Naegleria fowleri (Brain-Eating Amoeba): Life Cycle, Transmission, Symptoms, and Prevention
How does a warm freshwater amoeba cause a 97% fatal brain infection in days? Naegleria fowleri life cycle, the olfactory nerve route to the brain, lab diagnosis, and the prevention measures that actually work.
A healthy 12-year-old boy spends an afternoon swimming and diving in a warm lake in late August. Five days later, he develops a headache, fever, and vomiting; symptoms his parents reasonably assume are a stomach virus. Within 48 hours, he is confused, has a stiff neck, and begins seizing. He is dead within a week of the first headache.
There was no warning sign that distinguished this from ordinary summer illness until it was too late. Naegleria fowleri causes one of the most rapidly fatal infections known in medicine — primary amebic meningoencephalitis (PAM) kills more than 97% of those infected, usually within five days of symptom onset. It is also, paradoxically, one of the most preventable infections in parasitology: the organism cannot infect through swallowed water, cannot spread person-to-person, and a single simple behavioural change (keeping water out of the nose) eliminates the risk almost entirely. Understanding exactly how this organism travels from warm water to the brain is what makes that prevention message make sense and what makes the diagnosis recognizable before it is too late.
Naegleria is distributed worldwide in various freshwater habitats (including rivers, lakes, ponds, hot springs, spas, domestic water systems, air-conditioning systems, humidifiers, and cooling towers) and soil.
Naegleria fowleri is not found in saltwater, like in the ocean.
Naegleria fowleri is a thermophilic (heat-loving) organism. It grows best at higher temperatures up to 115°F (46°C) and cand is less likely to be found in the water as temperatures decline below 77°F (25°C). So infection mainly occurs during the summer months of July, August, and September.
Naegleria is not related to the intestinal amebae and does not inhabit the intestines of humans or other mammals.
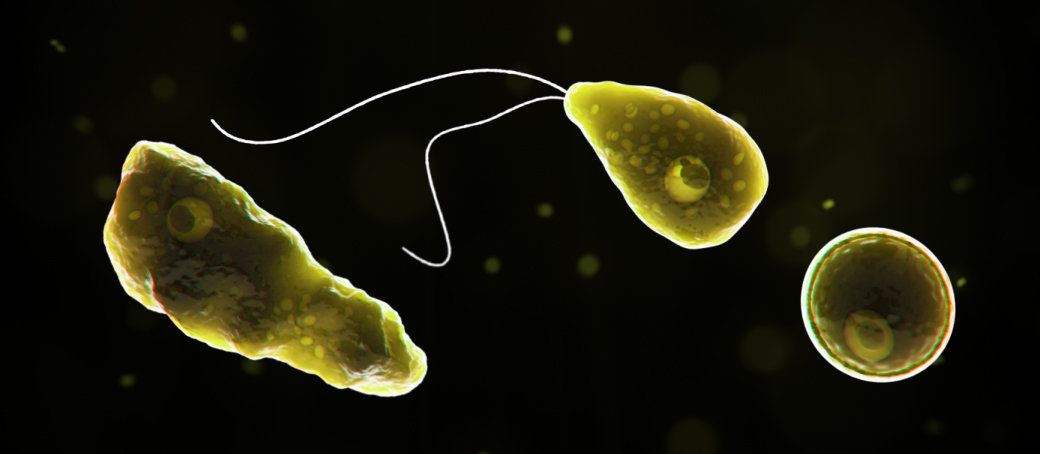 Figure: A computer-generated representation of Naegleria fowleri in its ameboid trophozoite stage, in its flagellated stage, and in its cyst stage (left to right). Image source: CDC
Figure: A computer-generated representation of Naegleria fowleri in its ameboid trophozoite stage, in its flagellated stage, and in its cyst stage (left to right). Image source: CDC
Stages of Naegleria fowleri
Trophozoite
Trophotozie is the only infective stage of Naegleria fowleri. Trophozoites are 10-35 µm long with a granular appearance and a single nucleus. Naegleria fowleri trophozoites are found in cerebrospinal fluid (CSF) and tissue.
Flagellate
Trophozoites can turn into a temporary, non-feeding, flagellated stage (10-16 µm in length) when stimulated by adverse environmental changes such as a reduced food source. Flagellated forms of Naegleria fowleri are occasionally found in CSF. They revert to the trophozoite stage when favorable conditions return.
Cyst
If the environment is not conducive to continued feeding and growth (like cold temperatures, food becomes scarce), the ameba or flagellate will form a cyst. The cyst form is spherical and about 7-15 µm in diameter. It has a smooth, single-layered wall with a single nucleus.
Cysts are environmentally resistant, which increases their chances of survival until better environmental conditions occur. Cysts are not seen in brain tissue.
Mode of Transmission
Naegleria fowleri usually infects people when contaminated water enters the body through the nose typically during swimming or diving in warm freshwater places. Naegleria fowleri infection cannot be spread from one person to another.
The occurrence ofNaegleria fowleri in freshwater is common but the infection is rare.
Life Cycle
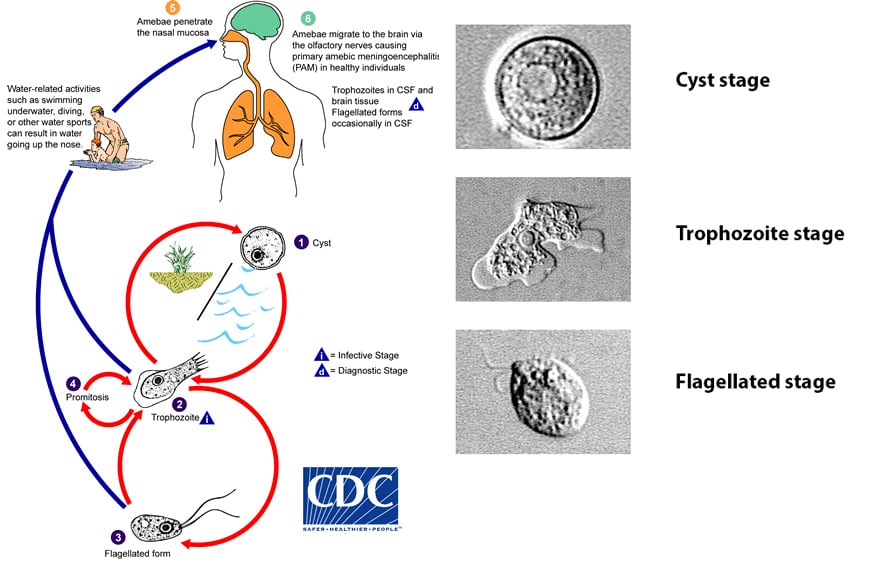 Figure: Life cycle of Naegleria fowleri (Image source: CDC)
Figure: Life cycle of Naegleria fowleri (Image source: CDC)
Naegleria fowleri has three stages in its life cycle: cyst, trophozoite, and flagellate. The trophozoites replicate by binary division, during which the nuclear membrane remains intact (a process called promitosis).
Trophozoites infect humans or animals by penetrating the nasal tissue and Migrating to the brain via the olfactory nerves causing primary amebic meningoencephalitis (PAM).
The upper respiratory tract is the true “primary” site of the infection. Most patients with Naegleria CNS infections have been children or young adults swimming in lakes or rivers. After infecting the nasal mucosa, N. fowleri spreads along the olfactory nerve through the cribriform plate into the brain. After reaching the brain, Naegleria fowleri can cause primary amebic meningoencephalitis (PAM) in healthy individuals.
Swallowing water contaminated with Naegleria does not cause infection.
Why PAM Progresses So Fast and Kills So Reliably
Three biological features combine to make this infection uniquely devastating:
1. Direct CNS entry, bypassing normal barriers. Most pathogens reaching the brain must cross the blood-brain barrier, a significant obstacle that slows or blocks many infections. Naegleria fowleri avoids this barrier entirely by travelling along the olfactory nerve through the cribriform plate — a direct anatomical shortcut from the nasal cavity into the brain that has nothing to do with the bloodstream. By the time the immune system would normally mount a response, the organism is already inside the CNS.
2. The trophozoite is a feeding, destructive organism, not a passive coloniser. Unlike many CNS pathogens that cause damage indirectly through immune-mediated inflammation, Naegleria trophozoites actively feed on brain tissue, producing the haemorrhagic necrosis described in the Sign and Symptoms section. This is a mechanical, ongoing tissue destruction process, not solely an inflammatory one — and it explains the prominent association of trophozoites with blood vessels noted in the pathology findings.
3. Misleadingly nonspecific early symptoms delay diagnosis. Because initial symptoms (headache, fever, nausea, vomiting) are identical to viral illness or bacterial meningitis, and because the disease is rare enough that most clinicians have never seen a case, the diagnosis is frequently made late or only at autopsy. Given the 1–9 day incubation period and a typical 5-day course to death, even a 24–48 hour diagnostic delay represents a substantial fraction of the entire available treatment window.
Why a handful of patients survive anyway: Documented survivors share two factors — exposure history that prompted very early suspicion (often because a parent or clinician specifically asked about recent freshwater swimming), and rapid initiation of aggressive combination therapy before extensive brain damage occurred. Survival is not about a uniquely effective drug; it is almost entirely about how early treatment starts.
Sign and Symptoms
N. fowleri causes primary amebic meningoencephalitis (PAM) the symptoms of which are similar to symptoms of bacterial meningitis. Initial symptoms of PAM start about 5 days (range 1 to 9 days) after infection.
- The initial symptoms may include headache, fever, nausea, or vomiting.
- Later symptoms can include stiff neck, confusion, lack of attention to people and surroundings, loss of balance, seizures, and hallucinations.
Primary amebic meningoencephalitis is characterized by large areas of hemorrhagic necrosis, especially involving the olfactory bulbs, frontal lobes, base of the brain, proximal spinal cord, and/or temporal lobes of the brain. The parietal lobes and occipital cortex may also be involved. Acute purulent exudate is found in the leptomeninges and within the cortex.
Amebic trophozoites are scattered or may be seen focally in clusters within necrotic cortex. They especially show a predilection for blood vessels; small arteries, arterioles, veins, venules, and capillaries may be surrounded by Naegleria trophozoites containing a large prominent karyosome. This disease progresses rapidly and usually causes death within about 5 days (range 1 to 12 days).
The fatality rate of Nageleria fowleri infection is over 97%.
Laboratory Diagnosis
Sample
Cerebrospinal fluid or CNS tissue is the sample of choice for diagnosing meningoencephalitis caused by N. fowleri. Specimen for culture should be collected aseptically and maintained at 20°C to 30°C during transport to the laboratory. If an immediate examination is impossible, the fluid can be kept at room temperature (The amoebae can survive several days at room temperature). The specimen should never be frozen or refrigerated.
Direct Microscopic Examination
Small drops of CSF or tissue suspension should be examined in wet mounts on slides under coverslips by light microscopy under reduced light, or phase-contrast microscopy for motile trophozoites (using a 40x objective). Motile Naegleria may be seen in the preparation (Naegleria is actively motile at 22°C to 25°C). The amebae can also be stained with a variety of stains, such as Giemsa-Wright or a modified trichrome stain.
Morphologic Feature
N. fowleri has two stages-motile trophozoites and non-motile cysts.
Trophozoites of Naegleria are 8-15 μm in diameter and contain large, prominent karyosome. Naegleria has one or more smooth, lobate pseudopods and is actively motile at room temperature. Naegleria species are characterized by a temporary ameboflagellate stage. When Naegleria trophozoites are put in distilled water, they may develop pear-shaped, actively motile forms containing two or more flagella (within 1 to 3 hours).
Cysts of Naegleria fowleri are uninucleate, spherical, 7-15 um in diameter and are surrounded by a relatively thin cyst wall; a feature that makes N. fowleri cyst susceptible to desiccation.
Identification of Naegleria beyond the genus level is usually achieved by nucleic acid sequencing.
Ameba Culture
Naegleria fowleri can be grown in culture by inoculating it into a growth plate containing lawn culture of Escherichia coli or Klebsiella aerogenes (these bacteria serve as a food source for Naegleria fowleri). The growth plate is then incubated at 42°C to kill other free-living amebae. The appearance of tracks made by an ameba in the lawn culture confirms the presence of thermophilic amebae which could be Naegleria. The presence of Naegleria is then confirmed by PCR or direct visualization.
Antigen detection
Naegleria fowleri antigen present in a sample can be detected using a specific antibody to Naegleria fowleri by indirect immunofluorescence techniques.
Polymerase Chain Reaction
The presence of Naegleria fowleri in CSF or biopsy specimens can be ascertained using molecular techniques. The presence of a specific DNA sequence of this organism can be detected after amplifying it using polymerase chain reaction (PCR).
Treatment
There is no single proven curative therapy for PAM, and the disease remains fatal in the overwhelming majority of cases — only a small number of documented survivors exist worldwide. The CDC recommends aggressive combination therapy, typically including:
- Amphotericin B (intravenous and intrathecal) — the longstanding mainstay of treatment, present in the regimen of every documented survivor
- Miltefosine — an antiparasitic agent originally developed for leishmaniasis, now considered a key addition based on laboratory activity against free-living amoebae and survivor outcomes
- Azithromycin — may have a synergistic effect when combined with amphotericin B
- Fluconazole or voriconazole
- Rifampin
- Dexamethasone — to manage cerebral oedema and elevated intracranial pressure
Why early treatment is everything: Every well-documented survivor was treated very early in the disease course, often based on strong clinical suspicion from a recent freshwater exposure history rather than waiting for definitive laboratory confirmation. Aggressive management of elevated intracranial pressure — sometimes including therapeutic hypothermia — has also been used alongside antimicrobial therapy in survival cases. This is why a clinician's index of suspicion, triggered simply by asking "has this patient been swimming in warm freshwater recently?", may matter as much as the specific drugs chosen.
Prevention
Because there is no reliable cure and the fatality rate exceeds 97%, prevention is by far the most effective tool against this disease — and fortunately, the transmission mechanism makes prevention straightforward:
- Avoid getting water up the nose while swimming, diving, or playing in warm freshwater (lakes, rivers, hot springs, poorly chlorinated or unchlorinated pools, splash pads) during warm months
- Use nose clips or hold the nose shut when jumping or diving into warm freshwater
- Avoid putting your head underwater in warm freshwater bodies, particularly in shallow, stagnant, or warmer water near the shore
- Avoid digging in or stirring up sediment in shallow warm water, since Naegleria can be present in higher concentrations near the bottom
- Use only sterile, distilled, or properly boiled/filtered water for nasal irrigation (e.g., neti pots, sinus rinsing) — this is a separate but important transmission route distinct from recreational swimming, and has caused confirmed infections and deaths
What does NOT cause infection:
- Swallowing water contaminated with Naegleria does not cause infection — as already noted in this article, the organism must specifically enter through the nose to reach the olfactory nerve. Drinking contaminated water poses no PAM risk.
- Properly chlorinated and maintained swimming pools are not a significant risk, since Naegleria does not survive adequate chlorination
- Person-to-person transmission does not occur
Why this matters for public health messaging: Because the organism is common in warm freshwater (the CDC notes it is frequently present in lakes and rivers during summer) but the disease is extremely rare, blanket avoidance of all freshwater recreation is not the message — the message is specifically about keeping water out of the nose. This distinction is what allows public health guidance to be both honest about the ubiquity of the organism and reassuring about the rarity of actual disease.
Where Students Actually Get Confused
1. "Naegleria fowleri infects the same way other amoebae cause disease — by ingestion." No — and this is the single most important transmission point in this entire topic. Unlike Entamoeba histolytica (feco-oral, ingested cysts), Naegleria fowleri infects exclusively through nasal entry, with trophozoites travelling along the olfactory nerve to the brain. Swallowing contaminated water, as the article already states, does not cause infection. This is precisely why nasal water exposure (diving, nose clips, neti pots) is the entire focus of prevention, while drinking water is not a concern at all.
2. "Naegleria fowleri and Acanthamoeba cause the same disease." They are both free-living amoebae capable of causing CNS infection, but the diseases, populations affected, and time courses differ substantially. Naegleria causes the fulminant, rapidly fatal PAM typically in healthy children and young adults after acute freshwater exposure, with death often within a week. Acanthamoeba causes granulomatous amebic encephalitis (GAE), a much slower, more indolent CNS infection typically affecting immunocompromised individuals, and Acanthamoeba is also a well-known cause of amoebic keratitis in contact lens wearers — a completely separate clinical entity not caused by Naegleria.
3. "Naegleria has only two life cycle stages, like most other amoebae." Naegleria fowleri is unusual in having three stages: trophozoite, a transient flagellate stage, and cyst — most amoebae of medical importance (e.g., Entamoeba) have only a trophozoite and cyst stage, with no flagellated intermediate. The flagellate stage is temporary and non-feeding, triggered by adverse environmental conditions, and reverts back to trophozoite when conditions improve.
4. "Finding cysts in brain tissue would confirm the diagnosis." As the article notes, cysts are not seen in brain tissue — only trophozoites are found in CSF and CNS tissue during active infection. The cyst form exists specifically as an environmental survival stage outside the human host. A laboratory or pathology report describing cysts in brain tissue should prompt reconsideration of the diagnosis, not confirmation of Naegleria PAM.
5. "A negative CSF wet mount rules out Naegleria infection." Given the rarity, rapid progression, and historically frequent missed/delayed diagnoses of this disease, a single negative wet mount in a clinically compatible case (especially with a relevant freshwater exposure history) should prompt repeat testing, PCR, or specialist consultation (e.g., with the CDC's Free-Living and Intestinal Amebas Laboratory) rather than ruling out the diagnosis outright.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Disease caused | Primary amebic meningoencephalitis (PAM) | "Brain-eating amoeba" |
| Organism type | Free-living, thermophilic amoeba | NOT related to intestinal amoebae |
| Habitat | Warm freshwater, soil; NOT saltwater | Rivers, lakes, hot springs, poorly chlorinated pools |
| Optimal growth temperature | Up to 115°F (46°C) | Explains summer seasonality (July–Sept) |
| Three life cycle stages | Trophozoite, flagellate (transient), cyst | Unusual — most amoebae have only 2 stages |
| Only infective stage | Trophozoite | Flagellate and cyst are not infective |
| Route of entry | Nasal — NOT ingestion | Swallowing contaminated water does NOT cause infection |
| Pathway to brain | Nasal mucosa → olfactory nerve → cribriform plate → brain | Bypasses blood-brain barrier entirely |
| Incubation period | 1–9 days (typically ~5 days) | Symptoms mimic bacterial meningitis |
| Time to death | Typically within 5 days (range 1–12) of symptom onset | Among the fastest-killing infections known |
| Case fatality rate | >97% | A small number of documented survivors exist |
| Cysts in brain tissue? | NOT seen | Only trophozoites found in CNS/CSF |
| Culture method | Lawn of E. coli/Klebsiella aerogenes, incubated at 42°C | Heat selects for thermophilic amoebae |
| Treatment regimen | Amphotericin B + miltefosine + azithromycin + rifampin + fluconazole/voriconazole + dexamethasone | Combination therapy; no single proven cure |
| Key survival factor | Very early treatment initiation | Suspicion from exposure history, not waiting for confirmation |
| Person-to-person spread | Does NOT occur | Reassurance point for public health messaging |
| Key confused organism | Acanthamoeba — causes slower GAE + keratitis, not PAM | Different disease, different population, different speed |
Self-Check Questions
- A child develops headache and fever five days after swimming in a warm lake, and is initially treated for suspected viral illness. What exposure-history question, if asked early, could have changed the diagnostic timeline?
- Why does Naegleria fowleri infection progress so much faster than most other CNS infections?
- A patient is concerned about Naegleria infection after accidentally swallowing lake water while swimming. Is this a valid concern?
- A CSF sample from a suspected PAM case shows only cysts, no trophozoites. Does this confirm the diagnosis?
- How does Naegleria fowleri infection differ from Acanthamoeba CNS infection in terms of speed, population affected, and additional disease manifestations?
- Why is nose-clip use during diving in warm freshwater a specifically targeted prevention measure, rather than general advice to avoid all water contact?
Answers
- Asking specifically whether the child had recently been swimming or diving in warm freshwater could have prompted earlier suspicion of PAM. Because initial symptoms are nonspecific and mimic viral illness or bacterial meningitis, a relevant exposure history is often the only early clue pointing toward this rare diagnosis, and earlier suspicion enables earlier aggressive treatment — the single most consistent factor among documented survivors.
- Naegleria fowleri reaches the brain by travelling directly along the olfactory nerve through the cribriform plate, bypassing the blood-brain barrier entirely — a barrier that slows or blocks most other pathogens. Additionally, the trophozoites actively feed on and destroy brain tissue (causing haemorrhagic necrosis) rather than causing damage solely through a slower immune-mediated inflammatory process.
- No — this is not a valid concern. Naegleria fowleri infection occurs only through nasal entry, with the organism travelling along the olfactory nerve to the brain. Swallowing contaminated water does not cause infection, since there is no pathway from the gastrointestinal tract to the brain for this organism.
- No. Cysts are not seen in brain tissue or CSF during active Naegleria fowleri infection — only trophozoites are found in these specimens. A report describing only cysts in CNS material should prompt reconsideration of the diagnosis rather than confirm it.
- Naegleria fowleri causes a much faster, more fulminant disease (PAM), typically affecting healthy children and young adults after acute freshwater exposure, with death often within a week. Acanthamoeba causes a slower, more indolent CNS infection (granulomatous amebic encephalitis), typically in immunocompromised individuals, and Acanthamoeba additionally causes amoebic keratitis in contact lens wearers — a distinct clinical entity not seen with Naegleria.
- Because the specific and only confirmed route of Naegleria fowleri infection is via the nose, not through general water contact or ingestion. Targeting nasal water entry specifically (nose clips, avoiding submersion of the head, avoiding diving in warm freshwater) addresses the actual mechanism of transmission, allowing public health guidance to prevent the disease without requiring unnecessary, overly broad avoidance of freshwater recreation in general.
References
- Clinical Microbiology Procedures Handbook (4th ed.). ASM Press. https://doi.org/10.1128/9781683670438.CMPH.ch9.9
- Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Foodborne, Waterborne, and Environmental Diseases (DFWED).
- Color Atlas and Textbook of Diagnostic Microbiology, Koneman (5th ed.).
- Gharpure, R., Bliton, J., Goodman, A., Ali, I. K., Yoder, J., & Cope, J. R. (2021). Epidemiology and clinical characteristics of primary amebic meningoencephalitis caused by Naegleria fowleri: a global review. Clinical Infectious Diseases, 73(1), e19–e27. https://doi.org/10.1093/cid/ciaa520
- CDC. (2024). Successful treatment of confirmed Naegleria fowleri primary amebic meningoencephalitis. Emerging Infectious Diseases, 30(4). https://wwwnc.cdc.gov/eid/article/30/4/23-0979_article
- Cope, J. R., Murphy, J., Kahler, A., et al. (2023). Fatal case of splash pad-associated Naegleria fowleri meningoencephalitis — Pulaski County, Arkansas, September 2023. MMWR Morbidity and Mortality Weekly Report, 74(10). https://www.cdc.gov/mmwr/volumes/74/wr/mm7410a2.htm
- Linam, W. M., Ahmed, M., Cope, J. R., et al. (2015). Successful treatment of an adolescent with Naegleria fowleri primary amebic meningoencephalitis. Pediatrics, 135(3), e744–e748. https://doi.org/10.1542/peds.2014-2292
- Centers for Disease Control and Prevention. Naegleria fowleri — Prevention & Control. https://www.cdc.gov/naegleria/prevention/index.html
Frequently Asked Questions
How does Naegleria fowleri infect the brain?
Why is primary amebic meningoencephalitis (PAM) so often fatal?
How can Naegleria fowleri infection be prevented?
What is the treatment for Naegleria fowleri infection?
What is the difference between Naegleria fowleri and Acanthamoeba infections?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.