Mucormycosis: Etiology, Pathogenesis, Clinical Features, Diagnosis and Treatment
Mucormycosis (black fungus): etiology, Rhizopus and Mucor characteristics, pathogenesis, clinical manifestations by organ system, laboratory diagnosis (KOH, histopathology, culture, PCR), and treatment.
Mucormycosis (previously called zygomycosis or phycomycosis); widely known as "black fungus disease" following its dramatic resurgence in India during the COVID-19 pandemic is a rapidly destructive, necrotizing fungal infection caused by the mucormycetes group of fungi. It is the third most important invasive mycosis after candidiasis and aspergillosis, carrying an overall mortality rate of approximately 50%.
Why "black fungus" is a misnomer: Mucorales are hyaline (colorless) fungi, not black. The name likely originated from the black, necrotic tissue characteristic of advanced rhinocerebral disease. True "black fungi" causing tinea nigra, chromoblastomycosis, and phaeohyphomycosis are entirely different organisms.
Etiology and Causative Organisms
Mucormycosis is caused by a group of fungi from the order Mucorales, collectively called mucormycetes, including the genera: Rhizopus, Mucor, Lichtheimia, Rhizomucor, Cunninghamella, Saksenaea, Apophysomyces, Cokeromyces, Actinomucor, and Syncephalastrum.
Rhizopus arrhizus (formerly Rhizopus oryzae) is the single most common etiological agent, responsible for approximately 60% of mucormycosis cases worldwide.
Rhizopus and Mucor are one of five medically important opportunistic fungal genera alongside Candida, Cryptococcus, and Aspergillus — and are widely distributed saprophytic molds found in soil and decaying vegetation worldwide.
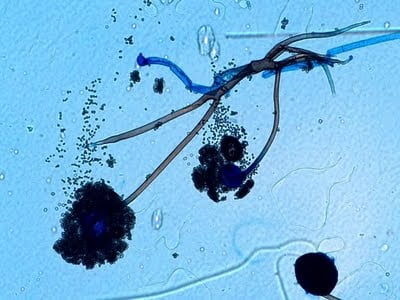 Figure: Mature sporangium of Rhizopus releasing sporangiospores
Figure: Mature sporangium of Rhizopus releasing sporangiospores
General Characteristics of Mucorales
- These saprophytic molds are not dimorphic — they exist only in mold form, both in the environment and in tissue
- Hyphae are non-septate (aseptate) with characteristic right-angle (90°) branching . This single feature distinguishes them microscopically from Aspergillus, which has septate hyphae with acute-angle (45°) branching
- Culture produces a fluffy, cotton-candy-like mold, typically with black or dark sporangia
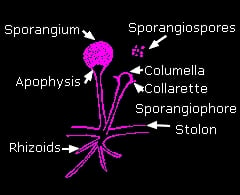
- Conidia (sporangiospores) are enclosed within a sac called the sporangium
- The sporangium forms at the tip of a supporting structure called the sporangiophore
Genus identification based on culture morphology
| Organism | Best growth temp | Sporangiophore | Apophysis | Columella | Sporangium | Rhizoids |
|---|---|---|---|---|---|---|
| Rhizopus sp. | 37°C | Non-branched, brown | Not prominent | Spherical | Spherical | Abundant, well developed |
| Mucor sp. | <37°C | Branched/non-branched, hyaline | Absent | Varying shapes | Spherical | Absent |
| Lichtheimia (Absidia) sp. | 37°C | Branched, hyaline | Conical | Dome-shaped | Pear-shaped | Primitive, rare |
| Rhizomucor sp. | 20–60°C | Branched, brown | Absent | Spherical | Spherical | Primitive, rare |
| Apophysomyces sp. | 24–42°C | Non-branched, brown | Bell-shaped | Rarely elongated | Pear-shaped | Tuft, from a foot cell |
| Mortierella sp. | >40°C | Branched, hyaline | Absent | Absent | Spherical | Primitive |
The key distinguishing feature: Mucor has a columella but no apophysis, whereas Lichtheimia has both a columella and an apophysis. The presence or absence of rhizoids (root-like structures) and their position relative to the sporangiophore is also diagnostic — Rhizopus has abundant, well-developed rhizoids directly beneath the sporangiophore.
 Risk Factors and Predisposing Conditions
Risk Factors and Predisposing Conditions
Mucormycosis is acquired through inhalation of airborne spores, percutaneous inoculation, or ingestion. Healthy hosts clear these spores efficiently through mononuclear and polynuclear phagocytes — disease occurs almost exclusively when this first-line defence is compromised.
Major predisposing conditions:
- Diabetes mellitus (especially with ketoacidosis) — the single most important risk factor, particularly for rhinocerebral disease
- Severely immunocompromised patients (cancer, HIV/AIDS)
- Immunosuppression from corticosteroid use — including the COVID-19-associated mucormycosis surge driven by widespread steroid use for severe COVID-19
- Hematological malignancies
- Hematopoietic stem cell or solid organ transplantation
- Intravenous drug use
- Neonatal prematurity and malnutrition
- Burns and trauma (for cutaneous disease, even in immunocompetent hosts)
Pathogenesis
Mucormycetes enter the body by inhalation of airborne spores (most common), percutaneous inoculation through skin breaks, or ingestion. In healthy individuals, phagocytes destroy the spores before germination. In immunocompromised hosts, spores germinate into hyphae that exhibit a hallmark behavior: angioinvasion — invasion of blood vessel walls.
This vascular invasion causes thrombosis and subsequent infarction and necrosis of the surrounding tissue — the mechanism behind the rapid, destructive tissue death characteristic of this infection. In diabetic patients, sinus spores germinate and invade the blood vessels supplying the brain, producing rhinocerebral disease.
Clinical Manifestations by Site of Infection
Rhinocerebral mucormycosis
The most common presentation, particularly in patients with uncontrolled diabetes mellitus, kidney transplant, or leukemia. Infection begins in the sinuses and can progress to the orbit and intracranial structures.
Symptoms: One-sided facial swelling, headache, nasal or sinus congestion, black necrotic lesions on the nasal bridge or hard palate that progress rapidly, fever.
Pulmonary mucormycosis
The second most common presentation, following inhalation of spores. Most common in patients with hematological malignancy and neutropenia, or following transplantation.
Symptoms: Fever, cough, chest pain, shortness of breath. Radiologically and clinically very difficult to distinguish from invasive aspergillosis — both show vascular invasion, thrombosis, and tissue necrosis on imaging.
Gastrointestinal mucormycosis
Acquired through ingestion of spores — from fermented foods, dried bread, fermented porridges, or contaminated tongue depressors. Most commonly affects the stomach, followed by colon, small intestine, and esophagus.
Symptoms: Abdominal pain, nausea and vomiting, gastrointestinal bleeding.
Cutaneous mucormycosis
The most common form in immunocompetent hosts — acquired by direct inoculation through skin breaks (surgery, burns, trauma, contaminated dressings or insulin injection sites). Healthcare-associated outbreaks have been traced to contaminated adhesive tape and wooden tongue depressors.
- Primary cutaneous disease — direct inoculation
- Secondary cutaneous disease — dissemination from another site (often rhinocerebral); further classified as localized, deep, or disseminated
Symptoms: Erythema and induration at the inoculation site progressing to a characteristic black eschar with central ulceration; pain, warmth, swelling.
Disseminated mucormycosis
Involves two or more non-contiguous organ systems, spreading hematogenously. Mortality of disseminated cutaneous mucormycosis reaches 90–100%.
Symptoms: Non-specific, varying by site — mental status changes or coma with cerebral involvement; erythematous lesions with cutaneous dissemination.
Other clinical manifestations
- Endocarditis (native or prosthetic valves)
- Osteomyelitis (typically adjacent to other mucormycosis sites)
- Peritoneal mucormycosis (in continuous ambulatory peritoneal dialysis patients)
- Isolated CNS mucormycosis (immunocompromised patients; IV drug users)
- Renal mucormycosis (IV drug use; contaminated central venous catheters)
Laboratory Diagnosis
Mucormycosis is frequently misdiagnosed because of non-specific symptoms and radiological features that overlap significantly with invasive aspergillosis. A high index of suspicion combined with prompt laboratory confirmation is essential — delayed diagnosis directly increases mortality.
Specimen collection
Specimen type depends on clinical presentation: skin scrapings (cutaneous lesions), nasal discharge and sinus aspirates (rhinocerebral disease), bronchoalveolar lavage and needle biopsy (pulmonary disease), and biopsy tissue (gastrointestinal or disseminated disease).
Direct microscopic examination
KOH wet mount provides rapid presumptive diagnosis and can be applied to virtually any specimen type. Supplementing KOH with fluorescent brighteners (Blankophor, Calcofluor white) significantly enhances hyphal visualization but requires a fluorescence microscope.
Characteristic microscopic findings: Thick-walled, refractile hyphae 6–15 µm in diameter (some sources report up to 25 µm), non-septate or sparsely septate, with swollen cells up to 50 µm, and wide-angle (90°) branching — the single most important distinguishing feature from Aspergillus, which shows septate hyphae with narrow-angle (45°) branching.
Critical action point: Any microscopic finding suggestive of Mucorales (Rhizopus, Mucor, Absidia) must be communicated to the clinical team immediately — these organisms are rapidly invasive and treatment delay directly worsens outcomes.
Histopathological examination
Tissue sections stained with H&E, Grocott methenamine-silver (GMS), or periodic acid-Schiff (PAS) reveal broad-based, ribbon-like, non-septate hyphae with wide-angle branching.
Histopathology serves a function direct microscopy cannot: it distinguishes true tissue pathogen invasion from culture contamination, and definitively demonstrates angioinvasion — the key pathogenic feature that confirms invasive disease rather than colonisation. It can also detect co-infection with other molds.
Culture
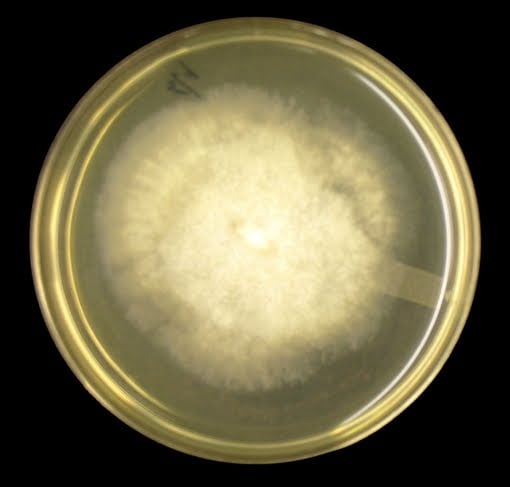 Figure: Mucor on SAB Agar plate 48hrs at 30°C
Figure: Mucor on SAB Agar plate 48hrs at 30°C
Culture provides definitive genus/species-level identification and enables antifungal susceptibility testing. Most medically important Mucorales are thermotolerant and grow rapidly (3–5 days) on Sabouraud dextrose agar or potato dextrose agar at 25–30°C.
Colonies are fluffy, white-grey-brown, filling a culture plate within 24–96 hours; the reverse remains pale. Colony morphology alone cannot distinguish between genera; sporangial morphology under microscopy (with lactophenol cotton blue staining) is required, examining sporangiophore branching, presence/absence of apophysis and columella, and rhizoid pattern.
Important limitations of culture:
- Culture positivity rate is low — a negative culture does not exclude mucormycosis
- Tissue grinding during specimen processing kills the fragile non-septate hyphae, reducing yield — gentle tissue handling is essential
- Necrotic tissue and exudates contain few viable organisms, requiring a heavy inoculum
- Because Mucorales can be laboratory contaminants, isolation from susceptible hosts should never be dismissed as contamination without clinical correlation
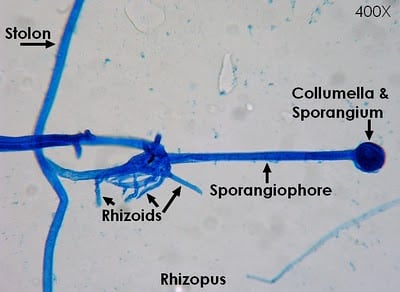 Figure: An adhesive tape preparation of Rhizopus stained with LPCB mount
Figure: An adhesive tape preparation of Rhizopus stained with LPCB mount
Serology
Antibody detection (ELISA, double diffusion, immunoblot) is not routinely used due to poor sensitivity/specificity, cross-reactivity with Candida and Aspergillus, and lack of clinical validation.
Molecular methods
- Conventional PCR targeting the internal transcribed spacer (ITS) region, sometimes combined with pan-fungal PCR and oligonucleotide array for species discrimination — highly sensitive but costly and labour-intensive
- PCR-RFLP targeting 18S rRNA — effective but expensive (restriction enzymes) and not in routine use
- DNA sequencing of the ITS region — efficient genus/species identification, applicable directly to extracted tissue DNA
- Semi-nested RT-PCR with high-resolution melt curve analysis targeting cytochrome B genes — high sensitivity for genus/species identification
- Emerging research on qPCR detection of circulating mucoralean DNA in blood (plasma/serum) or urine — promising for non-invasive, rapid diagnosis
[MALDI-TOF (automated proteomic identification)](https://microbeonline.com/maldi-tof-ms-principle-applications-microbiology/)
Well-established for bacterial and yeast identification but technically challenging for molds due to complex fungal structures, variable growth rates, and incomplete reference databases. Cost-effective in principle, but database enrichment and extraction protocol optimisation are still needed before routine clinical use.
Treatment
Successful treatment of mucormycosis depends on four pillars:
- Early diagnosis — the single most modifiable factor affecting survival
- Reversal of predisposing risk factors where possible (e.g. correcting diabetic ketoacidosis, reducing immunosuppression)
- Surgical debridement — extensive removal of necrotic tissue is essential to restore circulation and allow antifungal drug penetration; medical therapy alone is rarely sufficient
- Prompt antifungal therapy
Antifungal monotherapy
- Lipid formulations of amphotericin B (liposomal amphotericin B, amphotericin B lipid complex) are first-line — standard amphotericin B deoxycholate is more nephrotoxic
- Posaconazole is used as salvage therapy for patients refractory to or intolerant of polyenes
Critical prescribing point: Fluconazole, voriconazole, and itraconazole have no reliable activity against mucormycosis. Voriconazole — the first-line drug for invasive aspergillosis — is specifically ineffective here, which is why correctly distinguishing mucormycosis from aspergillosis is clinically critical, not just academic.
Combination and adjunctive therapy
- Polyene + caspofungin combination has shown significantly improved outcomes in rhino-orbital and rhino-orbital-cerebral disease compared to polyene monotherapy
- Deferasirox (iron chelator) + liposomal amphotericin B showed synergistic survival benefit in animal models — relevant because mucormycetes require iron for growth and patients with iron overload states are at higher risk
- Adjunctive immune therapy with recombinant G-CSF, GM-CSF, or IFN-γ enhances granulocyte ability to damage the organism and has been used successfully alongside lipid amphotericin B
Distinguishing Mucormycosis from Aspergillosis
These two invasive mold infections are frequently confused clinically, radiologically, and microscopically — but the distinction is treatment-critical because voriconazole (first-line for aspergillosis) does not work against mucormycosis.
| Feature | Mucormycosis | Aspergillosis |
|---|---|---|
| Hyphae septation | Non-septate (aseptate) | Septate |
| Branching angle | Wide angle (~90°) | Narrow/acute angle (~45°) |
| Hyphal width | Broad, ribbon-like, irregular | Uniform, narrower |
| First-line treatment | Lipid amphotericin B | Voriconazole |
| Angioinvasion | Yes — characteristic | Yes — also characteristic |
| Surgical debridement | Essential | Important but less universally critical |
→ Aspergillus: Morphology, Clinical Features, and Lab Diagnosis → KOH Preparation: Principle, Procedure, Results → Sabouraud Dextrose Agar (SDA) → Lactophenol Cotton Blue (LPCB) Mount → Dimorphic Fungi
References and Further Reading
- Bouza, E., Munoz, P., & Guinea, J. (2006). Mucormycosis: an emerging disease? Clinical Microbiology and Infection, 12(suppl 7), 7–23. https://doi.org/10.1111/j.1469-0691.2006.01604.x
- Centers for Disease Control and Prevention. Mucormycosis. https://www.cdc.gov/fungal/diseases/mucormycosis/
- Castrejón-Pérez, A. D., Welsh, E. C., Miranda, I., Ocampo-Candiani, J., & Welsh, O. (2017). Cutaneous mucormycosis. Anais Brasileiros de Dermatologia, 92(3), 304–311. https://doi.org/10.1590/abd1806-4841.20176614
- Spellberg, B., & Ibrahim, A. S. (2010). Recent advances in the treatment of mucormycosis. Current Infectious Disease Reports, 12(6), 423–429. https://doi.org/10.1007/s11908-010-0129-9
- Lass-Flörl, C. (2009). Zygomycosis: conventional laboratory diagnosis. Clinical Microbiology and Infection, 15(suppl 5), 60–65. https://doi.org/10.1111/j.1469-0691.2009.02999.x
- Lackner, M., Caramalho, R., & Lass-Flörl, C. (2014). Laboratory diagnosis of mucormycosis: current status and future perspectives. Future Microbiology, 9(5), 683–695. https://doi.org/10.2217/fmb.14.23
Frequently Asked Questions
Why is "black fungus" a misleading name for mucormycosis?
Why is diabetes mellitus the most important risk factor for mucormycosis?
How do you distinguish mucormycosis from aspergillosis on microscopy?
Why is surgical debridement essential, not optional, in mucormycosis treatment?
Why does culture have low positivity despite organisms being visible on microscopy?
Why don't fluconazole, voriconazole, and itraconazole work against mucormycosis?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.