Novobiocin Susceptibility Test: How One Disk Tells S. saprophyticus From a Contaminant
A 5 ug novobiocin disk separates S. saprophyticus, a real cause of UTI in young women, from S. epidermidis, usually just skin contamination. Full procedure, the corrected 16mm breakpoint, and the species this test does and doesn't apply to.
A young, sexually active woman comes in with dysuria and urgency. Urine culture grows gram-positive cocci in clusters, catalase-positive, coagulase-negative. Without the novobiocin test, this could be dismissed as skin contamination, the same picture S. epidermidis would give. With it, a resistant result confirms a genuine pathogen, S. saprophyticus, the second most common cause of uncomplicated UTI in this population after E. coli. One disk is the difference between treating a real infection and writing it off as a contaminated sample.
Novobiocin test is used to differentiate coagulase-negative staphylococci (CONS) and presumptively identify the isolate as Staphylococcus saprophyticus (novobiocin resistant). It is usually performed on CONS isolated from a urine sample of women of a reproductive age group.
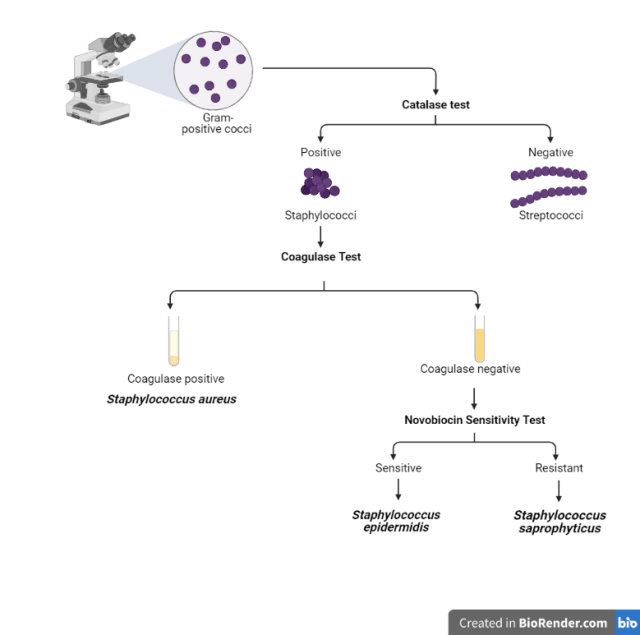 Figure: Flow chart for the identification of Staphylococcus saprophyticus
Figure: Flow chart for the identification of Staphylococcus saprophyticus
Principle of Novobiocin Test
S. saprophyticus is second only to E. coli as the most frequent causative organism of uncomplicated urinary tract infections (UTIs) in young sexually active women. So when an organism that looks like staphylococci is isolated from a woman of reproductive age coagulase test is done. If the organism is coagulase-negative i.e. CONS the laboratory must further identify that isolate and find out if this is a true pathogen (Staphylococcus saprophyticus-novobiocin resistant) or a contaminant (i.e. Staphylococcus epidermidis-novobiocin sensitive).
Mnemonic: On the office’s STAPH retreat, there was NO StRESs. (NO=novobiocin, S=Saprophyticus, R=Resistant, E=Epidermidis, S=Sensitive
Laboratory identification of S. saprophyticus is made on the basis of the absence of hemolysis, coagulase, and resistance to novobiocin. Novobiocin susceptibility test results are 100% sensitive and 96% specific. S. saprophyticus is innately resistant to the antibiotic novobiocin. Therefore, screening coagulase-negative staphylococci from urine cultures for novobiocin resistance is reliable presumptive identification of S. saprophyticus.
Test organism
- Testing should be performed on isolated colonies of gram-positive cocci in clusters that are catalase-positive and coagulase-negative isolated from urine specimens, usually from sexually active young women.
- All colonies should be taken from a blood agar plate and growth must be less than 24 hours old, 15-18 hours being optimal.
Procedure of Novobiocin test
- Allow containers to come to room temperature before use.
- Using a pure 18-24 hour culture, prepare a suspension of the organism; equivalent to a McFarland 0.5 opacity standard; to be identified in tryptic soy broth, sterile water, or brain heart infusion (BHI) broth
- Inoculate Mueller Hinton Agar, 5% blood agar, or tryptic soy agar plate with a sterile swab to obtain confluent growth.
- Aseptically apply one 5ug novobiocin disk onto the inoculated agar surface and lightly press down to ensure full contact with the medium.
- Incubate plate aerobically for 18 to 24 hours at 35 to 37°C.
- Measure (in millimeters) the diameter of the zone of inhibition around the novobiocin disk, and record it as susceptible or resistant.
Interpretation of Novobiocin test
- Sensitive (susceptible) – zone diameter ≥ 16 mm
- Resistant – zone diameter < 16 mm (typically S. saprophyticus shows little to no zone, often growth up to the disk edge)
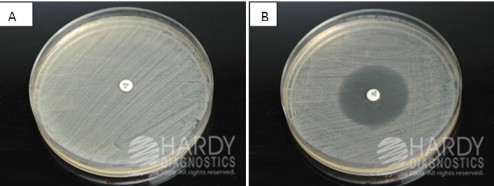 Figure: Novobiocin sensitivity testing A. Novobiocin-resistant (S. saprophyticus)
Figure: Novobiocin sensitivity testing A. Novobiocin-resistant (S. saprophyticus)
B. Novobiocin Sensitive (S. epidermidis)
Expected results:
- Staphylococcus saprophyticus (resistant) – zone ≤16 mm, typically little to no zone with growth up to the edge of the disk
- Staphylococcus epidermidis (susceptible) – zone >16 mm
Novobiocin is one of three disk-diffusion tests used to separate look-alike Gram-positive cocci, alongside optochin (for S. pneumoniae among the alpha-hemolytic streptococci) and bacitracin (for Group A strep among the beta-hemolytic streptococci). Novobiocin is the one you reach for on the catalase-positive, coagulase-negative side: a coagulase-negative Staphylococcus from urine. The catalase and coagulase results route you here. See the Gram-positive coccus disk-test grid on the optochin page for the full routing.
Quality Control
Quality control of novobiocin test should be performed per lot/shipment date with known organisms.
- Positive control (resistant) = Staphylococcus saprophyticus (ATCC® 15305)
- Negative control (sensitive) = Staphylococcus epidermidis (ATCC® 12228)
Limitation
The novobiocin disk is not helpful and can give misleading results if it is performed on isolates other than those from urinary specimens. Occasional human isolates that are not S. saprophyticus, S. cohnii subsp., or S. xylosis may also be resistant to novobiocin.
Novobiocin-Resistant vs. Novobiocin-Susceptible CoNS
Knowing the test result only matters if you know which species fall on which side of it.
Novobiocin-Resistant (little or no zone; growth up to the disk) | Novobiocin-Susceptible (zone ≥16mm) |
|---|---|
S. saprophyticus (the clinically important one) | S. epidermidis (the common skin contaminant) |
S. cohnii | S. capitis |
S. xylosus | S. hominis |
S. kloosii | S. lugdunensis |
This is exactly why the test result alone is not a species identification. A novobiocin-resistant CoNS from a urine sample in a young woman is presumptively S. saprophyticus, but a handful of other resistant CoNS species exist too, which is the basis for the Limitation noted above: this test is only reliable on urinary isolates, not as a general CoNS identification method.
Exam Facts
| Answer | |
|---|---|
| What does novobiocin inhibit? | DNA gyrase, blocking DNA replication |
| Disk potency used? | 5 ug |
| Susceptible breakpoint? | Zone diameter ≥ 16 mm |
| Reported sensitivity and specificity of the test? | 100% sensitive, 96% specific |
| Why is this test unreliable outside urinary isolates? | Other novobiocin-resistant CoNS species (S. cohnii, S. xylosus, S. kloosii) exist and would give a false impression of S. saprophyticus identification |
References
- Afanas’eva, T. I., Shcherbakova, N. A., Givental’, N. I., & Bogdanova, L. F. (1979). Znachenie opredeleniia chuvstvitel’nosti k novobiotsinu v taksonomii stafilokokkov [Significance of determining novobiocin sensitivity in the taxonomy of staphylococci]. Antibiotiki, 24(11), 824–827.
- Leighton, P. M., & White, M. (1983). Rapid determination of novobiocin susceptibility for the identification of Staphylococcus saprophyticus. Diagnostic microbiology and infectious disease, 1(3), 261–264. https://doi.org/10.1016/0732-8893(83)90026-3
- Kloos WE, Schleifer KH. Simplified scheme for routine identification of human Staphylococcus species. J Clin Microbiol. 1975;1(1):82-88. doi:10.1128/jcm.1.1.82-88.1975
- Procop GW, Church DL, Hall GS, Janda WM, Koneman EW, Schreckenberger PC, Woods GL. Koneman's Color Atlas and Textbook of Diagnostic Microbiology. 7th ed. Philadelphia: Wolters Kluwer; 2017.
- Tille PM. Bailey and Scott's Diagnostic Microbiology. 15th ed. St. Louis: Elsevier; 2022.
Frequently Asked Questions
What does the novobiocin susceptibility test actually identify?
What is the breakpoint for a susceptible result?
Why is this test unreliable outside urinary specimens?
What does novobiocin actually inhibit in the bacterial cell?
Why does it matter clinically whether an isolate is S. saprophyticus or S. epidermidis?
What are the quality control strains for this test?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.