Plasmodium and Malaria: Life Cycle, Pathogenesis, and Laboratory Diagnosis
Plasmodium life cycle, pathogenesis, and lab diagnosis explained: falciparum vs vivax, why only rings show on a smear, hypnozoites, relapse vs recrudescence.
A 26-year-old woman from rural Bihar presents to the district hospital with three days of high fever, rigors, and headache. Her temperature spikes every 48 hours like clockwork. The attending physician suspects malaria but which species? The answer changes everything: Plasmodium vivax means she needs a radical cure with primaquine to prevent relapse from dormant liver stages; Plasmodium falciparum means she is at risk of cerebral malaria and needs artemisinin-based combination therapy immediately. The laboratory has one job: tell the clinician which parasite it is, and fast.
This is why understanding the Plasmodium life cycle is not academic memorisation. Every stage you learn connects directly to a clinical decision, a drug target, or a diagnostic clue.
What Is Plasmodium?
Plasmodium is a genus of obligate intracellular protozoan parasites belonging to the phylum Apicomplexa. Five species cause malaria in humans. Four are long-established human parasites:
- Plasmodium falciparum causes malignant tertian malaria; the most dangerous
- Plasmodium vivax causes benign tertian malaria; most widely distributed
- Plasmodium malariae causes quartan malaria; 72-hour fever cycle
- Plasmodium ovale causes mild tertian malaria; rare
A fifth species, Plasmodium knowlesi naturally infects long-tailed and pig-tailed macaques in Southeast Asia and infects humans through the same Anopheles vectors. Its 24-hour erythrocytic cycle produces daily (quotidian) fever and allows parasitemia to rise very fast, so it can progress to severe disease within days. The diagnostic trap is what makes it dangerous: on microscopy P. knowlesi closely resembles P. malariae, including band-form trophozoites, and early rings can be mistaken for P. falciparum. Since P. malariae is benign and P. knowlesi is not, a "P. malariae" diagnosis in a patient from Malaysian Borneo or elsewhere in Southeast Asia should be treated as P. knowlesi until PCR proves otherwise.
Plasmodium has two hosts: the human (intermediate host, where asexual replication occurs) and the female Anopheles mosquito (definitive host, where sexual reproduction is completed). This distinction matters for the exam: the definitive host is always where sexual reproduction occurs.
Life Cycle of Plasmodium
The life cycle has three phases, each clinically relevant.
Phase 1: Pre-Erythrocytic (Hepatic) Schizogony: in the human liver
(Asymptomatic phase)
When an infected female Anopheles mosquito bites a human, it injects sporozoites into the bloodstream. Within 30–60 minutes, sporozoites travel to the liver and invade hepatocytes.
Inside hepatocytes, sporozoites develop into liver schizonts (exo-erythrocytic schizonts) and multiply asexually. Each schizont ruptures, releasing thousands of merozoites into the bloodstream to invade red blood cells.
Critical species difference: the dormant liver stage: In P. vivax and P. ovale, some sporozoites do not immediately develop into schizonts. Instead, they become dormant forms called hypnozoites in hepatocytes. These can reactivate months or years later, causing relapse. This is why patients with vivax malaria need primaquine (to kill hypnozoites) in addition to chloroquine because without it, the liver reservoir persists.
P. falciparum and P. malariae have no hypnozoite stage, so true relapse does not occur. (Recrudescence i.e. reappearance from surviving blood-stage parasites can occur in P. falciparum.)
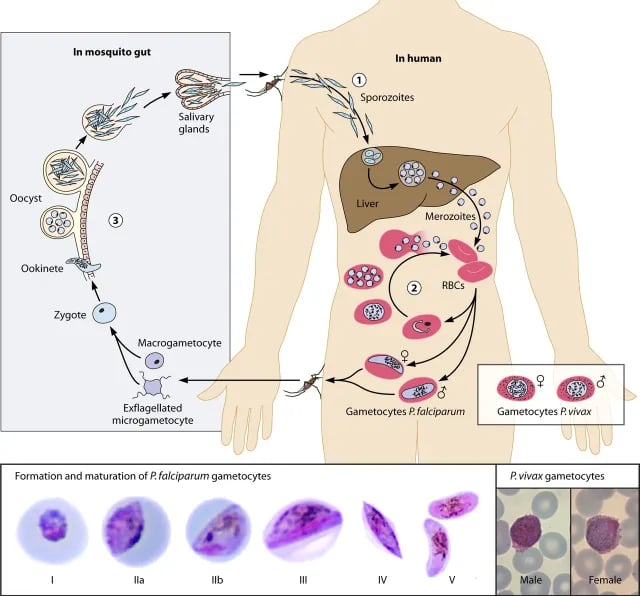 Figure: Life cycle of Plasmodium falciparum
Figure: Life cycle of Plasmodium falciparum
Timing of pre-erythrocytic phase:
| Species | Incubation in liver |
|---|---|
| P. falciparum | 6 days (single cycle, ~40,000 merozoites/schizont) |
| P. vivax | 8 days |
| P. ovale | 9 days |
| P. malariae | 13–16 days |
Phase 2: Erythrocytic Schizogony: in the red blood cells
(Symptomatic phase)
Merozoites released from the liver invade RBCs and progress through several stages:
Ring stage (early trophozoite) → Growing trophozoite → Schizont → Rupture → merozoites released → reinvade new RBCs
The rupture of RBCs releases merozoites, malarial pigment (hemozoin), and toxic waste products into the bloodstream — this is what triggers the characteristic fever paroxysm.
Why the fever is periodic: Because erythrocytic schizogony is synchronized across millions of RBCs, they rupture together in waves. The periodicity depends on the species:
- P. falciparum, P. vivax, P. ovale: 48-hour cycle → fever every 3rd day (tertian)
- P. malariae: 72-hour cycle → fever every 4th day (quartan)
- P. knowlesi: 24-hour cycle → daily fever (quotidian)
Where in the body does erythrocytic schizogony happen? This is a key exam distinction:
- P. vivax: erythrocytic schizogony occurs mainly in peripheral circulation, therefore all stages (rings, trophozoites, schizonts, gametocytes) are visible on peripheral blood smear.
- P. falciparum: erythrocytic schizogony of mature forms occurs inside capillaries of internal organs (spleen, liver, bone marrow). Therefore, only ring forms are found in the peripheral blood under normal circumstances. Mature trophozoites and schizonts are sequestered and this sequestration causes the severe complications of falciparum malaria (cerebral malaria, placental malaria).
Which RBCs does each species prefer?
| Species | RBC preference | Effect |
|---|---|---|
| P. vivax | Young RBCs (reticulocytes) | Low parasitemia (only 1–2% RBCs infected) |
| P. ovale | Young RBCs | Low parasitemia |
| P. malariae | Old RBCs | Low parasitemia |
| P. falciparum | No preference (young + old) | High parasitemia possible; more RBC destruction |
Phase 3: Gametogony: back in the human blood, completed in the mosquito
Some merozoites, instead of continuing asexual replication, develop into gametocytes (sexual forms) within RBCs. These gametocytes are taken up by a feeding female Anopheles mosquito.
Inside the mosquito midgut:
- Gametocytes → gametes → fertilization → zygote → ookinete → oocyst (in mosquito gut wall) → sporozoites → migrate to salivary glands → ready to infect the next human host
The mosquito is the definitive host because sexual reproduction (syngamy) occurs here.
Gametocytes of diagnostic importance: Mature P. falciparum gametocytes are crescent or banana-shaped, and no other human Plasmodium species produces this form. Seeing one on a smear effectively settles the species. The qualifier matters: only the mature (stage V) gametocyte is crescentic. Immature falciparum gametocytes are sequestered in bone marrow and are not seen on a peripheral smear at all, which is why crescents typically appear a week or more into the illness rather than at presentation.
This is one of the single most reliable microscopic clues on the exam and in the field.

Why It Matters: Pathogenesis
Why P. falciparum is the killer
Three mechanisms make P. falciparum uniquely dangerous:
- Cytoadherence and sequestration. Infected RBCs express PfEMP1 (P. falciparum erythrocyte membrane protein 1) on their surface, causing them to stick to endothelial cells of capillaries. This blocks microcirculation in the brain (cerebral malaria), the placenta (placental malaria, causing low birth weight and fetal loss), and the kidneys (acute kidney injury).
- High parasitemia. Because P. falciparum invades all RBC ages, it can infect a much higher percentage of circulating red cells than other species, leading to severe anemia and metabolic complications.
- No exo-erythrocytic (hypnozoite) stage, but rapid multiplication. While it does not relapse, it multiplies faster and more aggressively than other species.
Why P. vivax relapses but P. falciparum does not
The hypnozoite reservoir in the liver is the key. Primaquine targets hypnozoites (exo-erythrocytic forms). It is the only drug with this action and is essential for radical cure of vivax and ovale malaria. Without it, a patient can appear cured (blood-stage cleared) and relapse months later from liver reactivation.
Why the fever paroxysm feels like it does
The classic cold stage → hot stage → sweating stage sequence corresponds to:
- Cold stage: merozoites invade RBCs, host vasoconstricts
- Hot stage: RBCs rupture, merozoites and hemozoin released, TNF-α and IL-6 spike → fever 41°C+
- Sweating stage: thermoregulation kicks in, temperature falls, patient feels exhausted
Laboratory Diagnosis of Malaria
When to collect the blood sample
Blood should be collected during or just after the onset of fever because this is when the highest number of parasites are present in the peripheral blood. Collecting during an afebrile period reduces sensitivity significantly.
1. Peripheral Blood Smear is the Gold Standard
Thick and thin blood smears stained with Giemsa (WHO recommended) remain the gold standard for malaria diagnosis.
- Thick smear: Dehemoglobinized layer of lysed RBCs — used for screening (higher sensitivity, detects low parasitemia). Cannot be used for species identification.
- Thin smear: Single layer, RBC morphology preserved — used for species identification and quantifying parasitemia.
→ For full procedure and smear preparation, see: Thick and Thin Blood Smear for Malaria Diagnosis
Species identification on smear — key microscopic features:
| Feature | P. falciparum | P. vivax | P. malariae | P. ovale |
|---|---|---|---|---|
| RBC size | Normal/small | Enlarged (up to 2×) | Normal/small | Slightly enlarged, oval |
| RBC inclusions | Maurer's dots (6–12, brick-red) | Schüffner's dots (stippled) | Ziemann's dots (rare) | James's dots (like Schüffner's) |
| Trophozoite form | Appliqué/accolé (ring at RBC margin); multiple rings/RBC | Amoeboid, irregular | Band form (across RBC) | Compact |
| Gametocyte | Crescent/banana-shaped (mature forms only) | Round/oval | Round/oval | Round/oval |
| Stages in peripheral blood | Ring forms only (schizonts rare, only in severe disease) | All stages | All stages | All stages |
| % RBCs infected | Can exceed 10% (severe: >5% in low-transmission settings) | <1–2% | <1% | <1% |
2. Quantitative Buffy Coat (QBC)
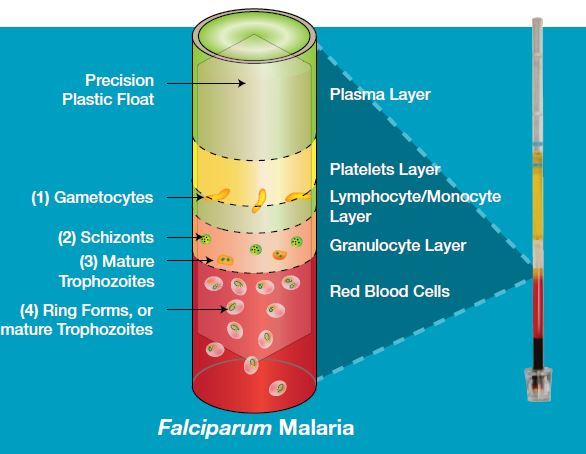 Figure: Falciparum malaria in QBC Test
Figure: Falciparum malaria in QBC Test
Uses acridine orange to fluorescently stain nucleic acids in parasitized RBCs. Centrifuged in a microhematocrit tube; parasites concentrate at the buffy coat layer and fluoresce under UV light.
- Sensitivity: 5.5–7% more sensitive than Giemsa thick film
- Detects as few as 1 parasite/μL of blood
- Limitation: requires fluorescence microscope; cannot reliably identify species
→ See dedicated article: Quantitative Buffy Coat (QBC) Test
3. Rapid Diagnostic Tests (RDTs)
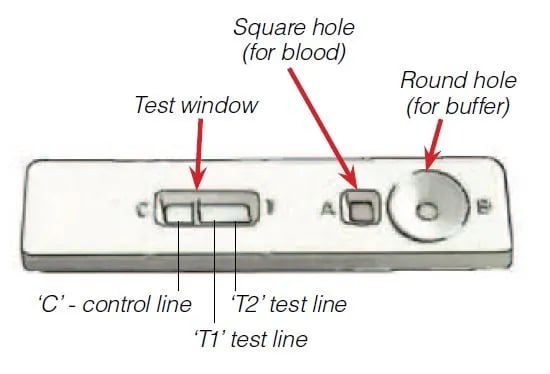 Figure: RDT for Malaria Diagnosis
Figure: RDT for Malaria Diagnosis
RDTs detect malaria antigens from a finger-prick blood sample. Results in 15 minutes. Three main targets:
- HRP-2 (histidine-rich protein 2) which is specific to P. falciparum
- pLDH (parasite lactate dehydrogenase) which is pan-specific or species-specific isoforms
- Aldolase which is also pan-specific
Interpreting a dual-line RDT (T1/T2 format):
- T1 line only (+ C): P. falciparum detected
- T2 line only (+ C): Non-falciparum species (P. vivax, P. malariae, P. ovale) or mixed infection
- Both T1 and T2 (+ C): P. falciparum + non-falciparum co-infection
RDTs do not replace microscopy because microscopy is still needed to quantify parasitemia and confirm species when species-differentiation affects treatment.
→ Full procedure: RDTs for Malaria Diagnosis
4. Serology
Indirect fluorescent antibody (IFA) tests and ELISA can detect anti-malarial antibodies but they have limited clinical value in endemic areas. Antibodies persist after cleared infection and cannot distinguish active from past disease. Main uses: blood donor screening and epidemiological surveys.
5. Molecular Diagnosis (PCR)
PCR amplifies parasite DNA from blood; can detect as few as 5–10 parasites/μL. Highest sensitivity and can definitively identify all five species including P. knowlesi. Not approved for routine clinical use in most settings; used for reference laboratory confirmation and research.
How to Remember
The FALCIPARUM mnemonic
Use the word F-A-L-C-I-P-A-R-U-M as a checklist of what makes falciparum special:
Letter | Content |
|---|---|
F | Fatal and Fast. Malignant tertian malaria; shortest pre-erythrocytic phase at 6 days |
A | Appliqué / accolé forms. Ring sitting on the RBC margin, partly outside the cell outline AL: All RBC ages infected (not selective) |
L | Lots of merozoites per schizont (around 40,000, the highest of any species) |
C | Crescent gametocytes. Mature forms only; no other human species makes them |
I | Internal organs. Mature forms sequester in deep capillaries |
P | Peripheral blood shows rings only. The visible consequence of I |
A | All ages of RBC invaded. No preference for young or old cells |
RU | RBC size Unaltered. Contrast P. vivax, which enlarges the cell up to twice normal |
M | Multiple rings per cell (2 to 6), Maurer's dots (not Schüffner's) |
Some elaboration:
- I and P together. The I and P entries are the same phenomenon seen from two sides. Infected cells express PfEMP1 and stick to capillary endothelium, so mature forms never return to circulation. That is why only rings appear on a peripheral smear, and it is also why falciparum causes cerebral and placental malaria. If you understand one, you have the other for free.
- A and M together. P. falciparum invades red cells of any age, so at high parasite loads a single cell may receive several merozoites. Multiple rings per cell and the ability to reach parasitemia above 5 percent both follow from that one property.
- L. A single falciparum liver schizont releases roughly 40,000 merozoites, against about 10,000 for P. vivax. Combined with indiscriminate RBC invasion, this is why falciparum parasitemia rises so much faster than the other species.
Remembering the hypnozoite rule
"ViVO stays alive" — Vivax and Ovale have hypnozoites (they stay alive in the liver). Falciparum and Malariae do not.
Where Students Actually Get Confused
1. "Does P. falciparum relapse?" No. Recrudescence (parasites surviving at sub-detectable levels in blood and re-emerging) can happen but this is not relapse. True relapse means reactivation from a liver hypnozoite. P. falciparum has no hypnozoites, therefore no true relapse. Only P. vivax and P. ovale relapse.
2. "Why do I only see ring forms for P. falciparum?" Because mature trophozoites and schizonts of P. falciparum are sequestered in deep capillaries of the spleen, liver, and brain, they never reach peripheral circulation. If you see mature falciparum schizonts on a peripheral smear, this is a sign of severe, late-stage disease (parasites spilling out of sequestration) and a medical emergency.
3. "Which is the definitive host — human or mosquito?" The mosquito. The definitive host is where sexual reproduction occurs. In the mosquito midgut, gametocytes form gametes, fertilize, and produce the zygote. The human is the intermediate host (asexual schizogony).
4. "What is the difference between relapse, recrudescence, and re-infection?"
- Relapse: Hypnozoites in liver reactivate → new blood-stage infection → new fever (P. vivax, P. ovale only)
- Recrudescence: Residual blood-stage parasites (survived below detection) re-multiply (P. falciparum, P. malariae)
- Re-infection: New mosquito bite with new sporozoites (any species)
5. "Schüffner's dots vs Maurer's dots — which is which?" P. vivax → Schüffner's dots (the "S" in vivax's dotted RBC, or remember: vivax = S for Stippled). P. falciparum → Maurer's dots (fewer, larger, brick-red). The word "FALCIPARUM" contains no letter S — a useful memory trick from the mnemonic above.
6. "The fever chart: tertian vs quartan?" Tertian = fever on day 1, day 3, day 5 (every 48 hours, but counted inclusively; so the gap feels like every other day). Quartan = fever on day 1, day 4, day 7 (every 72 hours). The terminology is archaic but the exam still uses it.
Key Exam Facts in One Table
| Fact | Detail | Memory Hook |
|---|---|---|
| Definitive host | Female Anopheles mosquito | MOSquito = DEFinitive (sexual repro) |
| Intermediate host | Human | Asexual schizogony; erythrocytic cycle |
| Species causing relapse | P. vivax, P. ovale | "ViVO stays alive" (hypnozoites) |
| Species with crescent gametocytes | P. falciparum only | One crescent on smear = falciparum confirmed |
| Peripheral blood stages: falciparum | Ring forms only | P. falciparum is shy — hides mature forms |
| Peripheral blood stages: vivax | All stages | P. vivax is sociable |
| RBC enlargement | P. vivax, P. ovale enlarge RBC up to 2× | Falciparum = RBC unaltered (the U in FALCIPARUM) |
| RBC inclusions | Schüffner's (vivax/ovale); Maurer's (falciparum) | FALCIPARUM has no S → no Schüffner's |
| Fever periodicity: falciparum/vivax/ovale | 48 hours (tertian) | 48-hour RBC rupture cycle |
| Fever periodicity: malariae | 72 hours (quartan) | Malariae = slower |
| Multiple ring forms per RBC | P. falciparum only | 2–6 rings per cell (the M in FALCIPARUM) |
| Appliqué/accolé forms | P. falciparum only | Ring at RBC margin, partial outside |
| Gold standard diagnosis | Thick + thin smear, Giemsa stain | Cannot be replaced by RDT alone |
| HRP-2 antigen | P. falciparum specific | HRP-2 = Histidine Rich Protein, falciparum only |
| pLDH antigen | Pan-specific (all species) | pLDH = parasite LDH (all plasmodia have it) |
| Primaquine: why needed for vivax | Kills hypnozoites in liver | Blood-stage cure ≠ radical cure without primaquine |
| P. knowlesi | Macaque parasite; humans infected in SE Asia | 24-hour cycle; can be severe |
References
- Forbes, B. A., Sahm, D. F., & Weissfeld, A. S. (2007). Bailey & Scott's Diagnostic Microbiology (12th ed.). Mosby Elsevier.
- Levinson, W. (2016). Review of Medical Microbiology and Immunology (14th ed.). McGraw-Hill.
- Venugopal, K., Hentzschel, F., Valkiūnas, G., et al. (2020). Plasmodium asexual growth and sexual development in the haematopoietic niche of the host. Nature Reviews Microbiology, 18, 177–189. https://doi.org/10.1038/s41579-019-0306-2
- Talman, A. M., Domarle, O., McKenzie, F. E., et al. (2004). Gametocytogenesis: the puberty of Plasmodium falciparum. Malaria Journal, 3, 24. https://doi.org/10.1186/1475-2875-3-24
- Menkin-Smith, L., & Winders, W. T. (2023). Plasmodium vivax Malaria. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK538333/
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- World Health Organization. (2023). Guidelines for malaria. WHO. https://www.who.int/publications/i/item/guidelines-for-malaria
- Arbeitskreis Blut, Untergruppe «Bewertung Blutassoziierter Krankheitserreger». (2009). Malaria. Transfusion Medicine and Hemotherapy, 36(1), 48–60. https://doi.org/10.1159/000197327
Frequently Asked Questions
Which Plasmodium species causes the most dangerous form of malaria?
Why does Plasmodium vivax malaria relapse but P. falciparum does not?
What is the gold standard for malaria diagnosis?
What is the significance of crescent-shaped gametocytes on a blood smear?
Why are only ring forms seen in the peripheral blood smear of P. falciparum malaria?
What is the difference between the definitive and intermediate host of Plasmodium?
What does HRP-2 detect and which species is it specific for?
Why is primaquine needed to treat P. vivax but not P. falciparum malaria?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.