Hookworm (Ancylostoma duodenale and Necator americanus): Life Cycle, Pathogenesis, and Lab Diagnosis
Why does a skin-penetrating larva cause iron-deficiency anemia months later? Complete hookworm life cycle, species comparison, clinical manifestations by site, and laboratory diagnosis with exam-ready tables.
A 6-year-old girl in a rural farming community presents with pallor, lethargy, and poor concentration at school. Her haemoglobin is 7.2 g/dL — severe anemia. There is no history of visible blood loss, no melena, no haematuria. Her mother mentions the child often plays barefoot in the fields near where the family practises open defecation.
The connection between bare feet in contaminated soil and severe anemia months later is not obvious and that is exactly why hookworm remains one of the most underdiagnosed causes of iron-deficiency anemia in children worldwide. A larva no more than half a millimetre long penetrates intact skin, migrates silently through the bloodstream and lungs, and ultimately attaches to the small intestine where it feeds on blood for years. Understanding this journey — from soil to skin to gut — is what allows a clinician to recognise hookworm disease in a patient who has never knowingly been "bitten" by anything.
Hookworm species have a worldwide distribution, with two species known to infect humans: Ancylostoma duodenale and Necator americanus. They are the second most common helminthic infection reported in humans. Other soil-transmitted helminths, roundworm (Ascaris lumbricoides) and whipworm (Trichuris trichiura) are the first and second most prevalent helminthic infections.
The greatest number of hookworm cases occur in Asia, followed by sub-Saharan Africa. N. americanus is the most common hookworm worldwide, whereas A. duodenale is more geographically restricted. Iron-deficiency anemia and protein-energy malnutrition from blood loss are the two major manifestations of hookworm infections.
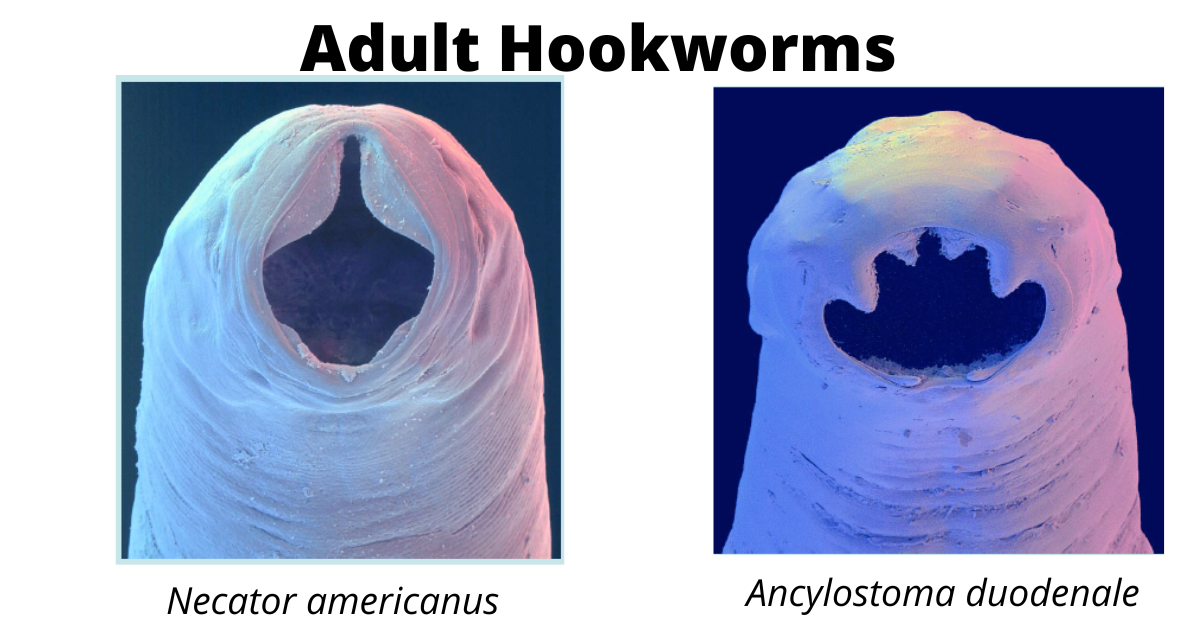 Figure: Hookworm
Figure: Hookworm
The eggs and rhabiditiform larvae of the two species are indistinguishable. Differentiation of the species is based on the morphology of the buccal capsule and the adult male copulatory bursa.
Why Hookworm Causes Anaemia: The Mechanism
Hookworm disease is fundamentally a disease of chronic, low-grade intestinal blood loss, and understanding the mechanism explains both the clinical presentation already described in this article and why species matters.
Adult worms attach to the intestinal mucosa using either teeth (A. duodenale) or cutting plates (N. americanus) and feed directly on blood. Each worm causes continuous microhaemorrhage at its attachment site, and worms also secrete anticoagulant proteins that prevent the bite wound from clotting, prolonging blood loss even after the worm moves to a new attachment site.
The blood loss is per-worm and cumulative. A single worm causes a small, almost negligible amount of blood loss. But infections are rarely caused by a single worm — they accumulate over months to years of repeated soil exposure, and the cumulative effect of hundreds of worms, each independently causing chronic microhaemorrhage, is what produces the iron-deficiency anemia described in the Hematologic row of the clinical manifestations table above.
Why species matters for severity: A. duodenale causes substantially more blood loss per worm than N. americanus — clinical studies using PCR-based quantification have found A. duodenale infections cause 2 to 10 times more blood loss than equivalent N. americanus burdens. This is the biological basis for the blood loss figures already in the species comparison table (10–20 mL/day for A. duodenale vs 0.03 mL/day for N. americanus) — and it means a patient with A. duodenale infection is at higher risk of severe anemia even at a similar worm burden, despite A. duodenale's shorter lifespan.
Why children are hit hardest: Children have smaller iron reserves and higher iron requirements for growth, making them disproportionately vulnerable to the same worm burden that an adult might tolerate with only mild anemia. This is why hookworm-attributable iron-deficiency anemia is concentrated in pre-school and school-age children in endemic regions, with documented effects on growth and cognitive development — directly explaining the "Growth and Mental Retardation" consequence already listed in this article.
Life Cycle
Hookworms are found in areas with moist, warm soil capable of supporting the parasite’s life cycle. Soil becomes infectious around 5-10 days after contamination and remains so for 3-4 weeks, depending on conditions.
Hookworm infection is mainly acquired by walking barefoot on contaminated soil through direct skin penetration by filariform larvae. Ancylostoma duodenale can also be transmitted through the ingestion of larvae.
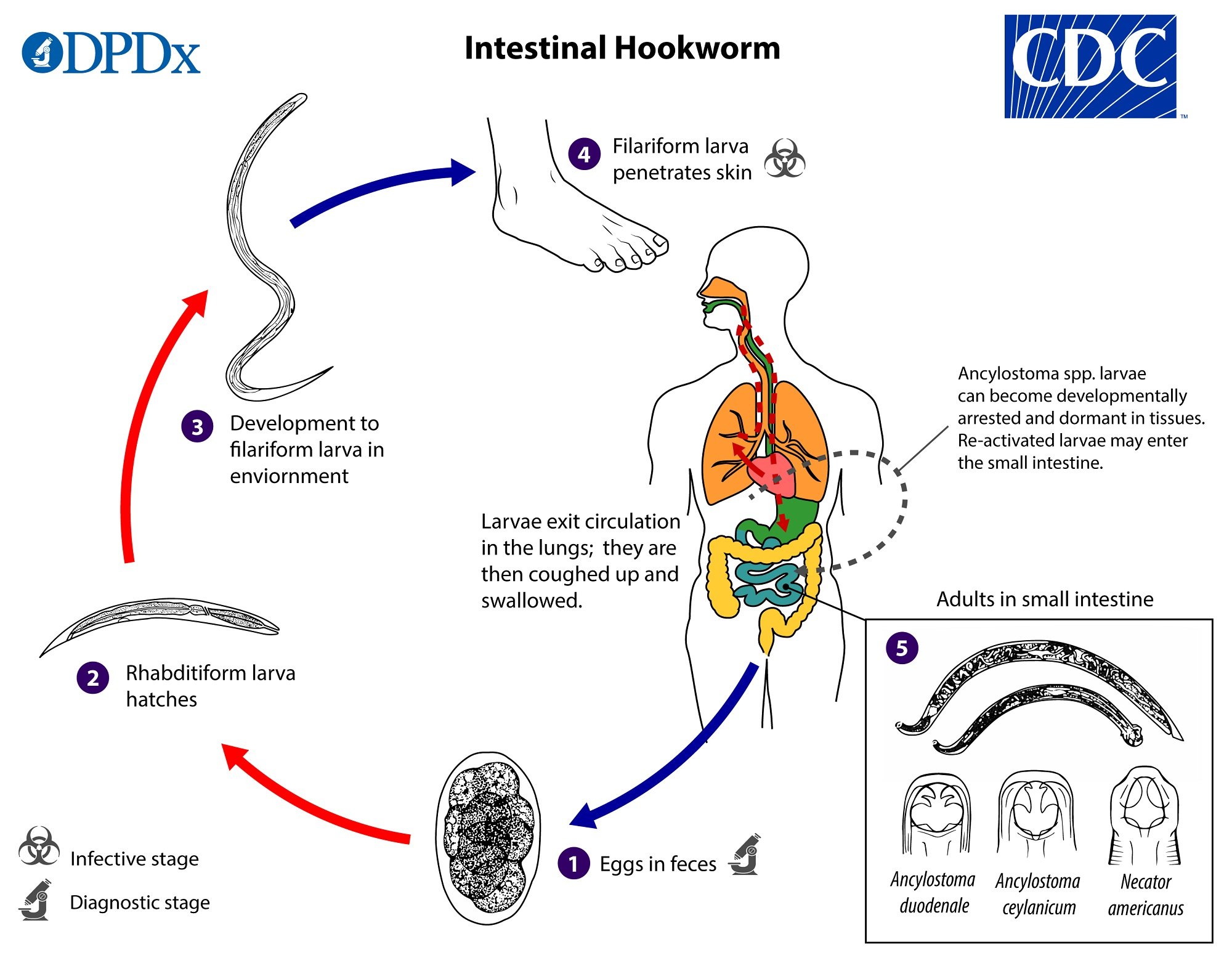 Figure: Life cycle of Hookworm (Image source: CDC)
Figure: Life cycle of Hookworm (Image source: CDC)
Eggs are passed in the stool.
If there is a practice of open defecation (defecation in fields, bushes, near water bodies, or other open spaces) or if the feces of infected persons are used as fertilizer, eggs get deposited on soil.
Under favorable conditions (moisture, warmth, shade), larvae hatch in 1 to 2 days and become free-living in contaminated soil. These released rhabditiform larvae grow in the feces and/or the soil.
After 5 to 10 days (and two molts), the noninfective rhabdifiform larvae will mature into infective filariform larvae (third-stage larvae). These infective larvae can survive 3 to 4 weeks in favorable environmental conditions.
On contact with the human host, typically bare feet, the infective filariform larvae penetrate the skin and enter the circulation.
Humans acquire hookworm when third-stage infective larvae in soil either penetrate the skin (as do both N. americanus and A. duodenale) or when they are ingested (A. duodenale only).
Larvae exit circulation in the lungs coughed up and swallowed. Reach intestine, mature, and lay eggs.
The larvae are carried through the blood vessels to the heart. The larvae can break through the capillaries and enter the host’s lungs. They penetrate the pulmonary alveoli, migrate up the bronchial tree to the pharynx, and are swallowed.
Upon entering the digestive system, the larvae attach to the mucosa of the small intestine. Here they secrete anticoagulants, ingest blood as their source of nourishment, and mature into adults. Adult worms live in the lumen of the small intestine, typically the distal jejunum.
The worms mature, and eggs are passed in the feces. About 5 weeks after infection, the worms attain sexual maturity, fertilization occurs, and females lay eggs that are passed along with the feces. Each female hookworm can lay 15000 – 20000 eggs per day.
Most adult worms are eliminated in 1 to 2 years, but the longevity may reach several years.
Clinical Manifestations
Most people infected with hookworms have no symptoms, but some may develop epigastric pain, diarrhea, anorexia, and eosinophilia. People who are infected for the first time may have gastrointestinal symptoms. Repeated exposure to third-stage larvae of hookworm results in a local pruritic, erythematous, papular rash known as “ground itch” at the site of larval penetration.
Two severe consequences of hookworm infections are;
- Anemia: The most serious effects of hookworm infection are blood loss, anemia, and protein loss.
- Growth and Mental Retardation: When many worms continuously infect children, the loss of iron and protein can retard growth and mental development.
Major clinical features of hookworm infections are tabulated here:
| Site | Symptoms | Pathogenesis |
|---|---|---|
| Dermal | Local erythema, macules, papules (ground itch) Creeping eruption | Cutaneous invasion and subcutaneous migration of larva |
| Pulmonary | Bronchitis, pneumonitis, and, sometimes, eosinophilia | Migration of larvae through lung, bronchi, and trachea |
| Gastrointestinal | Anorexia, epigastric pain, and gastrointestinal hemorrhage | Attachment of adult worms and injury to the upper intestinal mucosa |
| Hematologic | Iron deficiency, anemia, hypoproteinemia, edema, cardiac failure | Intestinal blood loss |
Laboratory Diagnosis
Sample: Stool, duodenal content, blood (to ascertain the nature of anemia and the presence of eosinophilia)
Microscopy
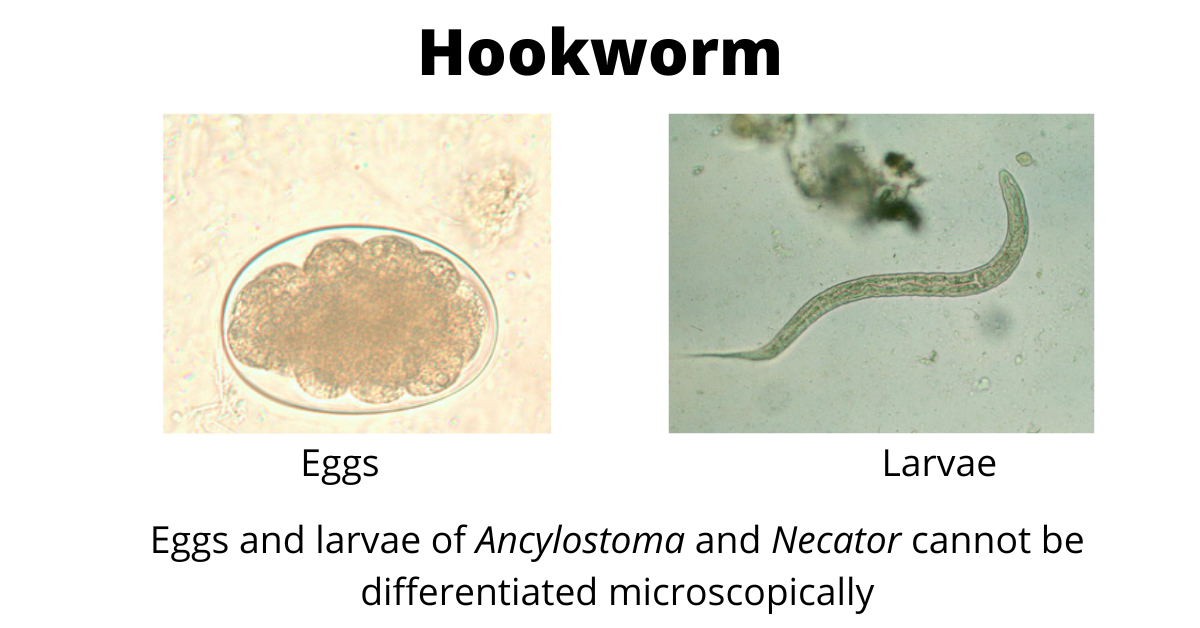
Hookworms are typically diagnosed by eggs or rhabditiform larvae found in stool specimens. Finding hookworm eggs on direct stool smear is problematic in light infections, so the concentration method is recommended. Ether concentration, FLOTAC, and Kato-Katz techniques are used to increase the diagnosis of hookworm infections. Species of hookworms cannot be distinguished by egg or larvae morphology. The eggs and larvae of the two species are indistinguishable.
 Eggs
Eggs
The eggs are oval, thin-shelled, and contain a visible four-eight stage embryo. There is a characteristic clear space between the shell and the developing embryo.
Larvae
The rhabditiform larvae are typically 250 to 300 μm with a long buccal capsule and an inconspicuous genital primordium. The larger filariform larvae are approximately 500 μm, with a pointed tail and an esophageal-to-intestinal ratio of 1:4. The rhabiditiform and filariform larvae must be differentiated from S. stercoralis.
Adults
Adult female hookworms measure up to 15 mm and males up to 10 mm in length. The anterior end is bent slightly dorsally, hence called hookworm. The mouth is large, and buccal capsule is equipped with four teeth on the ventral surface and a pair of smaller teeth on its dorsal surface
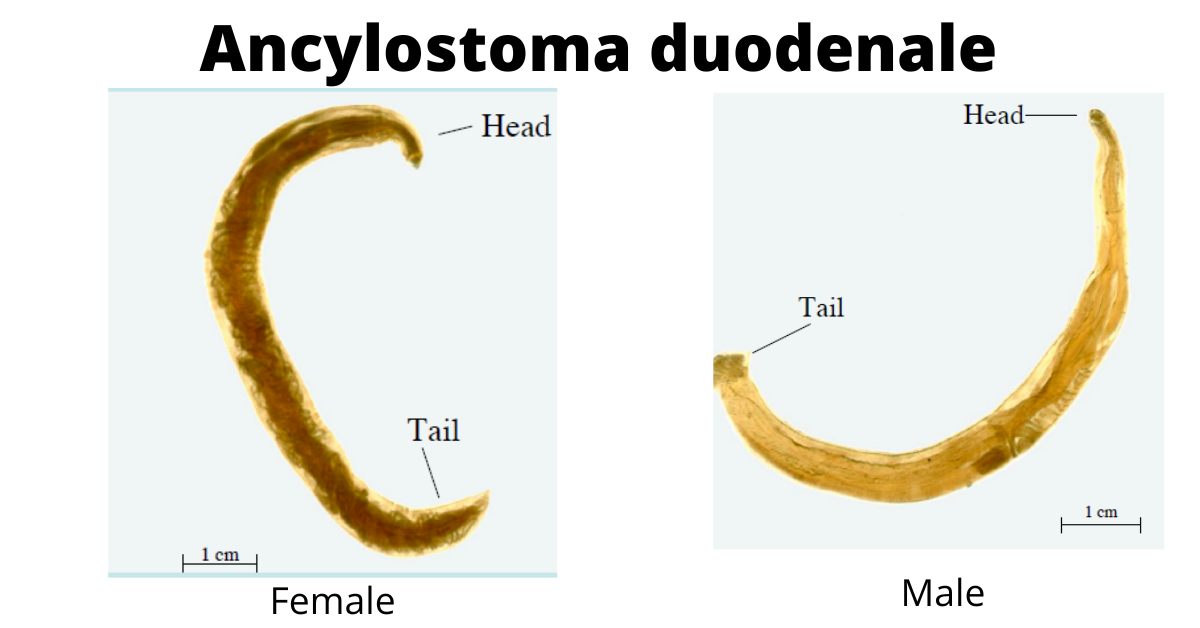 Figure: Female (left) and male (right) Ancylostoma duodenale
Figure: Female (left) and male (right) Ancylostoma duodenale
- Male: the posterior end is expanded into a copulatory bursa containing two copulatory spicules supported by fleshy rays. The expanded umbrella-like pattern of the posterior end is the characteristic feature of the male worm.
- Female: the hind end is coiled with a subterminal anus situated ventrally
Harada-Mori culture
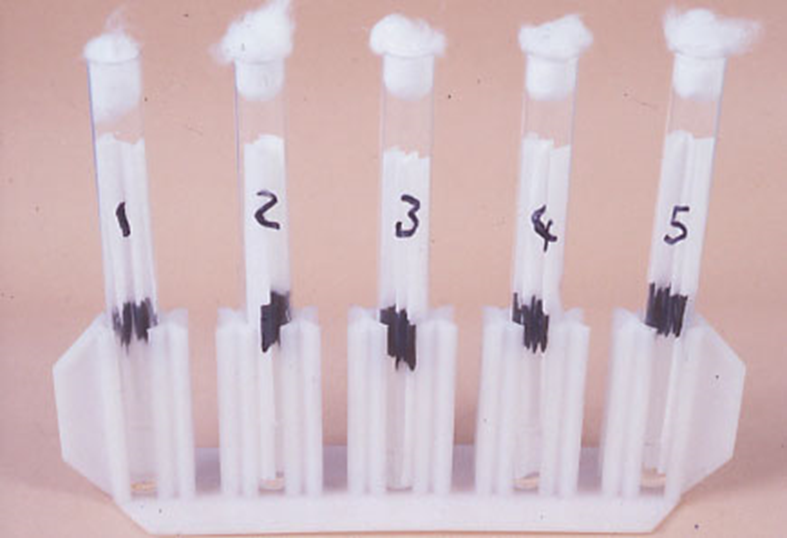 Figure: Harada-Mori culture
Figure: Harada-Mori culture
Rearing filariform larvae in a fecal smear on a moist filter paper strip for 5 to 7 days) to identify the species of nematode involved.
Treatment
Anthelmintic agents — albendazole (400 mg single dose) or mebendazole (500 mg single dose, or 100 mg twice daily for 3 days) — are the standard treatment. Iron supplementation is required in patients with significant anemia, and may need to continue for months to fully replenish iron stores even after the worms are cleared.
Important caution — co-infection with Strongyloides stercoralis: Because hookworm and Strongyloides share the same soil-transmission route and often co-exist in the same endemic populations, clinicians should consider co-infection, particularly before prescribing corticosteroids or other immunosuppressive therapy. Unlike hookworm, Strongyloides can cause life-threatening hyperinfection syndrome in immunosuppressed patients, and the standard hookworm treatment (benzimidazoles) is not the preferred treatment for Strongyloides — ivermectin is preferred. Empirically treating presumed hookworm with albendazole in a patient who also has unrecognised Strongyloides does not adequately address the more dangerous co-infection.
Prevention
Avoid contaminated soil (places with open defecation) and beaches. When traveling to a potentially contaminated area, wear appropriate footwear, such as enclosed shoes, and avoid other skin-to-soil contact forms. Communities can be protected by implementing effective sewage disposal systems. Currently, no preventive vaccine exists.
Types of Hookworms
Necator americanus and Ancylostoma duodenale are the significant hookworm species responsible for >90% of cases. Other species that can also cause infections are Ancylostoma ceylanicum, Ancylostoma braziliense, and Ancylostoma caninum.
Ancylostoma duodenale
Ancylostoma duodenale, Old World hookworm, is prevalent in southern Europe, Northern Africa, Southeast Asia, and South America. They attach to the intestinal mucosa by well-developed mouthparts, especially teeth.
Necatar americanus
Necatar americanus, New World hookworm, is prevalent in Africa, Southeast Asia, South and Central America, and the southeastern United States. They attach to the intestinal mucosa by well-developed cutting plates.
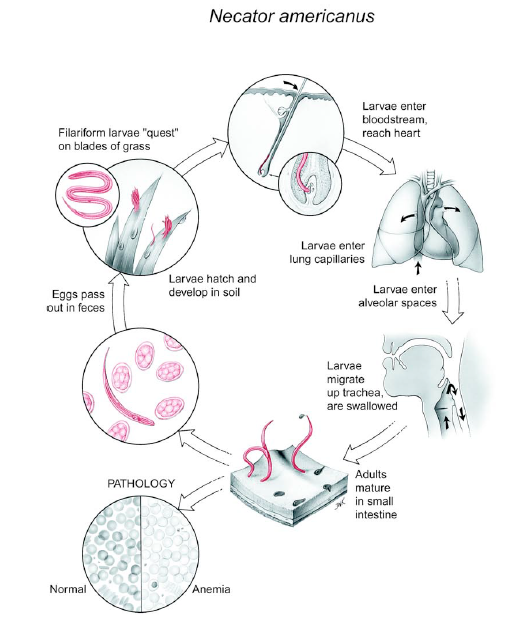 Figure: The Life cycle of Necator americanus
Figure: The Life cycle of Necator americanus
Differences between *Ancylostoma duodenale* and *Necator Americanus*
| Ancylostoma duodenale | Necator americanus | |
|---|---|---|
| Size | Longer | Shorter |
| Blood loss | 10.20 mL/day | 0.03 mL/day |
| Life Span | 1-2 years | 3-5 years or more |
| Egg production | 10,000 to 25000 /day | 5000 to 10,000/day |
| Mode of Transmission | Skin penetration and ingestion | Skin penetration only |
| Buccal capsule | Ancylostoma contains sharp teeth. | Necator contains cutting plates. |
Where Students Actually Get Confused
1. "Hookworm is only transmitted by skin penetration." This is true for Necator americanus, but Ancylostoma duodenale can also be transmitted by ingestion of larvae (e.g., on contaminated vegetables or in water) — this is reflected in the comparison table's "Mode of Transmission" row, but the distinction is easy to miss. This dual route is a commonly tested point distinguishing the two species.
2. "Rhabditiform and filariform larvae are interchangeable terms for hookworm." They represent different developmental stages with different significance. Rhabditiform larvae are the non-infective, feeding form found in stool and soil shortly after eggs hatch. Filariform (L3) larvae are the infective, non-feeding form that develops after 5–10 days and two moults in the environment — this is the form capable of skin penetration, as already described in the life cycle above. Finding rhabditiform larvae in a stool sample confirms infection but is not the form responsible for transmission to new hosts.
3. "Hookworm larvae can be distinguished from Strongyloides larvae by size alone." The article notes that hookworm rhabditiform and filariform larvae "must be differentiated from S. stercoralis" but does not explain how. The key distinguishing feature: hookworm rhabditiform larvae have a long buccal cavity (already stated in the article's larvae description), while Strongyloides rhabditiform larvae have a short buccal cavity — this is the primary differentiating feature on direct microscopy. Additionally, Strongyloides larvae have a more prominent genital primordium. Misidentifying Strongyloides as hookworm has real consequences — see the treatment caution above.
4. "Eggs of A. duodenale and N. americanus can be told apart under the microscope." They cannot — the article correctly states this, but it's worth emphasising as an exam point: hookworm eggs and rhabditiform larvae of the two species are morphologically indistinguishable. Species differentiation requires examining the buccal capsule (teeth in Ancylostoma vs cutting plates in Necator) of recovered adult worms, or Harada-Mori culture to rear filariform larvae for morphological comparison, or molecular methods (PCR).
5. "A heavy hookworm burden always causes obvious symptoms." Most infections are asymptomatic, particularly light infections, as already noted in the article. Iron-deficiency anemia develops gradually and silently over months as cumulative blood loss outpaces iron intake — a patient can have a clinically significant worm burden with no symptom beyond fatigue and pallor, which are easily attributed to other causes. This is precisely why hookworm is underdiagnosed: there is no acute, obviously infectious presentation pointing to the diagnosis.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Two major species | Ancylostoma duodenale, Necator americanus | >90% of cases combined |
| Global burden | ~500–740 million infected; up to 4.1 million DALYs/year | Leading cause of NTD morbidity |
| Infective stage | Filariform (L3) larva | Active skin penetration |
| Transmission: N. americanus | Skin penetration ONLY | "New World hookworm" |
| Transmission: A. duodenale | Skin penetration AND ingestion | Dual route — exam trap |
| Buccal capsule: Ancylostoma | Teeth (sharp) | "Ancylostoma bites" |
| Buccal capsule: Necator | Cutting plates | "Necator cuts" |
| Blood loss per worm: A. duodenale | 10–20 mL/day; 2–10× more than Necator | Higher anemia risk despite shorter lifespan |
| Blood loss per worm: N. americanus | 0.03 mL/day | Lower per-worm loss, but longer-lived |
| Lifespan: A. duodenale | 1–2 years | Shorter-lived |
| Lifespan: N. americanus | 3–5 years or more | Longer-lived |
| Egg output (overall) | 15,000–20,000 eggs/day per female | Species-specific rates also in comparison table |
| Time to sexual maturity | ~5 weeks after infection | Matches comparison table data |
| "Ground itch" | Local pruritic rash at site of larval skin penetration | First clinical sign |
| Pulmonary phase | Bronchitis, pneumonitis, eosinophilia | Larvae transit through lungs en route to intestine |
| Two severe consequences | Iron-deficiency anemia; growth/cognitive impairment in children | Cumulative chronic blood loss |
| Diagnosis | Stool eggs/larvae; concentration methods recommended for light infections | Direct smear insufficient for light infections |
| Species differentiation | NOT possible by egg/larva morphology | Requires adult buccal capsule or Harada-Mori culture |
| Must differentiate from | Strongyloides stercoralis larvae | Long buccal cavity (hookworm) vs short (Strongyloides) |
| Treatment | Albendazole or mebendazole + iron supplementation | Check for Strongyloides co-infection first |
Self-Check Questions
- A patient has chronic fatigue and a haemoglobin of 8 g/dL with no history of visible bleeding. Stool examination reveals hookworm eggs. Explain the mechanism connecting the infection to the anemia.
- Which hookworm species can be transmitted by ingestion in addition to skin penetration, and why is this an important distinction?
- A stool sample shows rhabditiform larvae with a long buccal cavity. How does this differ from what you would see with Strongyloides stercoralis, and why does the distinction matter clinically?
- A patient with suspected hookworm infection is about to start long-term corticosteroid therapy. What additional consideration is important before starting treatment, and why?
- Explain why Ancylostoma duodenale infection carries a higher risk of severe anemia than an equivalent worm burden of Necator americanus, despite A. duodenale having a shorter lifespan.
- Using the life cycle described in this article, explain why a patient might present with respiratory symptoms weeks after walking barefoot on contaminated soil.
Answers
- Adult hookworms attach to the intestinal mucosa using teeth or cutting plates and feed directly on blood, while also secreting anticoagulant proteins that prolong bleeding from each attachment site. This causes chronic, low-grade intestinal blood loss that accumulates across the worm burden over months, depleting iron stores faster than dietary intake can replace them, ultimately producing iron-deficiency anemia.
- Ancylostoma duodenale can be transmitted by ingestion of larvae as well as skin penetration, unlike Necator americanus, which is transmitted only by skin penetration. This distinction matters because it affects exposure risk assessment — a patient could acquire A. duodenale infection through contaminated food or water even without direct soil-to-skin contact, a route not available for N. americanus.
- Hookworm rhabditiform larvae have a long buccal cavity, while Strongyloides stercoralis rhabditiform larvae have a short buccal cavity — this is the key microscopic distinguishing feature. The distinction matters clinically because Strongyloides, unlike hookworm, can cause life-threatening hyperinfection syndrome in immunosuppressed patients, and the standard treatment differs (ivermectin preferred for Strongyloides vs benzimidazoles for hookworm).
- The patient should be evaluated for possible Strongyloides stercoralis co-infection before starting corticosteroids. Since hookworm and Strongyloides share the same soil-transmission route and often co-exist in the same populations, missing a Strongyloides co-infection before immunosuppression risks triggering hyperinfection syndrome, a potentially fatal complication that does not occur with hookworm alone.
- Ancylostoma duodenale causes 2 to 10 times more blood loss per worm than Necator americanus, based on PCR-quantified clinical studies, because its teeth and feeding mechanism cause greater mucosal damage and blood loss per attachment site compared to Necator's cutting plates. This higher per-worm blood loss outweighs the effect of its shorter lifespan, making A. duodenale infections more likely to produce severe anemia even at comparable worm burdens.
- This presentation is consistent with the pulmonary migration phase already described in the life cycle: after skin penetration, filariform larvae travel via the bloodstream to the heart, then to the lungs, where they break through the pulmonary capillaries into the alveoli before migrating up the bronchial tree to be coughed up and swallowed. This pulmonary transit causes bronchitis, pneumonitis, and eosinophilia, and the timing (weeks after exposure, before the larvae reach the intestine) corresponds to this migration period.
References and further readings
- Sastry, A. S., & Bhat, S. (2014). Essentials of Medical Parasitology. Jaypee Brothers Medical Publishers (P) Ltd.
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- Jonker, F. A., Calis, J. C., Phiri, K., Brienen, E. A., Khoffi, H., Brabin, B. J., Verweij, J. J., van Hensbroek, M. B., & van Lieshout, L. (2012). Real-time PCR demonstrates Ancylostoma duodenale is a key factor in the etiology of severe anemia and iron deficiency in Malawian pre-school children. PLOS Neglected Tropical Diseases, 6(3), e1555. https://doi.org/10.1371/journal.pntd.0001555
- Bartsch, S. M., Hotez, P. J., Asti, L., Zapf, K. M., Bottazzi, M. E., Diemert, D. J., & Lee, B. Y. (2016). The global economic and health burden of human hookworm infection. PLOS Neglected Tropical Diseases, 10(9), e0004922. https://doi.org/10.1371/journal.pntd.0004922
- Carroll, K. C. (Ed.), Pfaller, M. A. (Ed.). Ancylostoma. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK507898/
- World Health Organization. (2023). Soil-transmitted helminth infections. WHO Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections
- Loukas, A., Hotez, P. J., Diemert, D., Yazdanbakhsh, M., McCarthy, J. S., Correa-Oliveira, R., Croese, J., & Bethony, J. M. (2016). Hookworm infection. Nature Reviews Disease Primers, 2, 16088. https://doi.org/10.1038/nrdp.2016.88
Frequently Asked Questions
How does hookworm infection cause anemia?
What is the difference between Ancylostoma duodenale and Necator americanus?
Why does hookworm infection cause respiratory symptoms?
How is hookworm species identified if eggs look the same?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.