ELISA Test: Principle, Types (Direct, Indirect, Sandwich, Competitive), Procedure, and Uses
ELISA (Enzyme-Linked Immunosorbent Assay) is the most widely used immunoassay for detecting antibodies and antigens. Learn all four ELISA types — direct, indirect, sandwich, and competitive — with step-by-step procedures, clinical applications (HIV, HBsAg, dengue), and how to choose the right type.
When a blood sample from a patient suspected of HIV infection arrives in the laboratory, the first test performed is not culture, not PCR, and not a Western blot. It is an ELISA — specifically an indirect ELISA that detects anti-HIV antibodies in the patient's serum. In under four hours, a result is available. If reactive, confirmatory testing follows. If non-reactive in a low-risk individual, infection is effectively ruled out.
ELISA (Enzyme-Linked Immunosorbent Assay) is the most widely used immunoassay in clinical, research, and public health laboratories worldwide. It can detect either an antigen (what the pathogen is) or an antibody (how the body has responded to the pathogen), depending on which of the four ELISA formats is used. It is the platform behind HIV screening, HBsAg detection, dengue NS1 antigen tests, pregnancy tests, food safety testing, and hundreds of other diagnostic applications.
Understanding ELISA means understanding four different formats — Direct, Indirect, Sandwich, and Competitive — each designed for a different detection purpose.
Enzyme immunoassay (EIA), enzyme-linked immunosorbent assay (ELISA), is the most widely used type of immunoassay. ELISA is a rapid test for detecting the presence and amount of either antigen or antibody in a sample.
The indirect ELISA is used to screen patients for detecting or quantifying antibodies (Ab) against viruses, bacteria, and other antigens (Ag). For example, detection of HIV antibodies, antibodies against rubella virus, etc., are done using indirect ELISA. Direct ELISA is used to detect hormones (such as human chorionic gonadotropin (HCG) in some pregnancy tests and luteinizing hormone (LH) in ovulation tests), drugs, and viral and bacterial antigens.
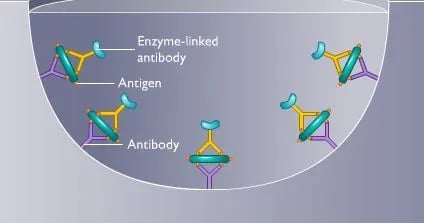
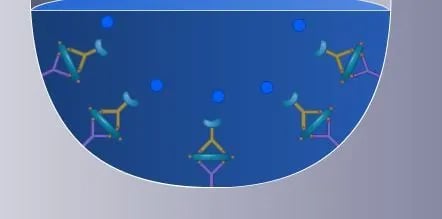
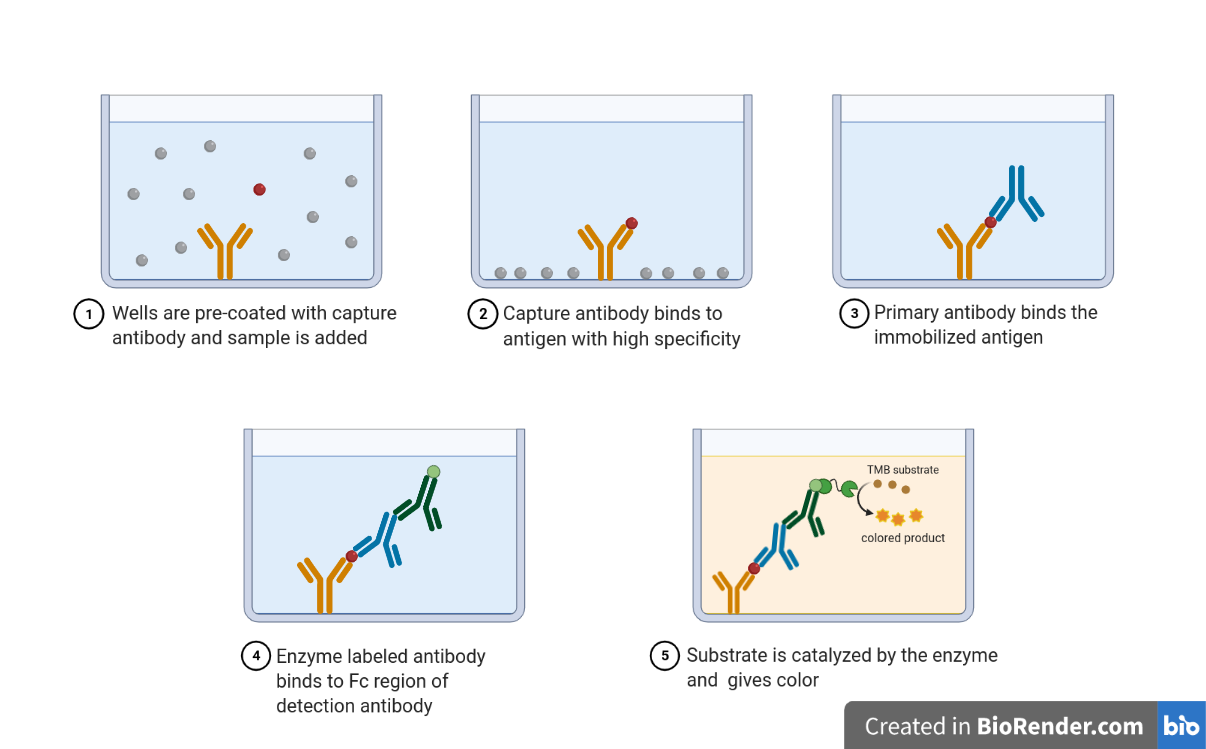 Figure: Sandwich ELISA (imagesource)
Figure: Sandwich ELISA (imagesource)
What Is ELISA?
ELISA is so named because the test technique involves using an enzyme system and immunosorbent. The term enzyme-linked refers to an enzyme’s covalent binding to an antibody. ELISA belongs to a family of techniques called solid-phase immunoassays — assays in which one member of the antigen-antibody pair is immobilised on a solid surface (the well of a 96-well polystyrene plate) and the other is captured from the test sample. An enzyme-labelled antibody then generates a measurable color signal proportional to the amount of antigen or antibody present.
The solid-phase design solves a fundamental problem in immunoassay: separating bound from unbound reagents. Washing the plate removes everything not attached to the well surface, eliminating background noise and making the signal clean and quantifiable.
Why enzyme labelling instead of radioactivity (as in RIA)
The use of enzymes as the label has several advantages.
- The enzyme itself is not changed during ELISA. It can catalyze the reaction of many substrate molecules, greatly amplifying the reaction and enhancing detection.
- Enzyme-conjugated antibodies are stable and can be stored for a relatively long time.
- The formation of a colored end product allows direct observation of the reaction or automated spectrophotometric reading.
The Four Types of ELISA — Overview
Four ELISA formats exist, each designed for a specific detection purpose. Understanding which format to use requires knowing whether you are detecting an antigen or an antibody, and whether speed or sensitivity is the priority.
| ELISA type | What is coated on plate | What is detected in sample | Enzyme conjugated to | Best for | Sensitivity |
|---|---|---|---|---|---|
| Direct ELISA | Antigen (from sample, non-specific adsorption) | — (antigen itself is detected directly) | Primary antibody against antigen | Screening antigen in simple samples; research; coating efficiency checks | Low-moderate |
| Indirect ELISA | Antigen (known) | Antibody in patient sample | Secondary anti-human IgG antibody | Patient antibody detection: HIV, HCV, rubella, toxoplasma serology | High |
| Sandwich ELISA | Capture antibody (known, specific) | Antigen in patient sample | Detector antibody against different antigen epitope | Antigen quantification in complex samples: HBsAg, dengue NS1, p24, cytokines | Highest |
| Competitive ELISA | Antibody (known) OR antigen (known) | Antigen OR antibody — by competition | Enzyme-labelled antigen or antibody | Small molecules, haptens, drugs, hormones; when only one antibody binding site available | Variable |
The most important clinical distinction: Indirect ELISA detects patient antibodies (serology); Sandwich ELISA detects patient antigens (direct pathogen detection). This distinction drives test selection in clinical diagnostics.
Type 1: Direct ELISA
What it detects: Antigen directly in a sample.
Principle: In Direct ELISA, the antigen from the test sample is adsorbed non-specifically onto the plate surface. An enzyme-labelled antibody specific to that antigen is then added directly — there is no secondary antibody. The enzyme-labelled antibody binds directly to the plate-adsorbed antigen, hence "direct."
Step-by-step procedure:
- Coat plate: Add sample directly to the well — antigen adsorbs non-specifically to the polystyrene surface. Incubate at 4°C overnight or 37°C for 2 hours.
- Block: Add blocking buffer (1–5% BSA or skimmed milk in PBS) for 1 hour at 37°C to prevent non-specific antibody binding to bare polystyrene.
- Wash: 3–5 times with PBS-Tween wash buffer.
- Add enzyme-conjugated primary antibody: Specific for the target antigen; labelled directly with HRP or alkaline phosphatase. Incubate 1–2 hours.
- Wash: Remove unbound conjugated antibody — 3–5 washes.
- Add substrate: TMB (for HRP) or PNPP (for AP). Incubate 15–30 minutes in the dark.
- Stop reaction: Add stop solution (H₂SO₄ for TMB; NaOH for PNPP).
- Read absorbance: Measure at 450 nm (TMB) or 405 nm (PNPP) using an ELISA reader.
Advantages:
- Fast — fewer incubation steps
- No cross-reactivity from secondary antibody
- Simple protocol
Limitations:
- Lower sensitivity than Indirect or Sandwich ELISA (no signal amplification)
- Each target antigen requires its own enzyme-conjugated primary antibody (expensive)
- Non-specific adsorption of antigen to plate may lose conformational epitopes
Clinical uses: Screening antigens in research; coating efficiency checks; some rapid antigen tests.
Type 2: Indirect ELISA
What it detects: Antibodies in patient serum — the most clinically important ELISA format for infectious disease serology.
Principle: A known antigen is coated on the plate. If the patient's serum contains antibodies against that antigen, they bind to the plate-coated antigen. An enzyme-labelled secondary antibody (anti-human IgG) then detects any human antibody bound to the plate. The "indirect" name comes from this two-step detection: the enzyme label is on the secondary antibody, not directly on the patient antibody.
The signal amplification advantage: Because multiple secondary antibody molecules can bind to a single primary antibody, Indirect ELISA amplifies the signal — detecting antibodies present in very small quantities.
Step-by-step procedure:
- Coat plate with known antigen: Add antigen solution (specific concentration per kit instructions). Incubate at 4°C overnight.
- Block: 1–5% BSA or milk for 1 hour at 37°C.
- Wash: 3–5 times with PBS-Tween.
- Add patient serum (primary antibody): Diluted as per kit instructions (typically 1:100 to 1:400). Incubate 1–2 hours at 37°C.
- Wash: Remove unbound patient antibodies — 3–5 washes.
- Add enzyme-conjugated secondary antibody: Anti-human IgG (or IgM) labelled with HRP or alkaline phosphatase. Incubate 1 hour at 37°C.
- Wash: Remove unbound secondary antibody.
- Add substrate: TMB or PNPP. Incubate 15–30 minutes in dark.
- Stop reaction and read absorbance.
Interpretation:
- Optical Density (OD) above cut-off value = Reactive (antibodies detected)
- OD below cut-off = Non-reactive
- The cut-off is determined by the mean OD of negative controls plus 2–3 standard deviations, as specified in the kit insert
Clinical applications of Indirect ELISA:
| Target antibody | Clinical use |
|---|---|
| Anti-HIV IgG/IgM | HIV screening (3rd and 4th generation kits) |
| Anti-HCV IgG | Hepatitis C screening |
| Anti-rubella IgG | Immunity status; antenatal screening |
| Anti-toxoplasma IgG/IgM | Toxoplasmosis diagnosis; pregnancy screening |
| Anti-Chikungunya IgM | Chikungunya diagnosis |
| Anti-Zika IgM | Zika virus diagnosis |
| Anti-H. pylori IgG | H. pylori serology (less preferred than stool antigen) |
| Anti-dengue IgM/IgG | Dengue serology (IgM = primary infection) |
Type 3: Sandwich ELISA
What it detects: Antigens in patient samples — the most sensitive and specific ELISA format.
Why "sandwich": Two antibodies recognising different epitopes of the same antigen "sandwich" the antigen between them — capture antibody on the bottom, detector antibody on top.
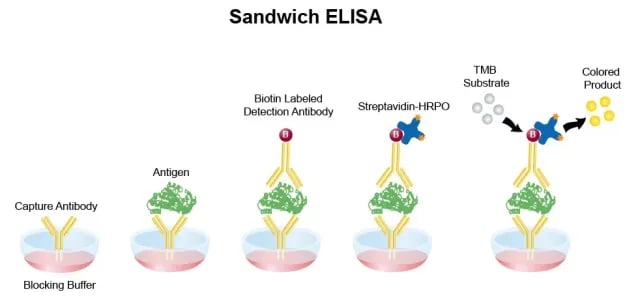 Figure: Sandwich ELISA
Figure: Sandwich ELISA
Principle: A capture antibody specific to the target antigen is coated on the plate. Patient sample is added — if antigen is present, it is captured. A second detector antibody (also specific to the target antigen but recognising a different epitope) is then added, labelled with an enzyme. The antigen is physically sandwiched between two antibodies. This dual-antibody recognition makes Sandwich ELISA the most specific and sensitive format.
Step-by-step procedure:
- Coat plate with capture antibody: Incubate at 4°C overnight or 37°C for 2 hours.
 2. Block: 1–5% BSA for 1 hour at 37°C. Wash 3–5 times.
3. Add patient sample (test specimen): If antigen is present, it binds to the capture antibody. Incubate 1–2 hours at 37°C.
2. Block: 1–5% BSA for 1 hour at 37°C. Wash 3–5 times.
3. Add patient sample (test specimen): If antigen is present, it binds to the capture antibody. Incubate 1–2 hours at 37°C.
 4. Wash: Remove unbound sample components thoroughly — 3–5 washes.
5. Add enzyme-conjugated detector antibody: Binds to a different epitope on the captured antigen. Incubate 1–2 hours at 37°C.
4. Wash: Remove unbound sample components thoroughly — 3–5 washes.
5. Add enzyme-conjugated detector antibody: Binds to a different epitope on the captured antigen. Incubate 1–2 hours at 37°C.
 6. Wash: Remove unbound detector antibody.
7. Add substrate: Color develops proportional to antigen quantity.
6. Wash: Remove unbound detector antibody.
7. Add substrate: Color develops proportional to antigen quantity.
 8. Stop and read absorbance.
8. Stop and read absorbance.
Advantages over other ELISA formats:
- Highest sensitivity — dual antibody recognition
- Highest specificity — requires binding to two different epitopes; very low false positives
- Works in complex matrices (serum, plasma, cell lysates) without extensive sample purification
- Quantitative with a standard curve
Clinical applications of Sandwich ELISA:
| Target antigen | Clinical use |
|---|---|
| HBsAg | Hepatitis B diagnosis and screening |
| HBeAg | HBV replication status |
| HIV p24 antigen | Early HIV detection (4th generation kits); neonatal diagnosis |
| Dengue NS1 antigen | Acute dengue diagnosis days 1–7 |
| Influenza antigen | Rapid flu diagnosis |
| Rotavirus antigen | Gastroenteritis diagnosis in children |
| C. difficile toxin A/B | Antibiotic-associated diarrhoea |
| Botulinum toxin | Food poisoning investigation |
| TNF-α, IL-6, IL-10 | Cytokine quantification in research |
| PSA (Prostate-Specific Antigen) | Prostate cancer screening |
The 4th-generation HIV test combines Indirect + Sandwich ELISA: Modern HIV "combo" tests simultaneously detect anti-HIV antibodies (Indirect ELISA component) AND HIV p24 antigen (Sandwich ELISA component) in a single well — reducing the window period from 45 days (3rd-generation antibody-only) to 15–20 days.
Type 4: Competitive ELISA
What it detects: Antigens at very low concentrations; small molecules (haptens, drugs, hormones) with only one antibody binding site.
Principle: Competitive ELISA works by competition between labelled and unlabelled antigen for a limited number of antibody binding sites. The more unlabelled antigen in the patient sample, the less labelled antigen binds, and the less color is generated. The relationship is inverse: high antigen concentration = low color signal.
Two configurations:
Configuration A (antigen-coated plate):
- Coat plate with known antigen
- Pre-mix patient sample with enzyme-labelled antibody
- Add the mixture to the plate — patient antigen and plate-coated antigen compete for the labelled antibody
- Wash and add substrate
- High patient antigen → less labelled antibody binds to plate → less color → HIGH patient antigen = LOW OD
Configuration B (antibody-coated plate):
- Coat plate with capture antibody
- Patient antigen and enzyme-labelled antigen compete for plate-bound antibody
- High patient antigen = less labelled antigen captured = low color
Clinical and non-clinical uses:
- Hormone measurement (testosterone, cortisol, progesterone, hCG in quantitative pregnancy tests)
- Drug monitoring (therapeutic drug levels: digoxin, cyclosporine)
- Pesticide and mycotoxin detection in food
- Hapten detection (molecules too small to have two different epitopes for a Sandwich ELISA)
Why competitive ELISA for hormones? Hormones are small molecules — too small to allow two different antibodies to bind simultaneously (required for Sandwich ELISA). Competitive ELISA is the only format that works reliably for these targets.
Choosing the Right ELISA Type
| Question | Recommended format |
|---|---|
| Detecting antibodies in patient serum (serology)? | Indirect ELISA |
| Detecting antigens in a complex biological sample? | Sandwich ELISA |
| Measuring a small molecule/hormone/drug? | Competitive ELISA |
| Simple research screening for antigen presence? | Direct ELISA |
| Highest sensitivity and specificity needed? | Sandwich ELISA |
| Fastest, fewest steps? | Direct ELISA |
| Can only afford one secondary antibody for multiple targets? | Indirect ELISA (same anti-species secondary works for all) |
Signal direction — the competitive ELISA trap: All ELISA formats give a direct signal (more analyte = more color) except Competitive ELISA which gives an inverse signal (more analyte = less color). This is the most common source of misinterpretation in competitive ELISA results.Salient Features of ELISA Test
ELISA test is being increasingly used in the detection of antigen (the infectious agent) or antibody due to its simplicity and sensitivity. It is as sensitive as radioimmunoassay (RIA) and requires only microliter quantities of test reagents. It has now been widely applied in the detection of a variety of antibodies and antigens such as hormones, toxins, and viruses.
Advantages of ELISA
- Highest sensitivity — detects nanogram to picogram quantities of analyte
- Highly specific — antibody-antigen reaction is highly specific
- Quantitative — OD value is proportional to analyte concentration; standard curves allow absolute quantification
- High throughput — 96-well format processes 40+ patient samples simultaneously with controls
- No radioactivity — safer than RIA, no radiation hazards, no radioactive waste
- Stable reagents — enzyme conjugates store at 4°C for months; longer shelf life than radiolabelled reagents
- Automated — plate washers and readers enable full automation in high-volume laboratories
- Versatile — detects antibodies, antigens, hormones, drugs, toxins across all specimen types
- Commercially available kits — standardised kits available for hundreds of targets with validated cut-offs
Limitations of ELISA
- Requires laboratory infrastructure — plate reader, washer, incubator; not suitable for point-of-care without modification
- Skilled operator needed — pipetting accuracy, wash technique, and timing all affect results
- Matrix effects — hemolysis, lipaemia, and high rheumatoid factor in patient serum can interfere
- Hook effect — very high antigen concentrations may give falsely low OD (antigen excess); requires dilution series
- Cross-reactivity — antibodies may cross-react with structurally similar antigens (e.g., dengue vs Zika antibody cross-reactivity in indirect ELISA)
- Window period — Indirect ELISA for antibodies cannot detect infection before seroconversion
- Confirmatory testing needed — reactive ELISA screens require confirmatory testing (e.g., Western blot for HIV, treponemal test for syphilis RPR)
Materials needed in ELISA Testing
- Pipettes, washer system, ELISA plate reader: Readers, washers, and pipettes are available as manual or automated systems. One of the main factors affecting equipment selection is the number and types of test samples being run.
- ELISA Readers: Readers need to have an appropriate filter (650 nm and 450 nm). Pipette: These are available as fixed as well as adjustable volume as well as single-channel and multi-channel. Washing system: It can be a manual system that washes one row or column at a time or semi-automated system that washes one strip or plate at a time or a fully automated system that can process multiple plates.
- Reagents needed for the testing- included in the kit (coated plates, sample diluents, controls, wash concentrate, conjugate, substrate, stop solution)
- Coated plates: The 96-well plates are made of polystyrene and are coated with either inactivated antigen or antibody. The function of the plate has to hold the immobilized either antigen or antibody. Antigens or antibodies present in the sample will bind to the plate. This coating acts as the binding site for the antibodies or antigens in the sample.
- Controls: Negative and positive controls are provided in each kit. The controls help to normalize or standardize each plate. Controls are also used to validate the assay and to calculate sample results. Controls might be pre-diluted and ready to use. (Please refer to the kit for specific instructions).
- Conjugates: ELISA conjugates are enzyme-labeled antibodies that react specifically to plate-bound sample analytes. Unbound conjugates are washed away after incubation and before the addition of substrate.
- Wash Concentrate: It acts as a buffered solution containing detergent to wash unbound material from the plate. (Not all test kits have wash concentrate; in that case, distilled water can be used for washing; please refer to kit insert for specific instructions)
- Stop solution: It stops the enzyme-substrate reaction and color development.
Principle of ELISA Test
Most ELISA methods developed for the detection of antigen or antibody consist of the use of the corresponding antibody or antigen in question which is firmly fixed on a solid phase, such as a plastic surface of a polyvinyl plate or polystyrene tube. Such systems are also called solid-phase immunosorbent assays (SPIA). A test sample is added to the microtiter plate, if there is the presence of Ag or Ab in the test sample, there will be Ag-Ab reactions (with immobilized Ab or Ag). Later enzyme-labeled antibody is added to the reaction mixture, which will combine with either the test antigen or the Fc portion of the test antibody. The enzyme system consists of;
- An enzyme: horse radish peroxidase, alkaline phosphatase which is labeled or linked, to a specific antibody.
- A specific substrate:
- o-Phenylenediamine dihydrochloride for peroxidase
- P Nitrophenyl Phosphate (PNPP)- for Alkaline Phosphatase
A substrate is added after the antigen-antibody reaction. The enzyme catalyzes (usually hydrolyses) the substrate to give a color endpoint (a yellow compound in the case of alkaline phosphatase). The intensity of the color is proportional to the amount of antibody or antigen present in the test sample, which can be quantified using an ELISA reader.
LAM ELISA is used for the measurement of lipoarabinomannan (LAM), a major surface antigen of Mycobacterial tuberculosis, from the urine and/or sputum of suspected tuberculosis patients. The analytical sensitivity of this assay is 50-100 folds higher compared to conventional ELISA.
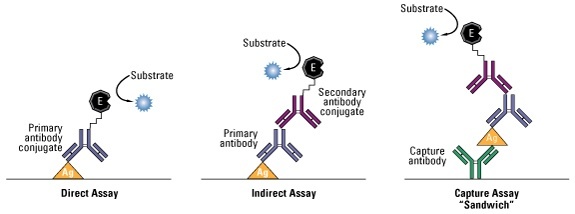 Figure: Format of ELISA
Figure: Format of ELISA
Clinical and Laboratory Uses of ELISA
ELISA is used across every field of diagnostic and research microbiology. The table below organises applications by ELISA type:
Infectious disease serology (Indirect ELISA): HIV antibody screening, HCV antibody, rubella IgG/IgM, toxoplasma IgG/IgM, Chikungunya IgM, Zika IgM, dengue IgM/IgG, EBV VCA IgM/IgG, CMV IgG/IgM, H. pylori IgG
Antigen detection (Sandwich ELISA): HBsAg, HBeAg, HIV p24, dengue NS1, influenza antigen, rotavirus antigen, C. difficile toxin A/B, Group A streptococcal antigen, botulinum toxin, histoplasma antigen
Bacteriology: Detection of Group A streptococcal antigen in throat swabs, C. difficile exotoxins in stool, botulinum toxin in food, Rocky Mountain spotted fever antibodies (Rickettsia rickettsii)
Mycology: Histoplasma antigen in urine/BAL (disseminated histoplasmosis), Aspergillus galactomannan (invasive aspergillosis)
Parasitology: Giardia antigen, P. falciparum HRP2 (malaria), Trypanosoma brucei IgM (African trypanosomiasis), Taenia solium antigen (neurocysticercosis)
Blood bank and transfusion medicine: HIV, HBsAg, HCV, HTLV-I/II screening of blood donors — ELISA is the primary screening platform for blood safety worldwide
LAM ELISA — a special application for tuberculosis: (Keep existing LAM ELISA callout box from main article)
Hormone and drug measurement (Competitive ELISA): hCG (pregnancy), LH (ovulation), testosterone, cortisol, therapeutic drug levels.
Common ELISA Problems and Troubleshooting
| Problem | Most likely cause | Solution |
|---|---|---|
| High background (all wells dark) | Insufficient washing; blocking inadequate; conjugate concentration too high | Increase wash steps and wash time; increase blocking time/concentration; dilute conjugate |
| No color in any well | Substrate forgotten or expired; enzyme activity lost; wrong substrate for enzyme | Check substrate expiry; verify enzyme-substrate compatibility (TMB for HRP; PNPP for AP); check plate reader wavelength setting |
| Positive control fails | Reagent degradation; incorrect incubation temperature; sample too dilute | Check reagent storage conditions; verify kit has not expired; use fresh positive control |
| All samples appear positive | Plate dried out during incubation; serum complement not inactivated (if required) | Use humidified incubation chamber; inactivate complement at 56°C for 30 min if required |
| Hook effect (high concentrations give falsely low OD) | Very high antigen concentration saturates both capture and detector antibodies separately | Dilute sample and repeat; use a wider standard curve range |
| Poor standard curve | Pipetting error in standard dilutions; standard degraded | Prepare fresh dilutions; use reverse pipetting for viscous standards; check pipette calibration |
| Inter-assay variability | Temperature variations; incubation time variation; wash variation | Strictly control incubation temperatures and times; use automated washer |
| Prozone effect (Competitive ELISA) | Sample tested neat — excess antigen; all antibody occupied | Test sample at multiple dilutions |
References
- Alhajj, M., Zubair, M., & Farhana, A. (2023). Enzyme Linked Immunosorbent Assay. In StatPearls. StatPearls Publishing.
- Hayrapetyan, H., Tran, T., Tellez-Corrales, E., & Madiraju, C. (2023). Enzyme-Linked Immunosorbent Assay: Types and Applications. Methods in molecular biology (Clifton, N.J.), 2612, 1–17. https://doi.org/10.1007/978-1-0716-2903-1_1
- Aydin S. (2015). A short history, principles, and types of ELISA, and our laboratory experience with peptide/protein analyses using ELISA. Peptides, 72, 4–15. https://doi.org/10.1016/j.peptides.2015.04.012
- Tille, P. M. (2017). Bailey and Scott's Diagnostic Microbiology (14th ed.). Elsevier.
- Engvall E., & Perlmann P. (1971). Enzyme-linked immunosorbent assay (ELISA). Quantitative assay of immunoglobulin G. Immunochemistry, 8(9), 871–874. https://doi.org/10.1016/0019-2791(71)90454-x
Frequently Asked Questions
Why is the indirect ELISA format used for HIV antibody detection rather than the direct or sandwich format?
What is the hook effect in sandwich ELISA and how can it cause a false negative in high-antigen-concentration samples?
How do 3rd-generation and 4th-generation HIV ELISA kits differ, and what is the clinical significance?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.