Serological Tests for Disease Diagnosis: A Complete Guide to Antibody Detection
Serological tests detect antibodies or antigens in patient serum to diagnose infections. This hub covers interpretation principles, seroconversion, the 9 key infections diagnosed serologically, all major test methods (ELISA, ICT, HAI, CFT, RIA, IFA), and links to detailed procedure articles for each test.
A 28-year-old woman presents to a health post with two weeks of fever and joint pain. A rapid diagnostic test for dengue IgM/IgG is performed and returns positive. The clinician diagnoses dengue fever and starts supportive treatment.
Three weeks later, she returns — still unwell. A repeat serology now shows a four-fold rise in Widal test titer. She had typhoid fever all along, and the dengue IgG was a remnant from an infection three years prior.
This case illustrates the most important principle in serology: antibody detection is indirect evidence of infection, not proof of current disease. Understanding how to interpret serological tests — what a positive result means, what it does not mean, when to trust it and when to repeat — is as important as knowing which test to order.
This article is the hub for all serological and immunodiagnostic content on Microbeonline. It explains the principles of antibody-based diagnosis, guides interpretation, and links to detailed articles for each specific test.
What This Hub Covers
| Section | What you will learn |
|---|---|
| How antibodies are produced and detected | B cell activation, seroconversion, window period |
| Why antibody presence ≠ current infection | Passive transfer, vaccination, cross-reactivity |
| How to interpret serological results | 4-fold rise, IgM vs IgG, cut-off titers |
| Antigen detection vs antibody detection | When to use which approach |
| Major serological test methods | ELISA, ICT, HAI, CFT, RIA, IFA, agglutination |
| Disease-specific serology | Dengue, Hepatitis B, HIV, Syphilis, Typhoid, and more |
Companion article: This hub covers antibody-based diagnostic tests. For antigen-based tests — NS1 dengue antigen, malaria RDTs, pneumococcal urinary antigen, HBsAg, HIV p24, H. pylori stool antigen, Cryptococcal CSF antigen — see Antigen Detection Tests for Disease Diagnosis.
Jump to any section using the table of contents, or use the links throughout to access full detailed articles on each test method or disease.
Antibodies are glycoproteins produced by our body in response to invading organisms or toxins (antigens). When a pathogen (bacteria, virus, protozoa, or helminth) enters our body and somehow manages to reach our bloodstream, antigen-presenting cells (such as macrophages, dendritic cells, or B cells) circulating in the bloodstream capture these pathogens and either destroy them or present them to appropriate T cells.
Receptors present on naïve B cells recognize the surface proteins of the pathogen. Antigens and other signals (such as MHC-II-peptide:TCR interaction and CD40-CD40L interaction) activate these naïve B cells. This results in the proliferation of antigen-specific cells (clonal expansion) and their differentiation into effector cells that actively secrete antibodies.
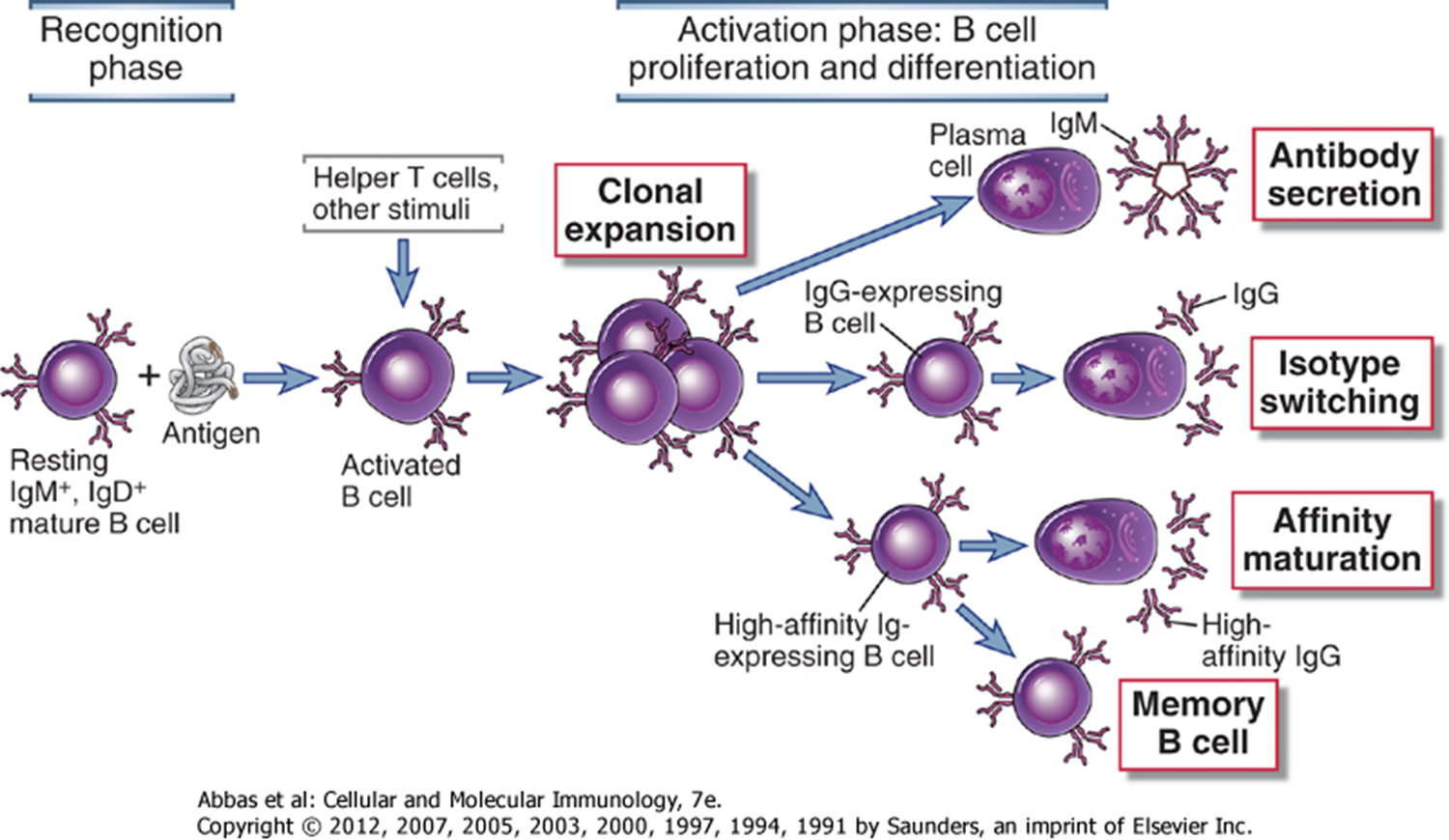 Figure: B Cell Activation and formation of Antibodies(Image source: Abbas-Cellular and Molecular Immunology)
Figure: B Cell Activation and formation of Antibodies(Image source: Abbas-Cellular and Molecular Immunology)
All these signals lead to activation of naïve B cells and convert them into antibody-producing cells (plasma cells). After the plasma cells start production of antibodies, the concentration of antibodies in the blood begins to rise slowly, as the initially formed antibodies are consumed in antigen capture (formation of Ag-Ab complex) and neutralization. As time passes and the disease progresses, the concentration of antigen in the bloodstream declines to a negligible level, while the concentration of antibodies increases to a detectable level. Seroconversion is the period between infection and the appearance of detectable antibodies in the serum; this duration varies by infection.
Presence of Antibodies in Blood ≠ Infection
In any systemic infection, antigen (Ag) always appears in the blood before antibodies do. For this reason, antigen detection tests or culture (when available) are used for initial diagnosis, and serological tests are used later.
If the pathogen does not reach the bloodstream or fails to mount sufficient humoral response, antibody detection tests may not be applicable to detect such infections. For example, antibody detection tests are not used to detect local or superficial skin infections (e.g. dermatophytoses), cholera (a toxin-mediated illness with no bloodstream invasion), giardiasis, etc.
The presence of antibodies against a particular infection (or pathogen of interest) should not be interpreted as evidence of active infection at that time, because antibodies may be present in the serum of individuals due to any of the following conditions:
- Vaccination
- Previous infection or sub-clinical infection (which is already subsided)
- Infection with another organism having antigenic similarity with the pathogen of interest
- Passively acquired from mother: If the person is a newborn, they might have acquired those antibodies from their mother through the placenta or breast milk. (All newborns of mothers who are antibody-positive for a particular disease/pathogen will have passively transferred maternal IgG. In such cases, titer can be high but may not indicate infection in the baby.
Following approaches should be used during interpretation of the serological tests
- A four-fold rise in antibody titer between acute- and convalescent-phase samples.
- Detection of IgM antibody against the pathogen of interest (indicates recent infection).
- Antibody titer should exceed the prevailing cut-off titer in the general population.
 The choice of the test methods for a particular pathogen of interest differs based on the nature of the organism, cost of the test procedure and facility available in the diagnostic laboratories.
The choice of the test methods for a particular pathogen of interest differs based on the nature of the organism, cost of the test procedure and facility available in the diagnostic laboratories.
Understanding the Window Period and Seroconversion
The window period is the time between infection and the appearance of detectable antibodies in serum. During this period, a patient may be infectious but serologically negative — a critically important concept for both clinical diagnosis and blood bank screening.
Window periods vary significantly between infections:
| Infection | Window period (approximate) | First antibody detectable |
|---|---|---|
| HIV | 18–45 days (3rd generation ELISA); 15–20 days (4th generation Ag/Ab combo) | IgM, then IgG |
| Hepatitis B | 6 weeks – 6 months | Anti-HBc IgM |
| Hepatitis C | 8–11 weeks (antibody); 1–2 weeks (RNA PCR) | Anti-HCV IgG |
| Dengue | 3–5 days (IgM); 14+ days (IgG) | IgM earlier in primary infection |
| EBV (mono) | 4–7 days after symptoms begin | Heterophile antibodies |
| Syphilis | 3–6 weeks after exposure | IgM (treponemal) |
Clinical implication: A negative serological test during the window period does not rule out infection. For HIV, a confirmed negative result requires testing 6 weeks after the last potential exposure (using 4th-generation tests) or 3 months (with older tests). For blood bank screening, NAT (nucleic acid testing) is used specifically because it detects the virus before antibodies appear.
Antigen Detection vs Antibody Detection: When to Use Which
In any infection, antigen (the pathogen or its components) appears in the blood before antibodies. This has direct implications for test selection:
| Approach | What is detected | Best for | Limitation |
|---|---|---|---|
| Antigen detection | The pathogen or its proteins directly | Early infection (before seroconversion); immunocompromised patients who may not mount antibody response | Antigen cleared quickly; may miss late-stage disease |
| Antibody detection (IgM) | Recent/acute infection | Diagnosis 5–14 days after onset; distinguishes recent from past infection | Window period — negative early; may cross-react |
| Antibody detection (IgG) | Past infection or immunity | Seroprevalence studies; vaccination response; paired samples (4-fold rise confirms acute infection) | Persists for life — positive does not mean current infection |
| Paired serology | Rising antibody titer | Gold standard for many viral infections | Requires two samples 2–4 weeks apart; delays diagnosis |
| Culture / molecular (PCR) | The organism directly | Definitive diagnosis; drug sensitivity testing | Slow (culture); expensive (PCR); not available everywhere |
The clinical rule: When a patient is acutely ill, start with antigen detection or culture if available. When culture is negative or unavailable, or when diagnosis is retrospective, use serology. When confirming immunity (e.g., post-vaccination HBsAb), IgG is appropriate.
Serological Test Methods (Overview with Links)
Choice of method depends on the pathogen, the cost of the test, and what's available in the lab — a district hospital and a tertiary referral center won't reach for the same test. The following table maps every major serological test method to its principle, clinical applications, and detailed article on this site:
| Method | Principle | Key applications | Detailed article |
|---|---|---|---|
| ELISA (Enzyme-Linked Immunosorbent Assay) | Antigen or antibody bound to solid phase; enzyme-linked conjugate; colour reaction | HIV, HBV, HCV, dengue, toxoplasma; most versatile serological platform | ELISA |
| Immunochromatography (ICT/RDT) | Lateral flow; antibody-labelled coloured particles migrate across membrane | Rapid diagnosis: malaria, dengue, HIV, typhoid, COVID-19, pregnancy tests | Immunochromatography |
| Haemagglutination Inhibition (HAI) | Antibodies inhibit virus-mediated red cell agglutination | Influenza, rubella, mumps serology | HAI test |
| Widal Test (tube/slide agglutination) | Patient antibodies agglutinate killed Salmonella antigens | Typhoid fever serology | Widal test |
| TPHA | Patient antibodies agglutinate T. pallidum-coated particles | Confirmatory syphilis test | TPHA |
| RPR (Rapid Plasma Reagin) | Non-treponemal; antibodies react with cardiolipin antigen; carbon particle flocculation | Syphilis screening; treatment monitoring | RPR |
| FTA-ABS | Indirect fluorescent antibody; patient antibodies react with T. pallidum | Confirmatory syphilis; most sensitive treponemal test | FTA-ABS |
| VDRL | Non-treponemal flocculation; cardiolipin antigen | Syphilis screening; CSF VDRL for neurosyphilis | VDRL |
| ASO Titer | Latex agglutination; antibodies to streptolysin O | Post-streptococcal disease (rheumatic fever, GN) | ASO titer |
| Monospot Test | Heterophile antibody agglutination of horse/ox RBCs | Infectious mononucleosis (EBV) | Monospot test |
| Complement Fixation Test (CFT) | Antigen-antibody complex fixes complement; indicator system (sensitised RBCs) | Mycoplasma, rickettsia, viral serology | CFT |
| Radioimmunoassay (RIA) | Radiolabelled antigen competes with patient antigen for antibody binding | Hormone levels; hepatitis markers; high sensitivity applications | RIA |
| Direct Fluorescent Antibody (DFA) | Fluorescent-labelled antibody applied directly to specimen | Rapid detection of organisms in tissue/smears (Legionella, Bordetella, HSV) | DFA |
| Indirect Fluorescent Antibody (IFA) | Patient antibody binds antigen; fluorescent anti-human IgG secondary antibody | ANA (autoimmune), IFAT for malaria/Leishmania, FTA-ABS | IFA |
| Immunofluorescence Assay (IFA general) | Fluorescent labelling for antigen or antibody detection | Wide range: viral, bacterial, parasitic, autoimmune | Immunofluorescence |
| CIE (Counterimmunoelectrophoresis) | Antigen and antibody migrate toward each other in electric field; precipitin line forms | Bacterial antigen detection in CSF (Pneumococcus, Meningococcus, Haemophilus) | CIE |
| Western Blot | Electrophoresis separates antigens; patient antibodies detected by band pattern | HIV confirmatory; Lyme disease confirmation | Western Blot |
| Hepatitis B serology interpretation | Combined antigen (HBsAg, HBeAg) and antibody (anti-HBc, anti-HBs) panel | Staging HBV infection; vaccination response; carrier identification | HBV serology |
The following diseases are commonly diagnosed serologically. For each, the table provides the test name, what is detected, and the key clinical note. Click through to the detailed article for full procedure, interpretation, and troubleshooting.
| Disease | Test(s) used | What is detected | Key clinical note | Article |
|---|---|---|---|---|
| Dengue fever | NS1 antigen RDT/ELISA (days 1–7); IgM/IgG ELISA; HAI | NS1 antigen (acute phase); Anti-dengue IgM (primary); IgG (secondary/past) | NS1 antigen detectable days 1–7, use before IgM appears; IgM detectable by day 3–5; IgG cross-reacts with other flaviviruses | Dengue virus |
| Malaria | RDT (HRP2, pLDH); blood film microscopy | HRP2 antigen (P. falciparum); pLDH (all species); aldolase (pan-malarial) | RDTs detect antigen directly — no antibody window period; HRP2 most sensitive for P. falciparum; pLDH distinguishes species | Malaria-Lab Diagnosis |
| Hepatitis B | HBsAg, HBeAg, anti-HBc, anti-HBs (panel) | Antigen (active infection) + antibody (immunity/past) | Panel interpretation distinguishes acute, chronic, carrier, immune states | HBV serology |
| HIV/AIDS | RDTs (Tri-Dot); ELISA; Western Blot | Anti-HIV IgG/IgM; p24 antigen (4th gen) | Window period 18–45 days; neonatal diagnosis requires PCR not serology | HIV/AIDS |
| Post-streptococcal disease | ASO titer | Anti-streptolysin O antibody | >200 IU/mL indicates recent S. pyogenes infection; titer remains elevated weeks after infection | ASO titer |
| Syphilis | RPR/VDRL (screening) + TPHA/FTA-ABS (confirmatory) | Non-treponemal (cardiolipin) + treponemal antibodies | Two-test algorithm: screen with non-treponemal; confirm with treponemal; treat based on clinical stage | RPR · TPHA · FTA-ABS |
| Typhoid fever | Widal test | Agglutinating antibodies against O, H, AH, BH antigens | Positive after day 10; cut-off depends on population baseline — your own research (anti-O >1:80, anti-H >1:160 for Nepal) | Widal test |
| Visceral leishmaniasis | rK39 RDT; IFAT | Anti-rK39 IgG | rK39 rapid test highly sensitive and specific for kala-azar in endemic areas | Leishmaniasis lab diagnosis |
| Hepatitis C | Anti-HCV ELISA; HCV RNA (confirmatory) | Anti-HCV IgG | Antibodies persist for life; positive serology requires RNA PCR confirmation of active infection | Hepatitis C Virus |
| Infectious mononucleosis | Monospot (heterophile); EBV-specific IgM/IgG | Heterophile antibodies; anti-VCA IgM/IgG | Monospot false-negative in <5 years age; VCA IgM = primary infection; IgG anti-EBNA = past infection | Monospot test |
| Brucellosis | Standard tube agglutination (STA); Rose Bengal Plate Test | Anti-Brucella agglutinins | Titre ≥1:160 suggestive; common cause of PUO; zoonosis in cattle-farming regions | Brucella |
How to Remember
The serology timeline — three phases of every infection:
EXPOSURE
↓
[Window period — culture or antigen detection only]
↓
IgM appears (3–14 days post-onset) → ACUTE infection
↓
IgG rises, IgM declines → RECENT/RESOLVING infection
↓
IgM gone, IgG persists → PAST infection or immunity
This single timeline explains 90% of serology interpretation questions. The key variable is which immunoglobulin class is elevated and when relative to symptoms.
The two-test rule for syphilis: Screen with a non-treponemal test (RPR or VDRL; cheap, quantitative, monitors treatment). Confirm with a treponemal test (TPHA or FTA-ABS; specific, stays positive for life). Never diagnose syphilis on a non-treponemal test alone; false positives from lupus, pregnancy, and other conditions are common.
The four reasons antibodies can be positive without current infection:
- Vaccination
- Past resolved infection
- Cross-reactive antigen (another organism)
- Passive maternal antibody (neonates)
Memorise these four because they appear in every serology interpretation question and clinical scenario involving unexpected positive results.
References
- Delforge M. L. (2011). De l’utilité ou non de la sérologie infectieuse: morceaux choisis [On the usefulness of serology testing in infectious diseases: selected topics]. Revue medicale de Bruxelles, 32(4), 285–288.
- Feng, Z., Li, Z., Sui, B., Xu, G., & Xia, T. (2005). Serological diagnosis of infectious mononucleosis by chemiluminescent immunoassay using capsid antigen p18 of Epstein-Barr virus. Clinica chimica acta; international journal of clinical chemistry, 354(1-2), 77–82. https://doi.org/10.1016/j.cccn.2004.11.010
- Delforge M.L. (2011). De l'utilité ou non de la sérologie infectieuse. Revue médicale de Bruxelles, 32(4), 285–288. (keep)
- Feng Z. et al. (2005). Serological diagnosis of infectious mononucleosis. Clinica chimica acta, 354(1-2), 77–82. (keep)
- Tille, P. M. (2017). Bailey and Scott's Diagnostic Microbiology (14th ed.). Elsevier.
- WHO. (2003). Manual for the Laboratory Identification and Antimicrobial Susceptibility Testing of Bacterial Pathogens of Public Health Importance. Geneva: WHO.
- Acharya T., Tiwari B.R., Pokhrel B.M. (2013). Reassessment of the Widal Test Cut-Off Titre for Diagnosis of Typhoid Fever in the Nepalese Context. JHAS, 3(1):27–30.

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.