Giemsa Stain: Principle, Procedure, Results
Complete Giemsa staining guide; stock and working solution preparation, pH 7.2 buffer chemistry, thick/thin smear procedure, organism-specific results, and a troubleshooting table for common staining problems.
A laboratory technician in a busy district hospital stains a batch of thirty blood smears for malaria screening. Every smear comes back uniformly blue-grey — no clear differentiation, parasite morphology unreadable, Schüffner's dots impossible to confirm. She re-checks her reagents: the Giemsa stock is fresh, the dilution is correct. The problem turns out to be the buffered water; it was prepared with tap water instead of pH 7.2 phosphate buffer, and the local water supply runs alkaline.
This single variable — pH — is responsible for more failed Giemsa stains in field and resource-limited laboratories than any other factor. Understanding not just the staining steps but the chemistry behind them is what separates a technician who can follow a protocol from one who can troubleshoot it when results go wrong.
Giemsa stain is a type of Romanowsky stain named after Gustav Giemsa, a German chemist who created a dye solution. It was primarily designed for the demonstration of malarial parasites in blood smears, but it is also employed in histology for routine examination of blood smears.
Principle of Giemsa Stain
Giemsa stain is a differential stain and contains a mixture of azure, methylene blue, and eosin dye. It is specific for the phosphate groups of DNA and attaches itself to where there are high amounts of adenine-thymine bonding.
Azure and eosin are acidic dye that variably stains the basic components of the cells like the cytoplasm, granules, etc.
Methylene blue acts as the basic dye, which stains the acidic components, especially the nucleus of the cell.
Methanol act as a fixative as well as a cellular stain. The fixative does not allow a further change in the cells and makes them adhere to the glass slide.
Giemsa vs Wright vs Wright-Giemsa — what is the difference?
These three stains are frequently mentioned interchangeably in clinical and research settings, which causes significant confusion. Here is a clear distinction:
| Feature | Giemsa stain | Wright stain | Wright-Giemsa stain |
|---|---|---|---|
| Composition | Azure B + eosin Y + methylene blue in glycerol/methanol | Eosin Y + methylene azure B in methanol (no glycerol) | Combination of both Wright and Giemsa formulations |
| Fixative | Methanol (separate step for thin smears) | Methanol incorporated into stain (self-fixing) | Methanol incorporated |
| Staining time | Longer (45–60 min for slow method) | Shorter (2–5 min) | Intermediate |
| Malaria diagnosis | Preferred — gold standard | Less reliable for malaria parasites | Acceptable |
| Blood cell morphology | Good | Preferred in hematology labs | Excellent — best of both |
| Parasite detail | Superior — better for stippling (Schüffner dots, Maurer clefts) | Adequate | Very good |
| pH sensitivity | High — requires buffered water pH 7.2 | High — requires buffered water | High |
| WHO recommendation | Recommended for malaria diagnosis | Not specifically recommended | Acceptable alternative |
In practice: Wright stain is the standard in hematology for routine blood cell differential counts. Giemsa stain is the WHO-recommended method for malaria diagnosis and parasite detection. Wright-Giemsa combines advantages of both and is widely used in reference laboratories for both hematology and parasitology.
Preparation of Giemsa Stain
Giemsa is the most commonly used stain for staining blood films for malaria diagnosis. It is available commercially as a ready-to-use product, but the quality varies according to the source. By following simple rules, laboratories can prepare a stock solution of Giemsa stain using Giemsa stain powder, thus ensuring the use of consistent, high-quality stain.
Composition
The essential ingredients of Giemsa stain are the same; however, dilutions can be made depending on their use.
| Ingredients | Gm/L |
|---|---|
| Giemsa powder | 7.6 |
| Glycerol | 500 ml |
| Methanol | 500 ml |
Supplies, Materials, and equipment
- Giemsa powder or stain, 7.6 g (preferably Biological Stain Commission grade, to ensure a very good product of standard quality;
- absolute methanol, pure, high-grade, acetone-free, 500 mL;
- glycerol, high-grade, pure, 500 mL;
- methanol-cleaned solid glass beads, 3-5 mm in diameter, 50-100 pieces;
- a spatula or measuring spoon;
- weighing paper;
- a graduated cylinder;
- a glass or plastic funnel;
- a screw-capped, dark or amber glass bottle, clean and dry, 500-ml capacity (If not available, a chemically clean, dry, clear hard glass or polyethylene bottle of suitable size may be used, but should be wrapped in dark paper);
- an analytical balance capable of weighing to 0.01 g; and
- a shaker, if available.
Note:
- The person preparing the Giemsa stain should follow universal precautions, including the use of relevant personal protective equipment (PPEs) such as gloves, safety glasses, and a laboratory gown.
- Avoid contact and inhalation of methanol and Giemsa stain. Methanol and Giemsa stain are inflammable and highly toxic if inhaled or swallowed. Keep both chemicals in a locked cabinet or cupboard when they are not in use.
Preparation of Giemsa Stock Solution
Place about 100 methanol-cleaned glass beads into a dark or amber bottle.
Weigh 7.6 g of Giemsa stain powder on an analytical balance, and pour it into the bottle containing the beads through a funnel.
Gently pour about 200 mL of methanol, ensuring that all dry stain is washed into the bottle.
Tighten the screw cap on the bottle and shake it in a circular motion for 2-3 minutes to start dissolving the stain crystals.
Add 500 mL glycerol to the mixture through the funnel, and shake again for 3-5 minutes.
Add the remaining 300 mL of methanol to the mixture through the funnel, ensuring that the last of the methanol washes the last of the glycerol from the funnel into the stain mixture.
Tighten the screw-cap on the bottle.
The bottle should be tightly capped at all times to prevent absorption of water vapor and to avoid evaporation and oxidation of the stain by high humidity. If the bottle is tightly stoppered and free of moisture, the Giemsa stain is stable at room temperature for longer.
About six times on the first day, continue shaking for 2-3 minutes each.
Shake for at least seven days every day for 2-3 minutes, about six times each. A shaker may be used, if available.
Label the bottle clearly with the batch number, the name of the person who prepared the stock, date of preparation and date of expiry, and document in the quality control log-book.
Giemsa stock solution
Batch No.: 2022-01 Prepared by: First name Last name
Date prepared: 17 Aug 2022
Expiry date: 17 Aug 2024
#2022-01 indicates the year prepared and the stock number.Tighten the screw-cap on the bottle to prevent absorption of water vapor from the air, and store it in a cool place away from direct sunlight.
Do NOT contaminate the stock Giemsa solution with water; even the smallest amount of water will cause the stain to deteriorate, making staining progressively ineffective. Store in a dark glass bottle in a cool, dry, shady place, away from direct sunlight. If a clear stock bottle is used, wrap it in thick dark paper to avoid light penetration.
Working Solution of Giemsa Stain
Working solution of Giemsa stain should be freshly prepared from Giemsa stock solution. Depending upon the method of staining used to stain malaria blood films, the Giemsa working solution is either 10% (for the rapid method) or 3% (for the slow method).
A rapid method is used in outpatient clinics and busy laboratories where a quick diagnosis is essential for patient management, whereas a slow method is used for staining a large number of slides collected during epidemiological or field.
Rapid (10% working solution) method
- Commonest method for staining 1-15 slides at a time.
- Used in outpatient clinics and busy laboratories
- Efficient method but costly (as more stain is consumed)
Slow (3% working solution) method
- Used for staining a larger number of slides (>20)
- Ideal for staining blood films collected during cross-sectional or epidemiological surveys, field research, or for preparing batches of slides for teaching
- Time-consuming method, so less appropriate when a quick result is needed
- Less expensive compared to the rapid method as it requires much less stain.
Materials and Supplies
- Giemsa stain, transferred and filtered from the stock solution into a 25-or 50-ml bottle;
- buffered water, pH 7.2;
- a beaker or tube, clean, 5-10-ml capacity;
- a Pasteur pipette and
- Whatman filter paper, grade #1.
Preparation of Giemsa Working Solution
Prepare either 10% or 3% Giemsa working solution, depending on your need. About 3 mL of stain is required for each slide with a blood film.
- Place 90 mL of prepared buffered water, pH 7.2, into a clean beaker or tube.
- Filter the Giemsa stock solution through paper Whatman #1 and transfer it to a 25 to 50 mL container.
- Add 10 mL of Giemsa stock solution using a clean, dry pipette. Do not take the aliquot from the large bottle containing the Giemsa stock solution to avoid contaminating it.
- Prepare the Giemsa working solution just before staining the blood film(s), and use it within 15 minutes of preparation. Discard any unused stain.
To prepare 3% Giemsa working solution, follow the procedure mentioned above, but mix 97 mL of buffered water with 3 mL of Giemsa stock solution.
Quality Control
Run a known positive control slide (confirmed malaria-positive or a slide with known WBC differential) alongside new batches of stock or working solution, particularly:
- When a new batch of stock solution is first prepared
- When switching to a new lot or brand of Giemsa powder
- Periodically (weekly or per laboratory SOP) even with established stock
Document for each batch: date prepared, batch number, expiry date, and result of the control slide (pass/fail). The article's existing stock solution labelling example (Batch No., Prepared by, Date prepared, Expiry date) is good practice — extend the same documentation discipline to the working solution and to control slide results, not just the stock bottle.
Why pH 7.2 buffered water is critical
The pH of the water used to dilute Giemsa stain is one of the most important — and most commonly overlooked — variables in Giemsa staining. Giemsa staining is extremely pH-sensitive:
- Too acidic (pH below 6.8): Eosin staining dominates — RBCs appear orange-red, parasites stain poorly, Schüffner's dots and Maurer's clefts may not be visible
- Optimal (pH 7.0–7.2): Correct differential staining — RBCs appear mauve-pink, parasite nuclei red/pink, parasite cytoplasm blue, stippling clearly visible
- Too alkaline (pH above 7.4): Azure/methylene blue dominates — RBCs appear blue-grey, nuclei overstained, everything appears blue, parasite morphology obscured
Practical preparation of pH 7.2 buffered water:
Use commercially available phosphate buffer tablets (pH 7.2) dissolved in distilled water, or prepare from:
- Solution A: 9.47 g Na₂HPO₄ (dibasic sodium phosphate) per liter of distilled water
- Solution B: 9.07 g KH₂PO₄ (potassium dihydrogen phosphate) per liter of distilled water
- Mix 72 mL of Solution A + 28 mL of Solution B → pH 7.2 buffered water
Always verify pH with a calibrated pH meter or pH strips before use. Do not use tap water — its pH is unpredictable and varies by location and season.
Staining of the Slides
For Thin blood smears
- Fix air-dried film in absolute methanol by dipping the film briefly (two dips) in a Coplin jar containing absolute methanol.
- Remove and let air dry.
- Stain with a working solution of Giemsa stain
- Wash by briefly dipping the slide in and out of a Coplin jar of buffered water (one or two dips). **Note:**Excessive washing will decolorize the film.
- Let air dry in a vertical position. Observe under the microscope first at 40X and then using an oil immersion lens
For Thick blood smears
- Allow the film to air dry thoroughly for several hours or overnight. Do not dry films in an incubator or by heat, because this will fix the blood and interfere with the lysing of the RBCs. **Note:**If a rapid diagnosis of malaria is needed, thick films can be made slightly thinner than usual, allowed to dry for 1 hour, and then stained.
- DO NOT FIX.
- Stain with diluted Giemsa stain
- Wash by placing the film in buffered water for 3 to 5 min.
- Let air dry in a vertical position, observe under the microscope at 40X, and then use an oil immersion lens.
For Chlamydia trachomatis
Follow the aforementioned steps with the dilute stain of 1:40 dilution (add 0.5 ml stock Giemsa solution to 19.5 ml buffered water) and leave the stain for 90-120 minutes.
Get details about: Thick and thin blood smear procedure
Observation
On microscopic observation, cell organelles, bacteria, and parasites are distinguished based on their morphology and color;
| Cell Components | The color observed after staining |
|---|---|
| Red blood cells | Mauve-pink |
| Neutrophils | Reddish purple nuclei with pink cytoplasm |
| Eosinophils | Purple nuclei, faintly pink cytoplasm, and red to orange granules. |
| Basophils | Purple nuclei, blue coarse granules. |
| Lymphocytes | Dark blue nucleus with light blue cytoplasm. |
| Monocytes | Pink cytoplasm with a purple color nucleus. |
| Platelets | Violet to purple color granules. |
| Nuclei of host cells | Dark purple |
| Nuclei of WBCs | Dark purple |
| The cytoplasm of host cells | Pale blue |
| The cytoplasm of white cells | Pale blue or grey-blue |
| Melanin granules | Black green |
| Bacteria | Pale or dark blue |
| Chlamydia trachomatis inclusion bodies | Blue-mauve to dark purple depending on the stage of development |
| Borrelia spirochetes | Mauve-purple |
| Yersinina pestis coccobacilli | Blue with dark stained ends (bipolar staining) |
| Malaria parasite | Malaria parasites have a red or pink nucleus and blue cytoplasm. If P. vivax is seen, the Schüffner dots are seen as an even carpet of pink dots in the cytoplasm of red blood cells . If P. falciparum is observed, Maurer clefts will be seen as unevenly distributed, coarse bodies in the red cell cytoplasm. |
Uses of Giemsa Stain
Wright-Giemsa’s stain is commonly used to demonstrate the cellular elements in peripheral blood and bone marrow smears. Giemsa stain is used to obtain differential white blood cell counts. It is also used to differentiate the nuclear and cytoplasmic morphology of the various blood cells like platelets, RBCs, and WBCs.
In Microbiology, Giemsa stain is used for staining inclusion bodies in Chlamydia trachomatis, Borrelia species, and if Wayson’s stain is not available, to stain Yersinia pestis. Giemsa stain also is used to stain Histoplasma capsulatum, Pneumocystis jiroveci, Klebsiella granulomatis, Talaromyces marneffei (formerly called Penicillium marneffei), and occasionally bacterial capsules.
Cytogenetics also uses this stain to stain the chromosomes and identify chromosomal aberrations. It is commonly used for G-banding (Giemsa-Banding)
Parasitology
In microbiology, this stain is most commonly used in parasitology to detect intraerythrocytic (plasmodia, babesiae) and exoerythrocytic (trypanosomes, microfilaria) parasites. It is also used for the detection of intracellular amastigotes of Leishmania species or Trypanosoma cruzi.

Get details about: Plasmodium life cycle and species differentiation
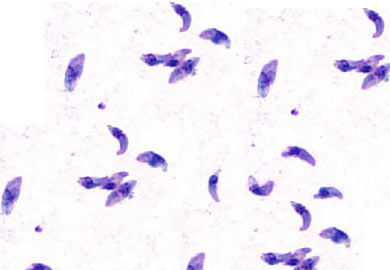 Figure: Tachyzoites
Figure: Tachyzoites
Giemsa stain is also used for the laboratory diagnosis of Toxoplasmosis. Tachyzoites of Toxoplasma gondii are best seen in needle aspirates, or impression smears stained with Wright-Giemsa. In Giemsa-stained smears characteristics, bow-shaped or crescent-shaped tachyzoites with the central dark-staining nucleus are seen.

Bacteriology
Wright-Giemsa stain has little use for staining bacteria, but it can be used for the laboratory diagnosis of various obligate intracellular parasites.
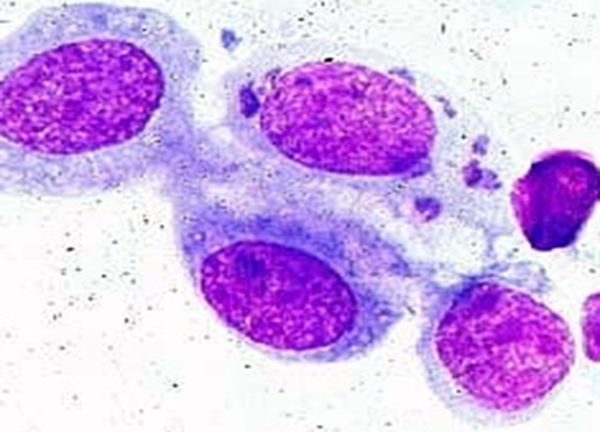 Figure: Giemsa Staining Photograph showing epithelial cells of conjunctiva containing intra-cytoplasmic inclusions “draped” around nucleus (source)
Figure: Giemsa Staining Photograph showing epithelial cells of conjunctiva containing intra-cytoplasmic inclusions “draped” around nucleus (source)
The diagnosis of Chlamydia trachomatis infection can be made if large numbers of chlamydial inclusion bodies are seen in a sample stained by the Giemsa or Gimenez methods.
The laboratory diagnosis of granuloma inguinale relies on the staining of intracellular bacteria in mononuclear cells and observation of “Donovan bodies” in tissue smears or biopsy specimens examined by Giemsa and Wright stains.
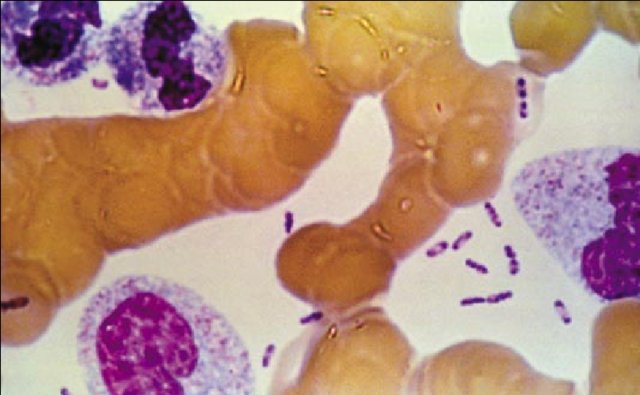 Wright-Giemsa stains of peripheral blood smears of people suffering from bubonic plague reveal the characteristics of bipolar staining typical of *Yersinia.*Note: bipolar staining “closed safety pin” shaped cells.
Wright-Giemsa stains of peripheral blood smears of people suffering from bubonic plague reveal the characteristics of bipolar staining typical of *Yersinia.*Note: bipolar staining “closed safety pin” shaped cells.

In people suffering from Carrion’s disease, Bartonella bacilliformis can be seen in the tissues both intra-and extracellularly. On Giemsa-stained blood films, the organism appears blue-to-purple extraerythrocytic and intraerythrocytic bacilli and coccobacilli.
Mycology
Detect the intracellular yeast forms of Histoplasma capsulatum.

Virology
The stain is also helpful for demonstrating specific intracellular viral inclusions. Herpes simplex virus produces multinucleated giant cells with intranuclear inclusions, which can be visualized after staining with Wright’s stain (or Wright-Giemsa stain).
Quick Reference:Giemsa Stain Uses by Organism
| Organism | Specimen type | What Giemsa shows | Category |
|---|---|---|---|
| Plasmodium falciparum | Thick and thin blood smear | Ring forms; crescent-shaped gametocytes; Maurer's clefts (coarse, irregular) | Parasitology |
| Plasmodium vivax | Thick and thin blood smear | Enlarged RBCs; amoeboid trophozoites; Schüffner's dots (fine, pink, regular) | Parasitology |
| Plasmodium malariae | Thick and thin blood smear | Band-form trophozoites; Ziemann's stippling | Parasitology |
| Plasmodium ovale | Thick and thin blood smear | Oval/fimbriated RBCs; Schüffner's/James' dots | Parasitology |
| Babesia spp. | Thin blood smear | Intraerythrocytic rings; "Maltese cross" (tetrad form) | Parasitology |
| Trypanosoma brucei | Peripheral blood smear | Extracellular trypomastigotes with undulating membrane | Parasitology |
| Trypanosoma cruzi | Peripheral blood smear | C-shaped or U-shaped trypomastigotes | Parasitology |
| Leishmania spp. | Bone marrow aspirate, splenic aspirate | Intracellular amastigotes (Leishman-Donovan bodies) in macrophages — 2–4 μm oval bodies with rod-shaped kinetoplast | Parasitology |
| Toxoplasma gondii | Needle aspirate, impression smear | Bow-shaped or crescent-shaped tachyzoites with dark central nucleus | Parasitology |
| Microfilaria | Thick blood smear | Sheathed or unsheathed microfilariae | Parasitology |
| Chlamydia trachomatis | Conjunctival scraping, urethral smear | Blue-mauve intracytoplasmic inclusion bodies "draped" around nucleus | Bacteriology |
| Borrelia spp. | Peripheral blood smear | Mauve-purple loosely coiled spirochetes between RBCs | Bacteriology |
| Yersinia pestis | Blood smear, lymph node aspirate | Blue coccobacilli with dark bipolar staining ("closed safety pin" or "closed pinhole" appearance) | Bacteriology |
| Bartonella bacilliformis | Blood smear | Blue-purple intra- and extraerythrocytic bacilli and coccobacilli | Bacteriology |
| Klebsiella granulomatis | Tissue smear | Intracellular organisms in mononuclear cells ("Donovan bodies") | Bacteriology |
| Histoplasma capsulatum | Bone marrow, peripheral blood, BAL | Small (2–4 μm) intracellular yeast forms within macrophages; narrow-based budding | Mycology |
| Pneumocystis jirovecii | BAL, induced sputum | Intracystic bodies (ascospores); cysts not stained by Giemsa (use GMS for cysts) | Mycology |
| Talaromyces marneffei | Blood smear, bone marrow | Intracellular yeast-like cells with transverse septum (not budding — distinguishes from Histoplasma) | Mycology |
| Herpes simplex virus | Tzanck smear | Multinucleated giant cells with intranuclear inclusions (Cowdry type A) | Virology |
| Chromosomes (G-banding) | Tissue culture, amniotic fluid | Dark and light bands on chromosomes for karyotype analysis | Cytogenetics |
Troubleshooting Common Giemsa Staining Problems
| Problem | Likely cause | Solution |
|---|---|---|
| Everything stains blue — RBCs appear grey-blue | Buffered water too alkaline (pH >7.4) | Prepare fresh buffered water at pH 7.2; verify with pH meter |
| Everything stains pink/red — parasites poorly visible | Buffered water too acidic (pH <6.8) | Prepare fresh buffered water at pH 7.2 |
| Pale, weak staining overall | Working solution too dilute; staining time too short; expired stain | Increase concentration to 10%; extend staining time; prepare fresh stock |
| Stain precipitate on slide | Water contamination in stock; working solution not filtered; staining too long | Filter stock before use; prepare working solution fresh; reduce staining time |
| Schüffner's dots not visible | Wrong pH (most common cause); understaining | Correct pH to 7.2; extend staining time |
| RBCs lysed in thick smear | Thick film fixed in methanol before staining | Never fix thick smears — methanol prevents RBC lysis; start fresh |
| Excessive background staining | Inadequate washing after staining; slide not clean before use | Wash more thoroughly with buffered water; use clean slides |
| Organisms not staining | Wrong dilution for organism type (e.g. Chlamydia needs 1:40); staining time too short | Use correct dilution per organism (see staining procedure); extend time |
| Uneven staining across slide | Slide not level during staining; insufficient stain volume | Ensure slide is horizontal; use at least 3 mL stain per slide |
| Stain colour changes over time | Water contamination in stock; exposure to light; heat | Store in dark amber bottle; discard contaminated stock |
Where Students Actually Get Confused
1. "Giemsa and Wright-Giemsa are the same stain." They are related but distinct formulations. Giemsa alone (azure B + eosin Y + methylene blue in glycerol/methanol) is the WHO-recommended stain specifically for malaria parasite morphology and stippling detail. Wright stain is self-fixing and faster, preferred for routine haematology differential counts. Wright-Giemsa combines both and is the common choice in reference laboratories needing both blood cell morphology and parasite detail. Using Wright stain alone for malaria diagnosis is acceptable but inferior — Schüffner's dots and Maurer's clefts are less reliably visualised.
2. "Thick and thin smears are stained the same way." No — this is the single most consequential procedural distinction in the entire article. Thin smears are fixed in methanol before staining; thick smears must never be fixed, because methanol prevents the RBC lysis that thick smear staining depends on. A thick smear accidentally fixed with methanol (or even methanol vapour from a nearby thin smear) becomes unreadable — RBCs remain intact and opaque, obscuring any parasites present.
3. "Any tap water works for buffered water." The article is explicit that tap water pH is unpredictable and varies by location and season — but this point is easy to skim past. In practice, this is the most common cause of stain failure in field laboratories, especially in regions with naturally alkaline groundwater (common in many limestone-rich areas of South Asia). Always verify pH with a calibrated meter or strips; never assume tap water is neutral.
4. "More staining time always gives better results." Understaining causes pale, weak results — but overstaining causes excessive background and can obscure fine structures like Schüffner's dots just as effectively as poor pH. The troubleshooting table correctly separates "pale, weak staining" (too short / too dilute) from pH-driven colour problems — students should not assume every staining failure is a timing issue when pH is the more common root cause.
5. "Giemsa stains the cyst wall of Pneumocystis jirovecii." The quick-reference table correctly notes Giemsa stains the intracystic bodies (ascospores) of P. jirovecii but does NOT stain the cyst wall itself. A learner reading only the organism name (and not the specimen/finding columns carefully) may assume Giemsa is a complete stain for Pneumocystis — it is not. GMS (Gomori methenamine silver) is required to visualise the cyst wall; Giemsa alone risks a false-negative impression if the cyst wall is what is being sought.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Stain type | Romanowsky stain | Named after Gustav Giemsa |
| Acidic dyes | Azure B, Eosin Y | Stain basic components (cytoplasm) |
| Basic dye | Methylene blue | Stains acidic components (nucleus) |
| Fixative for thin smear | Methanol | Required — fixes RBCs to slide |
| Thick smear fixation | Never fix | Methanol prevents RBC lysis |
| Optimal buffer pH | 7.0–7.2 | Single most common failure point |
| pH too low effect | Eosin dominates — pink/red overall | Acidic = pink |
| pH too high effect | Methylene blue dominates — blue-grey overall | Alkaline = blue |
| Rapid method dilution | 10% working solution | 1–15 slides; outpatient/urgent use |
| Slow method dilution | 3% working solution | >20 slides; field surveys |
| Working solution shelf life | Use within 15 minutes of preparation | Discard unused stain |
| Stock solution shelf life | ~2 years if kept dry and dark | Water contamination = primary degradation risk |
| P. vivax stippling | Schüffner's dots — fine, regular, pink | Even carpet pattern |
| P. falciparum stippling | Maurer's clefts — coarse, irregular | Patchy distribution |
| Chlamydia dilution | 1:40 dilution, 90–120 min stain time | Different protocol from blood films |
| WHO recommendation | Giemsa is gold standard for malaria | Wright stain not specifically recommended for malaria |
: Self-Check Questions
Paste: After Key Exam Facts table, before References
- A batch of thick blood smears is uniformly blue-grey after Giemsa staining and parasite morphology is unreadable. What is the most likely cause, and how would you confirm it?
- A technician accidentally applies methanol to a thick smear before staining. What happens, and why?
- Why is Wright stain preferred for routine haematology differential counts but Giemsa preferred for malaria diagnosis?
- A laboratory needs to stain 35 slides collected during a field survey with no urgency for same-day results. Should they use the rapid or slow method, and why?
- On a Giemsa-stained thin smear you see fine, regularly distributed pink stippling within enlarged RBCs. What organism and what feature is this?
- Why must the Giemsa working solution be used within 15 minutes of preparation?
Answers
- The most likely cause is alkaline buffered water (pH above 7.4). Methylene blue dominates at high pH, producing an overall blue-grey appearance and obscuring parasite morphology. Confirm by checking the pH of the buffered water with a calibrated pH meter or pH strips; correct by preparing fresh buffered water at pH 7.2.
- The RBCs will not lyse during staining, leaving them intact and opaque on the slide. This obscures the malaria parasites that the thick smear technique depends on detecting against a lysed, transparent background. The smear becomes unreadable and must be remade from a fresh, unfixed sample.
- Wright stain is self-fixing and faster (2–5 minutes), making it efficient for routine blood cell differential counts in busy haematology laboratories. Giemsa stain provides superior detail of parasite stippling (Schüffner's dots, Maurer's clefts), which is essential for accurate malaria species identification — this is why WHO specifically recommends Giemsa for malaria diagnosis despite its longer staining time.
- The slow (3%) method. It is appropriate for staining a larger number of slides (>20) where same-day urgency is not required, and it is less expensive per slide than the rapid method since it uses less stain. The rapid (10%) method is reserved for urgent, small-batch diagnosis (1–15 slides) in outpatient or clinical settings.
- Plasmodium vivax — the fine, regular, evenly distributed pink stippling within enlarged red blood cells is characteristic of Schüffner's dots, a key identifying feature distinguishing P. vivax from P. falciparum (which shows coarse, irregular Maurer's clefts instead).
- Giemsa working solution is unstable once diluted from the stock — the dye complex begins to degrade and precipitate shortly after dilution in buffered water, reducing staining quality. Using it promptly (within 15 minutes) ensures consistent, reliable staining; any unused solution should be discarded rather than stored for later use.
References
- World Health Organization. (2016). Malaria Microscopy. Quality Assurance Manual — Version 2. WHO Press, Geneva.
- Tille, P. M. (2017). Bailey & Scott's Diagnostic Microbiology (14th ed.). Mosby Elsevier.
- Garcia, L. S. (2013). Diagnostic Medical Parasitology (5th ed.). ASM Press.
- Barcia, J. J. (2007). The Giemsa stain: its history and applications. International Journal of Surgical Pathology, 15(3), 292–296. https://doi.org/10.1177/1066896907302239
Frequently Asked Questions
Why is Giemsa preferred over Wright stain for malaria?
What is the difference between thick and thin blood smears?
Why must thick smears never be fixed with methanol?
What is the significance of Schüffner's dots vs Maurer's clefts?
How do you differentiate Leishmania from Histoplasma on Giemsa?
What is the safety pin appearance of Yersinia pestis?
Why does Giemsa stain nucleus purple and cytoplasm blue?
How long is Giemsa stock stable?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.