Broth Dilution Method for MIC: Macrodilution vs Microdilution, Procedure & Troubleshooting
Step-by-step broth macrodilution and microdilution procedure for MIC determination — antibiotic stock prep, 0.5 McFarland standardization, reading results, and a troubleshooting guide for the errors that actually happen at the bench.
The lowest concentration at which the isolate is completely inhibited (as evidenced by the absence of visible bacterial growth) is recorded as the minimal inhibitory concentration (MIC).
For how MIC relates to MBC and when each is clinically ordered, see MIC vs MBC.
Why This Matters
Most infections never need an MIC. A simple Susceptible/Resistant call from disc diffusion is enough to guide treatment, and that's deliberately how routine AST is designed — fast, cheap, categorical. MIC determination earns its place on the bench in narrower situations: a patient relapsing on therapy that should be working, an immunosuppressed patient where there's no margin for a "probably fine" answer, or a borderline result where the categorical call alone isn't precise enough to trust.
The Borderline Vancomycin MIC: An MRSA isolate reported "Susceptible" by disc diffusion can still carry a vancomycin MIC of 2 μg/mL rather than 0.5 μg/mL — both technically fall in the susceptible range, but the higher end of that range is associated with worse clinical outcomes in MRSA bacteremia (a pattern often called "MIC creep"). A categorical report alone would look reassuring; the actual number tells a different story. This is exactly why MIC determination — not just disc diffusion — gets escalated for serious MRSA infections.
Dilution methods can be carried out in 2 ways; broth dilution and agar dilution.
Broth Dilution Method
Broth dilution testing allows providing both quantitative (MIC) and qualitative (category interpretation) results. MIC can help establish the level of resistance of a particular bacterial strain and can substantially affect the decision to use certain antimicrobial agents.
Broth dilution can again be performed in 2 ways.
- Macro dilution: Uses broth volume of 1 ml in standard test tubes.
- Microdilution: Uses about 0.05 to 0.1 ml total broth volume and can be performed in a microtiter plate or tray.
| Macrodilution | Microdilution | |
|---|---|---|
| Broth volume | 1 mL per tube | 0.05–0.1 mL per well |
| Format | Standard test tubes | 96-well microtiter tray |
| Typical setting | Reference/research testing, small batches | Routine clinical labs, high throughput |
| Reading method | Visual turbidity | Visual, or automated (Vitek 2, MicroScan, BD Phoenix) |
| Underlying principle | Identical to microdilution — differs only in scale | Identical to macrodilution |
The procedure for macro and microdilution is the same except for the volume of the broth. MIC of an antibiotic using the broth dilution method is determined by using the following procedure
- Preparation of antibiotic stock solution
- Preparation of antibiotic dilution range
- Preparation of agar dilution plates
- Preparation of inoculum
- Inoculation
- Incubation
- Reading and interpreting results
Preparation of antibiotic stock solution
Antibiotic stock solution can be prepared by commercially available antimicrobial powders (with given potency). The amount needed and the diluents in which it can be dissolved can be calculated by using either of the following formulas to determine the amount of antimicrobial powder (1) or diluent (2) needed for a standard solution:
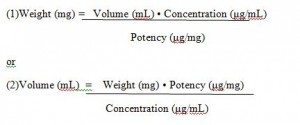 Figure: microdilution formula
Figure: microdilution formula
Prepare antimicrobial agent stock solutions at concentrations of at least 1000 μg/mL (example: 1280 μg/mL) or 10 times the highest concentration to be tested, whichever is greater.
Because microbial contamination is extremely rare, solutions prepared aseptically but not filter-sterilized are generally acceptable. If desired, however, solutions may be sterilized by membrane filtration. Dispense small volumes of the sterile stock solutions into a sterile glass, polypropylene, polystyrene, or polyethylene vials; carefully seal; and store (preferably at −60 °C or below, but never at a temperature warmer than −20 °C and never in a self-defrosting freezer). Vials may be thawed as needed and used the same day.
Preparation of antibiotic dilution range
- Use sterile 13- x 100-mm test tubes to conduct the test. If the tubes are to be saved for later use, be sure they can be frozen.
- Close the tubes with loose screw caps, plastic or metal closure caps, or cotton plugs.
- Prepare the final two-fold (or other) dilutions of antimicrobial agent volumetrically in the broth. A minimum final volume of 1 mL of each dilution is needed for the test.
Note: For microdilution, only 0.1 ml is dispensed into every 96 wells of a standard tray.
Preparation of inoculum
- Prepare the inoculum by making a direct broth suspension of isolated colonies selected from an 18- to 24-hour agar plate (use a non-selective medium, such asblood agar).
- Adjust the suspension to achieve turbidity equivalent to a 0.5 McFarland turbidity standard. This results in a suspension containing approximately 1 to 2 x 10^8 colony forming units (CFU)/mL for Escherichia coli ATCC®a 25922.
- Compare the inoculum tube and the 0.5 McFarland standard against a card with a white background and contrasting black lines.
- Optimally within 15 minutes of preparation, dilute the adjusted inoculum suspension in broth so, after inoculation, each tube contains approximately 5 x 10^5 CFU/mL.
Note: This can be accomplished by diluting the 0.5 McFarland suspension 1:150, resulting in a tube containing approximately 1 x 10^6CFU/mL. The subsequent 1:2 dilution in step 3 brings the final inoculum to 5 x 10^5CFU/mL.
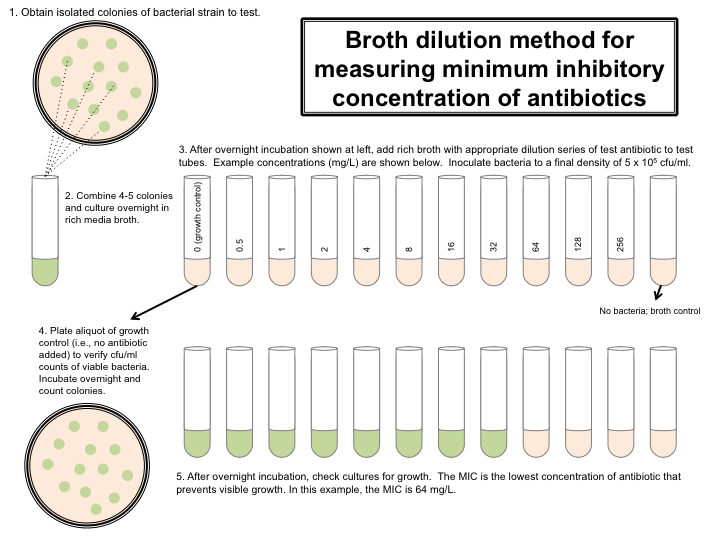 Figure: Broth dilution method for measuring the minimum inhibitory concentration of antibiotics.(image source:labome.com)
Figure: Broth dilution method for measuring the minimum inhibitory concentration of antibiotics.(image source:labome.com)
Inoculation
Within 15 minutes after the inoculum has been standardized as described above, add 1 mL of the adjusted inoculum to each tube containing 1 mL of antimicrobial agent in the dilution series (and a positive control tube containing only broth), and mix.
This results in a 1:2 dilution of each antimicrobial concentration and a 1:2 dilution of the inoculums.
Incubation
Incubate the inoculated tubes at 35 ± 2 ºC for 16 to 20 hours in an ambient air incubator. To maintain the same incubation temperature for all cultures, do not stack microdilution trays more than four high.
Interpretation
Compare the amount of growth in the wells or tubes containing the antimicrobial agent with the growth in the growth-control wells or tubes (no antimicrobial agent) used in each set of tests when determining the growth endpoints. For a test to be considered valid, acceptable growth (≥ 2 mm button or definite turbidity) must occur in the growth-control well.
Quality Control
Use reference bacterial strains that are genetically stable and have well-defined MICs in the middle range of the expected MICs of each antimicrobial agent to be tested. A dilution series should include at least two concentration increments above and below the previously established MIC for the reference organisms.
CLSI has established QC limits for dilution susceptibility tests; an unacceptable QC result falls outside these published limits. Reference strains recommended by the CLSI for
QC of dilution tests for aerobic bacteria are
- E. coli ATCC 25922,
- E. faecalis ATCC 29212,
- P. aeruginosa ATCC 27853, and
- S. aureus ATCC 29213.
Troubleshooting Microdilution Assays
Inappropriate MICs report: When MICs are lower than expected—the inoculum may be too light. When MICs are higher than expected—the inoculum may be too heavy. In such conditions, repeat testing using McFarland 0.5 turbidity standard or standardizing device. Check steps in the inoculum preparation and inoculation procedure.
When MICs are either higher or lower than expected—the composition of the cation-adjusted Müeller–Hinton broth may not be optimal. Check the pH and calcium concentration of in-house prepared media. Use an alternative commercial lot of media or an alternative lot of commercial panels.
When there are skipped wells—it may be caused by several problems: Check for contamination The panel may have been inadequately inoculated, or the inoculum may have been inadequately mixed. Drug concentration in the wells may be inaccurate. The volume of broth in the wells may be inaccurate.
When several MICs are too high or too low—which may indicate a possible reading/transcription error. Recheck all of the readings and repeat testing using an alternative lot.
Learning & Remembering
Quick hook: When troubleshooting a skewed result — Light → Low, Heavy → High. A too-light inoculum reads a falsely low MIC; a too-heavy inoculum reads a falsely high MIC. (This mirrors the existing troubleshooting section above — use it as the one-line version to recall under exam pressure.)
Clinical story 1 — The Borderline Vancomycin MIC: see "Why This Matters" above.
Clinical story 2 — The McFarland Shortcut: A classic bench scenario in any teaching lab — a rushed tech eyeballs the inoculum turbidity instead of confirming it against the actual 0.5 McFarland standard or a densitometer. The inoculum ends up heavier than intended, every MIC on the run reads falsely elevated, and it's only caught because that day's quality-control reference strain (E. coli ATCC 25922) also came back out of its expected range — which is the entire reason QC strains are run alongside patient isolates in the first place.
One sentence that captures it: A broth dilution MIC turns a vague "is this drug working?" into a precise number a clinician can weigh against achievable drug levels — but that number is only as trustworthy as the inoculum it was read from.
Exam facts
| Question | Answer |
|---|---|
| Standard broth volume for macrodilution? | 1 mL |
| Standard broth volume for microdilution? | 0.05–0.1 mL per well |
| McFarland standard used for inoculum prep? | 0.5 McFarland |
| Target final inoculum concentration in the tube? | ~5 × 10⁵ CFU/mL |
| Standard incubation conditions? | 35 ± 2°C for 16–20 hours |
| MICs read lower than expected across the board — likely cause? | Inoculum too light |
| MICs read higher than expected across the board — likely cause? | Inoculum too heavy |
| Two CLSI QC reference strains for dilution testing | E. coli ATCC 25922, S. aureus ATCC 29213 (also P. aeruginosa ATCC 27853, E. faecalis ATCC 29212) |
References and further readings
- CLSI. M07—Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically, 12th ed. Clinical and Laboratory Standards Institute; 2024.
- Procop GW, Church DL, Hall GS, Janda WM. Koneman's Color Atlas and Textbook of Diagnostic Microbiology, 7th ed. Wolters Kluwer; 2017.
Frequently Asked Questions
What's the difference between broth macrodilution and microdilution?
Why must the inoculum be standardized to a 0.5 McFarland standard?
Why are reference strains like E. coli ATCC 25922 run alongside patient isolates?
What happens if microdilution trays are stacked too high during incubation?
Can broth dilution MIC testing be automated?
Why might an MIC come back lower than clinically expected even with correct technique?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.