Helicobacter pylori: Properties, Pathogenesis, Virulence Factors, Diagnosis, and Treatment
Helicobacter pylori infects half the world's population and causes peptic ulcer disease and gastric cancer. Learn its properties (spiral GN rod, microaerophilic, urease-positive), virulence factors (CagA, VacA, urease, flagella), complete diagnostic tests (UBT, stool antigen, RUT, culture), and eradication treatment regimens.
In 1984, an Australian physician named Barry Marshall did something extraordinary. Unable to convince the medical establishment that a bacterium — not stress or spicy food — caused peptic ulcers, he drank a culture of Helicobacter pylori broth himself. Within days he developed gastritis. He treated himself with antibiotics and recovered. He and his colleague Robin Warren received the Nobel Prize in Physiology or Medicine in 2005.
That experiment overturned decades of medical dogma and established one of the most important principles in modern gastroenterology: peptic ulcer disease is an infectious disease, caused by a bacterium, and curable with antibiotics. Before Marshall and Warren's discovery, peptic ulcers were treated with antacids for life. Now, eradicating H. pylori cures the ulcer permanently.
Helicobacter pylori infects approximately 44% of the global population — but prevalence varies enormously: 70–90% in South Asia, Sub-Saharan Africa, and Latin America versus 20–40% in high-income countries. Most infections are acquired in childhood and persist lifelong without treatment. The organism causes gastritis in virtually everyone it colonises, but clinical disease depends on where in the stomach it establishes — and on which virulence factors it carries.
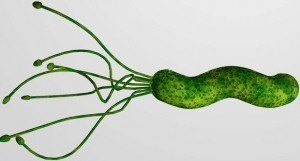 Figure: Helicobacter pylori
Figure: Helicobacter pylori
General Properties
Helicobacter pylori is:
- Gram-negative spiral (helical) rod — S-shaped or curved; 0.3–0.5 µm × 1.5–5 µm
- Microaerophilic — requires 5% O₂, 10% CO₂; cannot grow in ambient air or anaerobic conditions
- Highly motile — 4–6 unipolar sheathed flagella; corkscrew motility enables penetration of the viscous gastric mucus layer
- Urease-positive — produces large amounts of urease; the basis of the urea breath test and rapid urease test
- Oxidase-positive, catalase-positive
- Fastidious — slow-growing (3–7 days); requires enriched selective media (Skirrow's, Columbia blood agar); microaerophilic atmosphere
- Strict human pathogen — no significant animal reservoir; transmitted human-to-human via fecal-oral or oral-oral routes
Why H. pylori can survive the stomach: The gastric mucosa is an extremely hostile environment — pH 1–2, constant acid secretion, peristaltic movement. H. pylori survives by:
- Burrowing into the protective mucus layer (flagella-driven motility)
- Neutralising local acid with urease-generated ammonia
- Adhering to gastric epithelial cells via specific adhesins
These survival mechanisms are also its primary virulence factors.
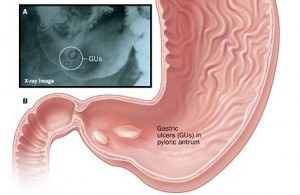 Figure: Gastric ulcer
Figure: Gastric ulcer
Epidemiology and Transmission
H. pylori is one of the most prevalent bacterial infections globally, with an estimated 44% of the world's population infected. Prevalence shows a strong inverse correlation with socioeconomic development:
| Region | Estimated prevalence |
|---|---|
| Sub-Saharan Africa | 70–90% |
| South Asia (India, Nepal, Bangladesh) | 60–80% |
| Latin America | 60–70% |
| East Asia | 50–70% |
| Eastern Europe | 40–60% |
| Western Europe, North America, Australia | 20–40% |
Transmission routes:
- Fecal-oral: Contaminated water and food are the primary transmission routes in high-prevalence settings; infection commonly occurs in early childhood
- Oral-oral: Transmission via saliva has been documented; gastric-oral transmission (via vomiting) is possible
- Iatrogenic: Endoscopes and pH electrodes have caused transmission in healthcare settings if inadequately sterilised
Age of acquisition: Most infections occur in early childhood (before age 10) in high-prevalence settings. Once acquired, the infection persists indefinitely without treatment. The high prevalence in Nepal, India, Nigeria, and the Philippines directly reflects the socioeconomic conditions in which most of the site's audience works and studies.
Pathogenesis: From Infection to Disease
H. pylori colonisation causes chronic gastric inflammation (chronic active gastritis) in virtually all infected individuals. Whether this progresses to clinical disease depends on three factors: where in the stomach the organism colonises, which virulence factors it carries, and host genetic factors.
The critical distinction — antrum vs corpus:
| Colonisation pattern | Gastric acid effect | Disease outcome |
|---|---|---|
| Antrum-predominant | Increased acid secretion (inhibits somatostatin, stimulates gastrin) | Duodenal ulcer |
| Corpus-predominant | Decreased acid (corpus inflammation → atrophy → reduced parietal cell mass) | Gastric ulcer; gastric cancer; MALT lymphoma |
| Pangastritis | Variable | Gastric cancer risk highest |
The H. pylori disease spectrum — from colonisation to carcinoma:
H. pylori infection
↓
Chronic active gastritis (universal)
↓
├─── Antrum-predominant → Duodenal ulcer (10–15% of infected)
│
├─── Corpus/pangastritis → Gastric ulcer (3–5%)
│
├─── Atrophic gastritis → Intestinal metaplasia → Dysplasia → Gastric adenocarcinoma
│ (the Correa cascade — decades-long process)
│
└─── Gastric MALT lymphoma (rare but treatable — eradication alone cures 60–90% of early cases)
H. pylori as a Group I carcinogen: The WHO/IARC has classified H. pylori as a definite (Group I) human carcinogen — the only bacterium with this classification. It accounts for approximately 90% of non-cardia gastric cancers globally, making it the single most preventable cause of cancer death worldwide. Eradicating H. pylori in populations with high prevalence is one of the most impactful cancer prevention strategies available.
Virulence Factors of Helicobacter pylori
Not all H. pylori strains cause the same disease. The clinical outcome is determined largely by which virulence genes the infecting strain carries.
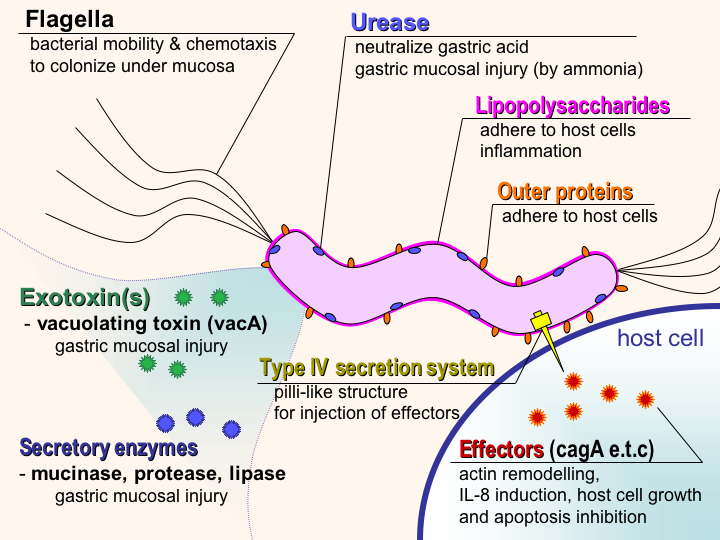 Figure: Schematic diagram of virulence factors of Helicobacter pylori
Figure: Schematic diagram of virulence factors of Helicobacter pylori
1. Urease — The Survival Factor
Urease is the most important virulence factor for establishing infection:
- Metabolises urea → ammonia (NH₃) + CO₂
- Ammonia neutralises gastric acid around the organism, creating a survivable microenvironment
- Directly toxic to gastric epithelium at high concentrations
- Diagnostic basis: Urease activity is detected by the urea breath test and the rapid urease test (CLO test) — both rely on this unique biochemical property
- All pathogenic H. pylori strains produce urease — it is not a strain-variable factor
2. Flagella — Motility and Mucus Penetration
- 4–6 unipolar sheathed flagella provide corkscrew motility
- Enable penetration of the thick viscous gastric mucus layer — essential for reaching the epithelial surface
- Flagellin is coated by a sheath derived from the outer membrane, hiding it from TLR5 (the flagellin pattern recognition receptor) — a mechanism for avoiding innate immune detection
- Non-motile mutants cannot colonise the stomach
3. CagA (Cytotoxin-Associated Gene A) and the Type IV Secretion System
CagA is the most important virulence factor for cancer risk:
- CagA is a bacterium-derived oncoprotein encoded on the cagPAI (cag pathogenicity island) — a 40-kb genomic island present in approximately 60–70% of Western strains and >90% of East Asian strains
- Delivered directly into host gastric epithelial cells via the Type IV Secretion System (T4SS) — a molecular syringe analogous to a hypodermic needle
- Once injected, CagA undergoes tyrosine phosphorylation by host kinases and activates multiple oncogenic signalling pathways:
- Disrupts cell polarity and tight junctions
- Activates Ras-MEK-ERK and PI3K-Akt pathways
- Inhibits tumour suppressor pathways
- Facilitates malignant transformation of gastric epithelial cells
- CagA also triggers NF-κB activation → IL-8 secretion → intense neutrophilic inflammation
- Clinical implication: CagA-positive strains are associated with significantly higher risk of peptic ulcer disease and gastric cancer compared to CagA-negative strains
4. VacA (Vacuolating Cytotoxin)
VacA is a secreted pore-forming toxin produced by all H. pylori strains but with variable activity:
- Induces vacuole formation in gastric epithelial cells (hence "vacuolating")
- Forms anion-selective channels in host cell membranes → disrupts membrane potential
- Triggers cytochrome c release from mitochondria → apoptosis of gastric epithelial cells
- Immunosuppressive: Inhibits T-cell activation and proliferation by targeting the T-cell receptor/NFAT pathway — allows the organism to persist despite immune responses
- VacA activity varies by allele type: s1/m1 alleles are most cytotoxic; s2/m2 strains produce inactive VacA
5. Adhesins — BabA and Others
H. pylori adhesins mediate specific attachment to gastric epithelial cells:
- BabA (Blood group antigen binding adhesin): Binds Lewis b (Le^b^) blood group antigens on gastric epithelial cells; high adherence to gastric mucosa; associated with increased peptic ulcer and gastric cancer risk
- OipA (Outer Inflammatory Protein A): Induces IL-8 secretion and actin dynamics; promotes inflammation through CagPAI-related pathways; associated with duodenal ulcer risk
- HopQ: Interacts with CEACAM receptors; facilitates CagA delivery via T4SS
6. DupA (Duodenal Ulcer Promoting Gene)
- Strains with a complete dupA gene cluster have 2.1-fold higher risk of duodenal ulcer
- Induces IL-8 production in the antrum → antrum-predominant gastritis → classic duodenal ulcer pattern
Virulence Factor Summary
| Factor | Function | Cancer risk association |
|---|---|---|
| Urease | Acid neutralisation; colonisation enabler | Present in all strains; essential for infection |
| Flagella | Mucus penetration; immune evasion | Present in all strains; essential for infection |
| CagA + T4SS | Oncoprotein injection; IL-8 inflammation | High — CagA+ strains: highest cancer risk |
| VacA | Cell vacuolation; apoptosis; T-cell suppression | Variable by allele; s1/m1 highest risk |
| BabA | Lewis b antigen adhesion | High — enhanced colonisation |
| OipA | IL-8 induction; inflammation | Duodenal ulcer risk |
| DupA | IL-8 antrum; antrum-predominant gastritis | Duodenal ulcer risk (not gastric cancer) |
Diagnosing H. pylori Infection
In order to optimize the diagnosis of H. pylori, it is usually recommended that several tests be used together. The choice of particular tests will depend on the locally available facilities, cost consideration, and clinical circumstances in which the diagnosis of H. pylori is made.
When to Test
H. pylori testing is indicated in:
- Active peptic ulcer disease (gastric or duodenal)
- History of peptic ulcer disease (to confirm eradication if not previously tested)
- Gastric MALT lymphoma
- Early gastric cancer (before or after endoscopic resection)
- Uninvestigated dyspepsia (test-and-treat strategy is recommended in high-prevalence settings)
- First-degree relatives of gastric cancer patients
The Two Categories — Non-Invasive vs Invasive
| Category | Test | Detects | Best use |
|---|---|---|---|
| Non-invasive | Urea Breath Test (UBT) | Active infection (urease activity) | Diagnosis and test-of-cure (preferred) |
| Non-invasive | Stool Antigen Test (SAT) | Active infection (H. pylori antigen in stool) | Diagnosis and test-of-cure (alternative to UBT) |
| Non-invasive | Serology (IgG) | Past or present infection | Epidemiology; not for test-of-cure |
| Invasive | Rapid Urease Test (CLO test) | Active infection at biopsy site | Endoscopy-based; rapid; inexpensive |
| Invasive | Histology | Active infection + gastric pathology | Gold standard; shows inflammation grade |
| Invasive | Culture + AST | Active infection + antibiotic susceptibility | Essential where clarithromycin resistance is high |
| Invasive | PCR | H. pylori DNA + resistance genes | Reference method; detects resistance mutations |
Serology: Serological tests that measure specific H. pylori IgG antibodies can determine if a person has been infected. The sensitivity and specificity of these assays range from 80% to 95% depending upon the assay used. A positive serology indicates present or past infection. A positive antibody screen should be confirmed by tests such as fecal antigen, urea breath test, or other invasive tests.
Urea breath test: In this test, the patient is given either 13C- or 14C-labeledureato ingest/drink (depending on the form; capsule or liquid). H. pylori metabolizes the urea rapidly, and the labeled carbon is absorbed into the blood and exhaled via the breath. This labeled carbon can then be measured as CO2 in the patient’s expired breath to determine whether H.pylori is present. The sensitivity and specificity of the breath test range from 94% to 98%.
Fecal antigen test (FAT):H. pylori stool antigen is a reliable noninvasive tool to screen H. pylori infection. The fecal antigen test identifies H. pylori antigen in the stool by enzyme immunoassay using polyclonal anti-H. pylori antibody.
Tests mentioned below require biopsy specimens of the stomach or duodenum. Test sample is taken during upper esophagogastroduodenal endoscopy.
- Microscopy: Histologic identification of organisms – considered the gold standard of diagnostic tests. Microscopy of gram-stained smears or imprints of gastric biopsies reveals curved gram-negative rods resembling Helicobacter.
- Culture: Culture of biopsy specimens for H. pylori requires sophisticated conditions. H. pylori can grow on different solid media containing blood or blood products (blood or lysed blood agar plates) **but requires a microaerophilic (less oxygen tolerance) bacteria. Culture is necessary to isolate agents to perform antimicrobial susceptibility testing.
- Rapid Urease Testing (RUT): Rapid Urease testing identifies active H. pylori infection through the organism’s urease activity. Gastric biopsies are obtained and placed into an agar gel or on a reaction strip containing urea, a buffer, and a pH-sensitive indicator. In the presence of H. pylori’s urease, urea is metabolized to ammonia and bicarbonate leading to a pH increase in the micro-environment of the organism. A change in color of the pH-sensitive indicator signifies the presence of active infection. Commercially available kits yield results in 1–24 h.
- Molecular Tests: PCR is a DNA amplification technique that utilizes the rapid production of multiple copies of a target DNA sequence to identify H. pylori. This testing method is highly specific and may be more sensitive than other biopsy-based diagnostic techniques.
Advantages and disadvantages of diagnostic testing for Helicobacter pylori
Test Methods | Advantage | Disadvantage |
Histology | Excellent Sensitivity and specificity | Expensive and requires infrastructure and trained personnel |
Rapid Urease Testing | Inexpensive and provides rapid results. Excellent specificity and very good sensitivity in properly selected patients. | Sensitivity significantly reduced in post- treatment setting |
Culture | Excellent specificity. Allows determination of antibiotic sensitivities. | Expensive, difficult to perform, and not widely available. |
Antibody testing (quantitative and qualitative) | Inexpensive, widely available, very good negative predictive value (NPV). | Positive predictive value (PPV) dependent upon background H. pylori prevalence. Not recommended after H.pylori therapy. |
Urea breath tests
| Identifies active H.pylori infection. Excellent PPV and NPV regardless of H.pylori prevalence. | |
Fecal antigen test
| Identifies active H.pylori infection. Excellent positive and negative predictive values regardless of H.pylori prevalence. Useful before and after H.pylori therapy. | Polyclonal test less well validated than the UBT in the post-treatment setting. Monoclonal test appears reliable before and after antibiotic therapy. Unpleasantness associated with collecting stool. |
Critical Rule: Serology Cannot Confirm Eradication
Serology (IgG antibodies) remains positive for 6–12 months after successful eradication. A positive IgG result after treatment does not indicate treatment failure — it represents persisting immunological memory. Only UBT or stool antigen test, performed ≥4 weeks after completing therapy and ≥2 weeks after stopping PPIs, reliably confirms eradication.
Treatment: Eradication of H. pylori
H. pylori eradication cures peptic ulcer disease (>90% of duodenal ulcers heal after eradication without ongoing acid suppression), reduces gastric cancer risk, and resolves early-stage MALT lymphoma in 60–90% of cases. The decision to treat should be based on confirmed active infection.
First-Line Regimens
Choice of regimen depends on local clarithromycin resistance rates:
| Regimen | Components | Duration | Use when |
|---|---|---|---|
| Clarithromycin triple therapy | PPI (standard dose BD) + clarithromycin 500 mg BD + amoxicillin 1g BD | 14 days | Clarithromycin resistance <15% in local population |
| Bismuth quadruple therapy | PPI BD + bismuth subsalicylate/subcitrate QID + metronidazole 500 mg TID + tetracycline 500 mg QID | 10–14 days | Clarithromycin resistance ≥15% OR penicillin allergy |
| Concomitant (non-bismuth quadruple) | PPI BD + clarithromycin 500 mg BD + amoxicillin 1g BD + metronidazole 500 mg BD | 14 days | Where both metronidazole and clarithromycin resistance are low |
For high-prevalence LMIC settings (South Asia, Africa, Southeast Asia): Clarithromycin resistance exceeds 15% in many of these regions, making bismuth quadruple therapy the preferred first-line regimen where bismuth is available. Where bismuth is not available, concomitant therapy is a reasonable alternative. Local resistance surveillance data should guide regimen choice.
Test-of-Cure
- Confirm eradication with UBT or stool antigen test — not serology
- Test ≥4 weeks after completing antibiotic therapy
- Test ≥2 weeks after stopping proton pump inhibitors (PPIs reduce urease activity, causing false-negative UBT/RUT results)
- If first-line eradication fails: re-treat with a different regimen (avoid repeating clarithromycin if first-line regimen contained it)
Rising Antibiotic Resistance
H. pylori antibiotic resistance is an increasing global concern:
- Clarithromycin resistance: 15–40% in many regions; dramatically reduces triple therapy efficacy
- Metronidazole resistance: 20–40% globally; impact is partial (quadruple therapy partially overcomes it)
- Fluoroquinolone resistance: Rising in Asia; second-line levofloxacin therapy affected
- Amoxicillin and tetracycline resistance: Rare; first-line agents remain reliably active
Culture with antimicrobial susceptibility testing is the only method to determine local and individual isolate resistance patterns. In settings with high treatment failure rates, culture-guided therapy is increasingly recommended.
How to Remember
The Nobel Prize story as the clinical anchor: Marshall drank H. pylori → developed gastritis → treated with antibiotics → cured. This experiment proved: PUD = infectious disease = curable with antibiotics. Before 1984: antacids for life. After 1984: 10-day antibiotic course. The discovery that changed gastroenterology is a built-in clinical hook for every student.
The antrum vs corpus rule:
- Antrum infection → more acid → Duodenal ulcer (think: acid Drives Duodenal ulcer)
- Corpus infection → less acid + atrophy → Gastric ulcer, Gastric cancer (think: Gastric Glandular damage)
CagA = cancer-associated gene A: The cag pathogenicity island encodes a molecular syringe (T4SS) that injects CagA oncoprotein directly into gastric cells. CagA activates oncogenic pathways from inside the cell — the bacteria never need to invade; they just inject their oncogene. CagA-positive strains → higher peptic ulcer AND cancer risk.
Urease as the foundation of all non-invasive tests: UBT: patient drinks labelled urea → urease splits it → labelled CO₂ in breath → positive RUT (CLO test): biopsy into urea medium → urease → pH change → colour change Both tests work because urease is unique to H. pylori in the stomach (no other gastric organism produces it in significant amounts)
The serology trap — never use for test-of-cure: IgG remains positive ≥6 months after eradication. "My serology is still positive" after treatment = immunological memory, not treatment failure. Use UBT or stool antigen, wait ≥4 weeks post-antibiotics and ≥2 weeks post-PPI.
The three reasons H. pylori is unique among bacteria:
- Only bacterium classified as a Group I carcinogen (WHO/IARC)
- Only infection where Nobel Prize was proven by self-experimentation
- Treatment of a chronic infection (not just suppression) prevents cancer
References
- Madigan Michael T, Bender, Kelly S, Buckley, Daniel H, Sattley, W. Matthew, & Stahl, David A. (2018). Brock Biology of Microorganisms (15th Edition). Pearson.
- Roberts, A. P., Childs, S. M., Rubin, G., & de Wit, N. J. (2000). Tests for Helicobacter pylori infection: a critical appraisal from primary care. Family practice, 17 Suppl 2, S12–S20. https://doi.org/10.1093/fampra/17.suppl_2.s12
- Atherton JC. H. pylori virulence factors. British Medical Bulletin. 1998;54(1):105–120.
- Kalali B et al. H. pylori Virulence Factors: Influence on Immune System and Pathology. Mediators of Inflammation. 2014.
- William G et al. Virulence factors of Helicobacter pylori. International Journal of Medical Microbiology. 2001;290(8):647–658.
- Chang WL, Yeh YC, Sheu BS. The impacts of H. pylori virulence factors on the development of gastroduodenal diseases. J Biomed Sci. 2018;25(1):68. doi:10.1186/s12929-018-0466-9
- Roesler BM et al. Virulence Factors of Helicobacter pylori: A Review. Clin Med Insights Gastroenterol. 2014;7:9–17.
- Malfertheiner P, et al. (European Helicobacter and Microbiota Study Group). Management of Helicobacter pylori infection — the Maastricht V/Florence Consensus Report. Gut. 2017;66(1):6–30. doi:10.1136/gutjnl-2016-312288 (The definitive European treatment guideline)
- Ford AC, et al. Helicobacter pylori eradication therapy to prevent gastric cancer. Lancet. 2020;395(10229):1113–1120.

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.