*Bacillus anthracis,*the most notorious pathogen of the genus Bacillus, is the causative agent of a serious zoonotic disease called **anthrax.**Anthrax is primarily a disease of wild and domestic herbivorous mammals. It is one of the most common agents of bioterrorismwhich was implicated previously in Sverdlovsk anthrax outbreak in 1979 and US postal system attack in 2001.
General properties
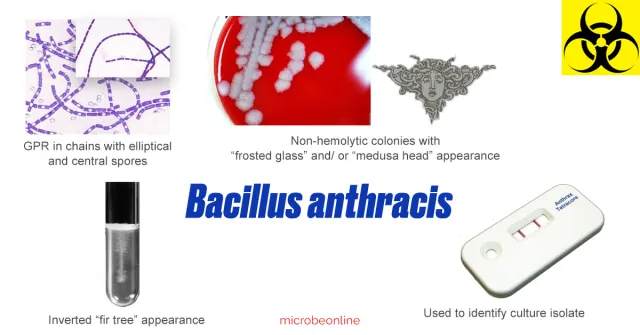
- Gram-positive, large rectangular rods arranged in chains
- Capsulated: B.anthracis has a polypeptide capsule, made up of polyglutamate (in contrast to the polysaccharide capsule present in most of the other capsulated bacteria). Capsulated bacilli are often square ended (“box-car”) in appearance.
- Endospore forming: B. anthracishas non-bulging spores; that are elliptical and centrally located.
- Non-motile, whereas other members of the genus are motile.
- Aerobes
Robert KochisolatedBacillus anthracisfor thefirst time in pure cultureand Koch’s postulates were made based onBacillus anthracis.Louis Pasteurpreparedfirst live attenuated bacterial vaccine, anthrax vaccine.
Pathogenesis and Clinical Presentations
Transmission
Both humans and animals acquire anthrax infection by ingestion, inhalation or traumatic inoculation of spores of *Bacillus anthracis.*The spores are dormant forms that are found in the soil or in contaminated animal products (e.g., hair or animal hides).
Virulence factorsofBacillus anthracis
Pathogenesis of anthrax is due to two plasmid-encoded virulence factors; anthrax toxin and capsule encoded in plasmid pXO1 and pXO2 respectively.
A: Anthrax toxin: It is a tripartite exotoxin, composed of three sub units:
Clinical presentations
Human anthrax is mainly divided into four clinical forms, depending up on the mode of acquisition. These forms are:
- Cutaneous anthrax: It accounts for 95-99% of cases worldwide. Infection results from direct inoculation of spores via small cuts or abrasions. The lesions (eschars) are generally found on exposed regions (e.g., hands, arms, neck, wrist, and face) of the body almost invariably accompanied by marked edema. The incubation period ranges from a few hours to 3 weeks, most often 2 to 6 days.
- Oropharyngeal/gastrointestinal anthrax: In oropharyngeal anthrax, lesions are seen in buccal cavity, tongue, tonsils or posterior pharyngeal wall whereas lesions are mostly seen in ileum and caecum in gastrointestinal anthrax. Symptoms include sore throat, dysphagia, vomiting, mild diarrhea and fever. These may be mild but are occasionally severe, progressing to haematemesis, bloody diarrhea, and massive ascites. The incubation period ranges from 3 to 7 days.
- **Inhalational (pulmonary) anthrax:**Symptoms of pulmonary anthrax include fever or chills, sweats, fatigue or malaise, non-productive cough, dyspnoea, changes in mental state including confusion, and nausea or vomiting. The incubation period ranges from 4-6 days.
- **Injectional anthrax:**This is a new form of anthrax reported from injectional-drug users. Symptoms may be similar to those of cutaneous anthrax, but there may be infection deep under the skin or in the muscle where the drug was injected. Injection anthrax can spread throughout the body faster and be harder to recognize and treat.
Despite its publicity as a potential agent of biologic warfare,B. anthracisis not highly contagious, so BSL 2 practices, containment equipment and facilities are appropriate for diagnostic tests.
Laboratory diagnosisof Anthrax
Sample
Sample should be collected before starting antibiotic treatment. The choice of the sample depends on the type of anthrax and clinical presentations. Commonly used specimens are pus, sputum, blood, CSF, gastric aspirate, and feces.
To isolateBacillus anthracisfrom environmental samples,heat or alcohol shockshould be given before plating on culture media. The shock will allow only thespore-forming bacillito survive, thus aiding as an enrichment technique.
Direct demonstration
- Gram staining: Reveals Gram-positive, large, rectangular rods. Spores are usually not seen in clinical specimens.
- McFadyean’s reaction: Polypeptide capsule can be demonstrated by staining with Gurr’s polychrome methylene blue stain for 30 seconds. Capsule appears as amorphous purple material surrounding blue bacilli. This is used for the presumptive diagnosis of animal anthrax.
- Direct immunofluorescence test (direct-IF): It detects capsular and cell wall polypeptide antigens by using fluorescent-tagged monoclonal antibodies. It is used for confirmation of the diagnosis during bioterrorism outbreaks.
- Ascoli’s thermoprecipitation test: It is a ring precipitation test, done when the sample is received in putrid form and bacilli are likely to be non-viable. Tissue samples are grounded in saline, boiled and filtered. This antigenic extract is layered over anthrax antiserum on a narrow capillary tube. A ring of precipitate appears at the junction of two liquids within 5 minutes.
Culture
Bacillus anthracis is aerobic, non-fastidious, grows in ordinary media and has a wide temperature range (12-45**°**C) of growth. Sporulation is promoted at 25-30°C and in the presence of unfavorable conditions such as distilled water, 2% NaCl, oxalate, and oxygen.

Colony morphologyof B. anthracis after 24 hours of incubation is as follows:
Blood agar
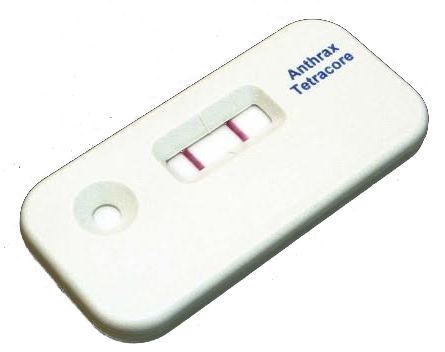
Bacillus anthracis produces dry wrinkled, non-hemolytic colonies with frosted glass appearance after overnight incubation on sheep blood agar. Occasionally the colonies may have fringed edges or put out curled protrusions (tailing). This is the so-called “Medusa head appearance” but is not encountered as frequently as textbooks often suggest, and varies from batch-to-batch of media. Non-hemolytic Bacillus colonies can be presumptively identified using ‘Red Line Alert Test‘, which is an immunochromatographic testfor the detection of surface protein found in Bacillus anthracis vegetative cells.
Medusa head appearance: When colonies are viewed under a low power microscope, the edge of the colony which is composed of long interlacing chains of bacilli, appears as locks of matted hair.
Gelatin stab
Growth occurs as inverted fir tree appearance (due to liquefaction of gelatin which occurs maximum at the surface, and then slows down towards the bottom).
Selective media
- Solid medium with penicillin: Colonies have a string of pearl appearance look (due to cells becoming larger and spherical because of their weaker cell walls under the action of penicillin, and cells tend to occur in a chain on the surface of agar).
- PLET medium: It consists of polymyxin, lysozyme, EDTA and thallous acetate added in heart infusion agar. It has been devised to isolate B. anthracis from mixtures of other spore-bearing bacilli.
Gram staining of the culture smear, reveals bamboo stick appearance, i.e. a long chain of gram-positive bacilli with non-bulging spores (appear as empty space).
Serology
Antibodies appear in convalescent sera and can be detected by ELISA or indirect hemagglutination methods.
Molecular diagnosis
PCR with specific primers can be used for further confirmation.
References and further readings
- Anthrax| CDC. (2019, February 19).
- Information, N. C. for B., Pike, U. S. N. L. of M. 8600 R., MD, B., & Usa, 20894. (2008). Laboratory procedures for diagnosis of anthrax, and isolation and identification of Bacillus anthracis. InAnthrax in Humans and Animals. 4th edition. World Health Organization.
- Procop, G. W., & Koneman, E. W. (2016). Koneman’s Color Atlas and Textbook of Diagnostic Microbiology (Seventh, International edition). Lippincott Williams and Wilkins.
- Tille, P. (2017). Bailey & Scott’s Diagnostic Microbiology (14 edition). Mosby.