | Reduced normal haemoglobin substrate for parasite | P. falciparum |
| G6PD deficiency | Oxidative stress in infected RBCs kills parasite; but mechanism complex | P. falciparum |
| Duffy blood group negativity | Absence of Duffy antigen (DARC receptor) on RBC surface | P. vivax only |
The Duffy antigen and P. vivax — a critical distinction:
P. vivax requires the Duffy antigen (also called DARC — Duffy Antigen Receptor for Chemokines) on the RBC surface to invade. More than 90% of West Africans and many of their diaspora descendants are Duffy-negative (FY*O allele) and are therefore naturally resistant to P. vivax infection. This is why P. vivax malaria is rare in West Africa but common in South Asia and Latin America.
Exam trap: The Duffy antigen story is specific to P. vivax only. It has no relevance to P. falciparum protection.
The Evolutionary Logic: Balancing Selection
This is the "Why does this matter clinically and intellectually?" section.
In a malaria-endemic environment, a child with HbAA has full susceptibility to fatal P. falciparum. A child with HbSS has sickle cell anemia with shortened life expectancy. But a child with HbAS gets the best of both worlds — no sickle cell disease and partial protection against the region's deadliest infection.
This creates balancing selection: the sickle allele is maintained at relatively high frequency in the population because heterozygotes have higher fitness than either homozygote in a malarious environment. In non-malarious regions (e.g., after the transatlantic slave trade displaced West Africans), the protective advantage disappears, but the sickle allele frequency remains elevated in those populations for many generations.
The geographic overlap of high HbS frequency and historical P. falciparum endemicity across sub-Saharan Africa, the Middle East, the Mediterranean, and India is one of the strongest pieces of evidence supporting the malaria hypothesis of sickle cell selection.
How to Remember
The AS advantage rule: "One sickle gene saves; two sickle genes suffer" HbAS = heterozygote = protected. HbSS = homozygote = suffers from malaria AND from sickle cell disease.
Remembering which parasite the Duffy antigen blocks: "Duffy stops VIVax" — the Duffy receptor is the entry door for P. vivax. No Duffy = no vivax entry. West Africans (Duffy-negative) are vivax-resistant, not falciparum-resistant.
Remembering G6PD and thalassaemia: Both protect against P. falciparum (the dangerous one). Think: the body's metabolic vulnerabilities (low G6PD, low haemoglobin) accidentally create a hostile environment for the parasite.
The evolutionary mnemonic: "Malaria wrote the sickle cell story" — in malaria-endemic regions, natural selection kept one copy of the sickle gene in the population because it saved lives. Remove malaria from the equation and the gene is just harmful.
Where Students Actually Get Confused
1. "HbAS protects — so people with sickle cell anemia are also protected, right?" No. HbSS is worse for malaria outcomes. The protection is specific to heterozygotes (HbAS). In HbSS, malaria is one of the commonest causes of sickle cell crisis. The fever, acidosis, and dehydration of malaria all trigger catastrophic sickling episodes.
2. "Duffy-negative means you can't get malaria." Incorrect. Duffy-negative protects only against P. vivax. Duffy antigen has nothing to do with P. falciparum entry. Duffy-negative individuals in malaria-endemic Africa are fully susceptible to falciparum malaria.
3. "G6PD deficiency always protects against malaria." The relationship is more complex. G6PD-deficient individuals appear to have reduced risk of severe falciparum malaria, but the mechanism is still debated. Additionally, G6PD deficiency is a contraindication to primaquine (used for P. vivax radical cure) — primaquine causes haemolytic anemia in G6PD-deficient patients. This is clinically crucial.
4. "The malaria-sickle cell relationship only matters for P. falciparum." Mostly correct for HbAS — the protection documented is predominantly against P. falciparum. But note the Duffy story for P. vivax is entirely separate.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Sickle cell trait genotype | HbAS (heterozygote) | One normal, one sickle allele |
| HbAS and malaria | Protects against severe P. falciparum (≈90% reduction in severe disease) | One sickle gene saves |
| HbSS and malaria | Worsens outcome; malaria triggers sickle crisis | Two sickle genes suffer |
| Mechanism (best supported) | Impaired parasite growth + sickling of infected RBCs + reduced cytoadherence | Multiple overlapping mechanisms |
| Duffy antigen role | Entry receptor for P. vivax on RBC surface | Duffy stops VIVax |
| West African Duffy status | >90% Duffy-negative | Resistant to P. vivax; not to P. falciparum |
| G6PD deficiency | Protective against severe P. falciparum | But: G6PD deficiency → primaquine causes haemolysis |
| Thalassaemia | Protective against P. falciparum | Reduced HbA substrate for parasite |
| Balancing selection | HbAS fitness > HbAA and HbSS in malaria-endemic environment | "Malaria wrote the sickle cell story" |
| Why HbS allele persists | Heterozygote advantage in malaria-endemic regions | Selection pressure from falciparum |
Self-Check Questions
- A child in Nigeria has genotype HbAS. Is he at higher, lower, or similar risk of dying from P. falciparum malaria compared to his HbAA sibling?
- Why does sickle cell trait (HbAS) protect against malaria, while sickle cell anemia (HbSS) does not?
- A West African woman is found to be Duffy-negative. Which Plasmodium species cannot infect her, and why?
- A patient with P. vivax malaria needs primaquine for radical cure, but their G6PD result is deficient. What is the clinical concern?
- Which type of natural selection explains why HbS remains common in malaria-endemic populations?
- Name three genetic factors (other than HbAS) that provide some protection against P. falciparum malaria.
Answers
- Lower risk — HbAS confers approximately 90% protection against severe disease.
- HbAS = heterozygote, produces both HbA and HbS, no sickling disease but parasite growth impaired; HbSS = homozygote, full sickling disease + malaria triggers crises.
- P. vivax — Duffy antigen is the RBC entry receptor for P. vivax; Duffy-negative cells cannot be invaded.
- Primaquine causes haemolytic anemia in G6PD-deficient individuals — use with caution or substitute.
- Balancing selection (heterozygote advantage).
- Any three of: HbC, G6PD deficiency, alpha/beta thalassaemia, Duffy-negative blood group.)
References
- Luzzatto, L. (2012). Sickle cell anemia and malaria. Mediterranean Journal of Haematology and Infectious Diseases, 4(1), e2012065. https://doi.org/10.4084/MJHID.2012.065
- Aidoo, M., Terlouw, D. J., Kolczak, M. S., et al. (2002). Protective effects of the sickle cell gene against malaria morbidity and mortality. The Lancet, 359(9314), 1311–1312. https://doi.org/10.1016/S0140-6736(02)08273-9
- Williams, T. N., Mwangi, T. W., Wambua, S., et al. (2005). Sickle cell trait and the risk of Plasmodium falciparum malaria and other childhood diseases. Journal of Infectious Diseases, 192(1), 178–186. https://doi.org/10.1086/430744
- Gong, L., Parikh, S., Rosenthal, P. J., & Greenhouse, B. (2013). Biochemical and immunological mechanisms by which sickle cell trait protects against malaria. Malaria Journal, 12, 317. https://doi.org/10.1186/1475-2875-12-317
- Menkin-Smith, L., & Winders, W. T. (2023). Plasmodium vivax Malaria. In StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK538333/
- Gracia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
Frequently Asked Questions
Does sickle cell trait protect against malaria?
How does sickle cell trait protect against malaria?
Why does the sickle cell gene remain common in malaria-endemic regions?
What is the Duffy antigen and how does it relate to malaria?
Why is primaquine dangerous in G6PD-deficient patients?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.