Parasitic Infections: Classification, Sources, Modes of Transmission, and Prevention With Examples
How do parasites reach and infect humans? Understand all six transmission routes — feco-oral, skin penetration, vector-borne, vertical, blood transfusion, and autoinfection — with specific organism examples, a complete disease-vector table, and exam-ready mnemonics.
A child in rural Bangladesh develops a pot belly, stunted growth, and chronic fatigue. A woman in sub-Saharan Africa has recurrent fever every 48 hours. A hiker in Nepal returns with explosive diarrhoea three weeks after drinking from a mountain stream. A pregnant woman in Brazil passes an infection to her unborn child that she never knew she had.
Four patients. Four different parasites. Four completely different transmission routes. Understanding how each parasite reaches its human host and why it behaves the way it does — is the foundation of both clinical diagnosis and public health prevention. The same knowledge that explains why you should cook pork thoroughly also explains why cerebral malaria kills and intestinal worms do not.
A parasite is a living organism typically a protozoan, helminth (worm), or arthropod that lives on or within a host and derives nutrients at the host's expense, providing no benefit in return. Without a host, a parasite cannot live, grow and multiply. Therefore, a parasite normally doesn’t kill the host, but it can spread diseases, and some of these can be fatal. Parasites can be unicellular or multicellular and are often smaller than the host. Hookworm, bed bugs, lice, honey fungus, Entamoeba etc. are a few examples of parasites.
Types of parasites
Based on their location, parasites may be classified as:
Ectoparasite
Organisms that inhabit the surface of the body of the host without gaining access to internal tissues are called ectoparasites. For example, ticks, fleas, lice, and mites attach or burrow into the skin of humans.
Ectoparasites can survive on the host’s skin and cause skin irritations. Infection can range from asymptomatic to moderate itching. The infection by these parasites is called an infestation.
Some common ectoparasites of humans are:
Scabies (Sarcoptes scabiei)
Scabies mite burrows into the upper layer of the skin. They can intense itching and a pimple-like skin rash. Scabies outbreaks can occur in crowded living facilities such as nursing homes, dorm rooms, and prisons.
Bed bug (Cimex lectularius)
These are parasitic insects that feed solely on the blood of people and animals while they sleep. Bed bug infestations usually occur in apartments, shelters, rooming houses, hotels, cruise ships, buses, trains, and dorm rooms.
Fleas
Fleas are ectoparasites of humans. Their bites cause itching and irritation. They also serve as vectors for transmitting diseases like cat scratch disease, flea-borne typhus, and plague.
Ticks: Ticks are tiny blood-sucking ectoparasites. Common ticks are black-legged tick (Ixodes scapularis), lone star tick (amblyomma americanum), American dog tick (Dermacentor variabilis, D. similis), brown dog tick (Rhipicephalus sanguineus), groundhog tick (Ixodes cookei), gulf coast tick (Amblyomma maculatum), Rocky Mountain wood tick (Dermacentor andersoni), soft tick (Ornithodoros spp.), and western black-legged tick (Ixodes pacificus).
Common tick-borne diseases are Rocky Mountain spotted fever, Lyme disease, ehrlichiosis, babesiosis, and anaplasmosis. Ticks of the genus Ixodestransmit three infectious diseases: Lyme disease, ehrlichiosis, and babesiosis, whereas ticks of the genus Dermacentor transmit tularemia, Rocky Mountain spotted fever, and also Ehrlichiosis.
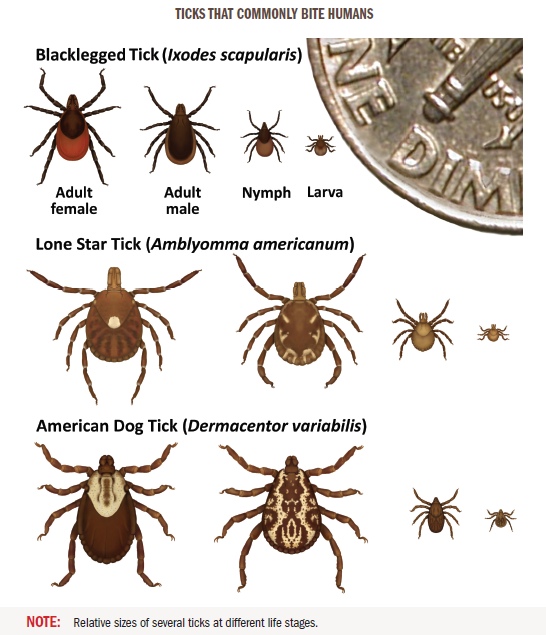 Figure: Ticks that common bite humans (Image source: CDC)
Figure: Ticks that common bite humans (Image source: CDC)
Human Lice: Human lice survive by feeding on human blood. Close person-to-person contact is needed for the transmission of lice infestations (pediculosis and pthiriasis). Three types of lice are found in the human body. They are
- Head louse (Pediculus humanus capitis)
- Body or clothes louse (Pediculus humanus corporis). Body lice also serve as vector for the transmission of epidemic typhus.
- “Crab” louse or pubic louse (Pthirus pubis)
Ectoparasites are important vectors for transmitting diseases such as spotted fever, typhus, ehrlichiosis, etc.
Endoparasite
Organisms that live within the host’s body (in the blood, tissues, body cavities, and other organs) are called endoparasites. Invasion by the endoparasite is called an infection. In humans, all pathogenic protozoan and helminthic parasites are endoparasites. For example, roundworm, hookworm, amoeba, etc.
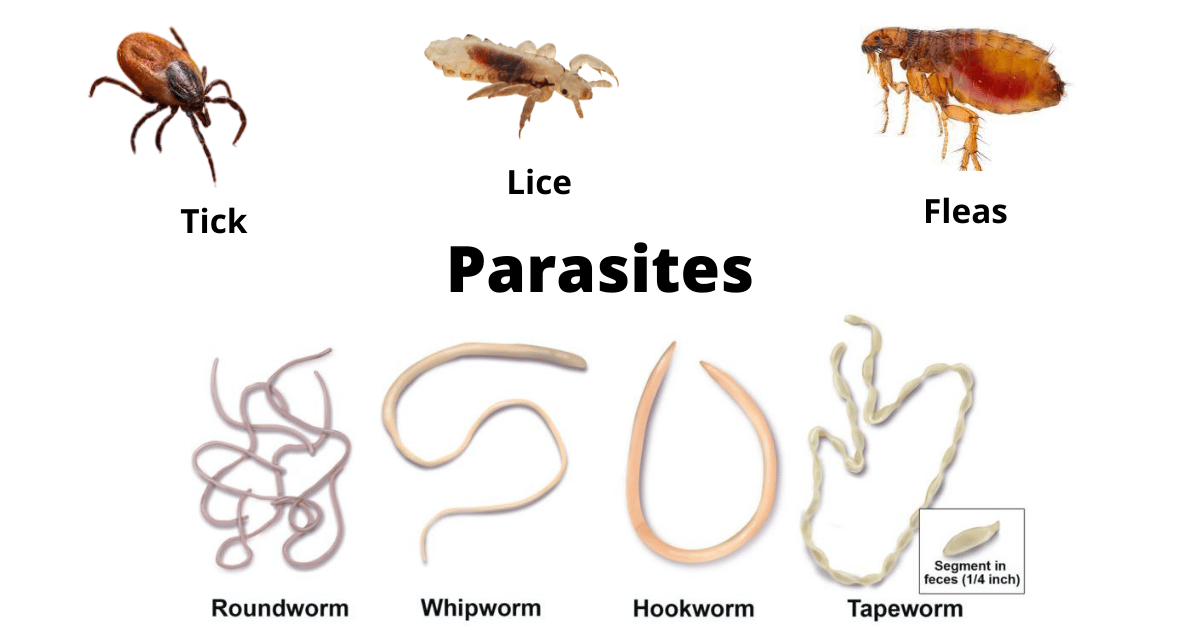 Figure: Various Ectoparasites and Endoparasites of Humans
Figure: Various Ectoparasites and Endoparasites of Humans
Endoparasites can be further subdivided into the following types based on their relation to the host.
- Obligate parasites: Parasites that complete a phase of their lifecycle in the host; therefore, without a host, they cannot complete their life cycle. For example, Plasmodium (malarial parasite), Toxoplasma gondii etc.
- Facultative parasites: Parasites that under favorable conditions, may live either a parasitic life or free-living life. Examples include Acanthamoeba, Naegleria fowleri etc
- Accidental parasites: Parasites that infect an unusual host. For example, Echinococcus granulosus is common in dogs but may infect humans accidentally.
- Aberrant parasites or wandering parasites: Parasites that infect a host where they cannot live or develop further (e.g., Toxocara in humans).
Why Transmission Routes Matter Clinically
Knowing how a parasite is transmitted is not academic — it directly determines three clinical decisions:
1. What to ask in the history. A patient presenting with eosinophilia and abdominal pain in Nepal: did they eat undercooked pork (Taenia solium)? Walk barefoot in soil (hookworm, Strongyloides)? Drink untreated water (Giardia, Entamoeba)? The transmission route narrows the differential immediately.
2. How to prevent reinfection. Treating a patient for hookworm without addressing barefoot walking on contaminated soil is a treatment that will fail within weeks. Prevention must target the route, not just the parasite.
3. Who else is at risk. Autoinfection-capable parasites (Strongyloides, Enterobius, Taenia solium) can produce escalating worm burden in a single host without reexposure. Vector-borne infections indicate a local transmission hotspot. Blood-transfusion-transmitted parasites have public health implications for blood banking.
Source of infection of parasites
Humans may acquire parasites from various sources, such as contaminated soil and water, food, and contact with
- Contaminated soil and water: Soil polluted with human excreta may contain eggs of the parasites (such as hookworm, Ascaris species, Strongyloides species, and Trichuris species) and is an important source of infection. Similarly, infection may occur by drinking water contaminated with human excreta-containing cysts of E. histolytica or Giardia lamblia.
- Raw or undercooked meat: Raw beef containing the larvae of Cysticercus bovis and pork containing Cysticercus cellulosae are examples where undercooked meat acts as a source of infection.
- Other sources of infection:
Aquatic source: Freshwater fishes (source of Diphyllobrothium latum), crab or crayfishes (source of Paragonimus westermanii), aquatic plants such as watercress (source of Fasciola hepatica)
Bloodsucking insects: Mosquitoes (source of Plasmodium, Wuchereria bancrofti), tsetse fly (source of Trypanosoma spp), sandflies (Leishmania spp)
Domestic animals: Animals such as cats (source of T.gondii) and Dog (source of E.granulosus), could also be the source of infection of parasites
Man: The human itself is the host to several parasites and can excrete infective stages (eggs and larvae) and become the source of parasites such as E.histolytica, G.lamblia, E.vermucularis, etc
Modes of Transmission
The infective stages of various parasites may be transmitted from one host to another in the following ways:
- The oral or feco-oral route is the most common mode of transmission of the parasites. Infection is transmitted orally by ingestion of food, water, or vegetables contaminated with feces containing the infective stages of the parasite, soiled fingers, etc. (e.g., cysts of E. histolytica, and ova of Ascaris lumbricoides)
- Penetration of the skin and mucous membranes: Infection is transmitted by the penetration of the larval forms of the parasite through unbroken skin (e.g., filariform larva of Strongyloides stercoralis and hookworm can penetrate through the skin of an individual walking bare-footed over fecally contaminated soil), or by the introduction of the parasites through insect bite of bloodsucking insect vectors (e.g., Plasmodium species, Leishmania species, and Wuchereria bancrofti)
- Physical and sexual contact: Parasites such as E. gingivalis is transmitted from person to person by kissing or drinking from contaminated drinking utensils. Parasite such as Trichomonas vaginalis is transmitted by sexual contact. Others such as Entamoeba, Giardia, and Enterobius are also transmitted rarely by sexual contact among homosexuals.
- Vertical transmission: Infections with Toxoplasma gondii, Plasmodium spp., and Trypanosoma cruzi may be transmitted transplacentally from an infected mother to a fetus.
- Blood transfusion: Certain parasites like Plasmodium species, Babesia species, Toxoplasma species, Leishmania species, and Trypanosoma species can be transmitted through the transfusion of blood or blood products.
- Autoinfection: Few intestinal parasites may be transmitted to the same person by contaminated hand (external autoinfection) or reverse peristalsis (internal autoinfection). It is observed in Cryptosporidium parvum, Taenia solium, Enterobius vermicularis, Strongyloides stercoralis, and Hymenolepis nana.
Autoinfection deserves special attention because it explains clinical phenomena that confuse students:
- External autoinfection (Enterobius vermicularis): The female pinworm migrates to the perianal area at night to lay eggs. Scratching transfers eggs to fingers → fingers to mouth → re-ingestion. This is why a single infected child can have a persistent, escalating infection despite treatment, and why the whole household must be treated simultaneously.
- Internal autoinfection (Strongyloides stercoralis): Rhabditiform larvae in the gut can transform into infective filariform larvae without leaving the host, penetrate the intestinal wall or perianal skin, and restart the migration cycle internally. In immunocompromised patients (HIV, corticosteroid therapy), this can produce hyperinfection syndrome — massive larval dissemination carrying gut bacteria into the bloodstream, causing fatal sepsis. Strongyloides is the only helminth that can maintain itself in a host indefinitely through autoinfection.
- Internal autoinfection (Taenia solium): If T. solium eggs are ingested (via contaminated hands or reverse peristalsis from the adult worm in the gut), they hatch and larvae migrate to tissues — including the brain — causing neurocysticercosis, the most common cause of acquired epilepsy in many LMIC settings. This is why T. solium tapeworm infection is far more dangerous than other tapeworm infections: you can give yourself cysticercosis.
Transmission Route Quick Reference
| Route | Key organisms | Infective stage | Clinical memory hook |
|---|---|---|---|
| Feco-oral | Entamoeba histolytica, Giardia lamblia, Ascaris lumbricoides, Trichuris trichiura, Taenia spp. | Cysts (protozoa); ova/eggs (helminths) | "Dirty hands, dirty water" |
| Skin penetration (active) | Hookworm (Ancylostoma, Necator), Strongyloides stercoralis | Filariform (L3) larvae | "Bare feet on contaminated soil" |
| Skin penetration (vector bite) | Plasmodium, Leishmania, Wuchereria bancrofti, Trypanosoma | Sporozoites; metacyclic promastigotes; L3 larvae; metacyclic trypomastigotes | "Insects inject infective stages" |
| Skin penetration (cercariae) | Schistosoma spp. | Cercariae (free-swimming in freshwater) | "Swimmer's itch" |
| Ingestion of infected meat | Taenia solium (pork), Taenia saginata (beef), Trichinella spiralis (pork), Toxoplasma gondii (undercooked meat/cat faeces) | Cysticerci; larvae; tissue cysts | "Cook it properly" |
| Ingestion of aquatic organisms | Diphyllobothrium latum (freshwater fish), Paragonimus westermani (crab/crayfish), Fasciola hepatica (watercress) | Plerocercoid larvae; metacercariae | "Freshwater foods" |
| Sexual/direct contact | Trichomonas vaginalis, Enterobius (rare), Entamoeba (rare) | Trophozoites; eggs | "Contact transmission" |
| Vertical (transplacental) | Toxoplasma gondii, Plasmodium, Trypanosoma cruzi | Tachyzoites; merozoites; trypomastigotes | "Mother to fetus" |
| Blood transfusion | Plasmodium, Babesia, Leishmania, Trypanosoma, Toxoplasma | Blood-stage forms | "Screen blood donors in endemic areas" |
| Autoinfection | Strongyloides stercoralis, Enterobius vermicularis, Taenia solium, Hymenolepis nana | Larvae (Strongyloides); eggs (Enterobius, Taenia) | "Reinfects same host — no new exposure needed" |
List of Parasitic Infections and Vectors
| Name of the Disease | Etiological agent (s) | Vector(s) |
|---|---|---|
| African Sleeping Sickness (African trypanosomiasis) | Trypanosoma brucei | Tsetse fly ( Glossina species) |
| Amebiasis | Entamoeba histolytica | |
| American Trypanosomiasis (Chagas Disease) | Trypanosoma cruzi | Various species of triatomine bugs |
| Ascariasis (intestinal roundworm infection) | Ascaris lumbricoides | |
| Babesiosis | Babesia species | Ixodes scapularis ticks |
| Balantidiasis | Balantidium coli | |
| Cryptosporidiosis | Cryptosporidium species | |
| Cyclosporiasis | Cyclospora cayetanensis | |
| Cysticercosis and Neurocysticercosis | Taenia solium | |
| Echinococcosis (Hydatid Disease) | Echinocococcus granulosus | |
| Elephantiasis (Filariasis, Lymphatic Filariasis) | Wuchereria bancrofti | Mosquitoes of the genus, Anopheles, Culex, Aedes and Mansonia |
| Enterobiasis (pinworm infection) | Enterobius vermicularis | |
| Fascioliasis (Fasciola Infection) | Fasciola hepatica (liver fluke) | |
| Giardiasis | Giardia lamblia | |
| Guinea Worm Disease (Dracunculiasis) | Dracunculus medinensis | |
| Hookworm infection | Ancylostoma duodenale, A. ceylanicum, and Necator americanus | |
| Hymenolepiasis | Hymenolepis nana | |
| Kala-azar (Leishmaniasis, Leishmania Infection) | Leishmania donovani | Sand fly ( Phlebotomus papatasi and Phlebotomus argentipes ) |
| Loiasis (Loa loa Infection) | Loa loa | Deerflies (mango flies or mangrove flies) of the genus Chrysops. |
| Malaria | Plasmodium species ( vivax, ovale, malariae and falciparum ) | Infected female Anopheles mosquito |
| Onchocerciasis (River Blindness) | Onchocerca volvulus | Blackflies of the genus Simulium |
| Toxoplasmosis | Toxoplasma gondii | |
| Trichinellosis (Trichinosis) | Trichinella species | |
| Whipworm Infection (Trichuriasis, Trichuris Infection) | Trichuris trichiura |
Prevention of Parasitic Infections
Prevention strategies must match the transmission route. Generic advice ("wash your hands") addresses feco-oral transmission but does nothing for vector-borne or transcutaneous infections.
Prevention by Transmission Route
Feco-oral route (Entamoeba, Giardia, Ascaris, Trichuris, Taenia):
- Safe water: boiling, chlorination, or filtration (removes cysts and eggs)
- Safe food handling: washing vegetables, cooking meat thoroughly (pork to ≥63°C, beef to ≥71°C to kill cysticerci and Toxoplasma cysts)
- Hand hygiene: washing with soap and water after defecation and before food preparation — the single highest-impact behavioural intervention
- Sanitation infrastructure: pit latrines or flush toilets to prevent faecal contamination of soil and water
Skin penetration (hookworm, Strongyloides):
- Wearing footwear — the simplest and most effective single intervention for hookworm prevention
- Avoiding sitting or lying on potentially contaminated soil
- Avoiding contact with untreated water in endemic areas (cercariae of Schistosoma)
Vector-borne (Plasmodium, Leishmania, Wuchereria, Trypanosoma):
- Insecticide-treated bed nets (ITNs) — highly effective for malaria, also reduce leishmaniasis and filariasis
- Residual insecticide spraying (IRS) in dwellings — for malaria and kala-azar vector control
- Repellents (DEET-based) for personal protection
- Protective clothing during peak vector activity hours
- Chemoprophylaxis for travellers to malaria-endemic areas
Vertical (transplacental) transmission (Toxoplasma, Plasmodium, Trypanosoma cruzi):
- Antenatal screening in endemic areas
- Avoiding undercooked meat and cat faeces during pregnancy (Toxoplasma)
- Prompt treatment of maternal malaria in pregnancy
- Congenital screening programmes in Chagas-endemic regions
Blood transfusion transmission (Plasmodium, Leishmania, Trypanosoma, Babesia):
- Donor screening in endemic areas — serological testing for malaria, Chagas disease
- Deferral of blood donation from travellers returning from malaria-endemic areas
- Leukodepletion of blood products reduces but does not eliminate the risk
Autoinfection (Strongyloides, Enterobius, Taenia solium):
- Treat all household members simultaneously for pinworm (not just the index case)
- Mass drug administration (MDA) programmes using albendazole/mebendazole in endemic areas
- Screening and treatment of Strongyloides before immunosuppressive therapy (corticosteroids, anti-TNF agents, transplant)
- Hygiene education to prevent reinfection
Population-Level Prevention
Mass drug administration (MDA): WHO-recommended preventive chemotherapy for soil-transmitted helminths (albendazole or mebendazole), lymphatic filariasis, schistosomiasis, and onchocerciasis. Targets school-age children and other at-risk groups in endemic areas regardless of individual infection status.
One Health approach: Many parasitic infections are zoonotic — controlling animal reservoirs (deworming dogs for Echinococcus, treating cats for Toxoplasma, veterinary surveillance for Taenia) directly reduces human infection risk.
WASH programmes: Water, Sanitation, and Hygiene infrastructure is the most durable long-term prevention for feco-oral parasites. No pharmaceutical intervention has a comparable lasting impact on transmission at the population level.
Where Students Actually Get Confused
1. "Bacteria and fungi are also parasites." In everyday language, "parasite" is used loosely. In medical parasitology, the term is restricted to protozoa, helminths (nematodes, cestodes, trematodes), and ectoparasites (arthropods). Bacteria are studied in bacteriology; fungi in mycology. While all pathogens benefit at the host's expense, only organisms studied in the parasitology curriculum are technically "parasites" in this context.
2. "The feco-oral route transmits all intestinal parasites." Not all. Hookworm and Strongyloides — both intestinal parasites — are not transmitted feco-orally. Their infective stage (filariform larvae) actively penetrates the skin. A patient who drinks clean water but walks barefoot on contaminated soil is still at risk of hookworm but protected against Ascaris and Giardia.
3. "Autoinfection = reinfection." Autoinfection means the same individual re-acquires infection from their own parasite without exposure to an external source. Reinfection requires a new external source. The clinical difference matters: Strongyloides hyperinfection can kill an immunocompromised patient without any new mosquito bite, contaminated food, or contact — purely from internal amplification.
4. "All vector-borne parasites are transmitted by mosquitoes." Mosquitoes transmit Plasmodium, Wuchereria bancrofti, and Brugia spp. But sandflies transmit Leishmania; tsetse flies transmit Trypanosoma brucei; triatomine bugs transmit T. cruzi; blackflies (Simulium) transmit Onchocerca volvulus; deer flies (Chrysops) transmit Loa loa. The vector-disease pairing is a common MCQ format.
5. "Vertical transmission only means mother-to-infant during birth." Vertical (transplacental) transmission occurs across the placenta during pregnancy, not only at birth. Toxoplasma gondii primary infection during pregnancy can cross the placenta at any trimester; Plasmodium can cross in endemic areas; Trypanosoma cruzi (Chagas) causes congenital disease in South America. This is distinct from perinatal transmission (during delivery) or postnatal transmission (via breast milk).
6. "Obligate parasites cannot survive outside a host at all." Obligate parasites cannot complete their life cycle without a host, but some infective stages (eggs, cysts, oocysts) can survive in the environment for extended periods — Ascaris eggs survive in soil for years, Cryptosporidium oocysts resist chlorination. "Obligate" refers to the need for a host to complete development, not to immediate death outside a host.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Most common transmission route | Feco-oral | "Dirty hands, dirty water" |
| Skin-penetrating helminths | Hookworm, Strongyloides | Filariform L3 larvae; no footwear = risk |
| Only helminth with indefinite autoinfection | Strongyloides stercoralis | Hyperinfection in immunocompromised = fatal |
| Autoinfection → neurocysticercosis | Taenia solium eggs ingested (own hands or reverse peristalsis) | Most common cause of acquired epilepsy in LMIC |
| Transplacental parasites | Toxoplasma, Plasmodium, T. cruzi | Screen pregnant women in endemic areas |
| Parasite transmitted by tsetse fly | Trypanosoma brucei | African sleeping sickness |
| Parasite transmitted by triatomine bug | Trypanosoma cruzi | Chagas disease (Latin America) |
| Parasite transmitted by blackfly (Simulium) | Onchocerca volvulus | River blindness |
| Parasite transmitted by deer fly (Chrysops) | Loa loa | Loiasis |
| Schistosoma: infective stage + route | Cercariae; penetrate skin in fresh water | No ingestion needed — swimming/wading enough |
| Diphyllobothrium: source | Freshwater fish (undercooked) | Fish tapeworm; vitamin B12 deficiency |
| Paragonimus: source | Crab or crayfish (undercooked) | Lung fluke |
| Fasciola: source | Aquatic plants (watercress) | Liver fluke |
| WASH impact | Most durable prevention for feco-oral parasites | Water + Sanitation + Hygiene |
| MDA drugs | Albendazole/mebendazole (helminths); ivermectin (filariasis, schistosomiasis) | WHO preventive chemotherapy |
| Facultative parasite examples | Acanthamoeba, Naegleria fowleri | Can live free or parasitic depending on conditions |
| Accidental parasite example | Echinococcus granulosus in humans | Normal host = dog; humans = dead-end host |
| Aberrant parasite example | Toxocara in humans | Cannot complete life cycle in humans |
Self-Check Questions
- A child presents with perianal itching that is worse at night. His mother says the whole family has been affected. Which parasite is responsible, what is the transmission mechanism, and why must the entire household be treated?
- An immunocompromised patient on long-term corticosteroids develops hyperinfection syndrome with gram-negative septicaemia. Which parasite is responsible, and why does immunosuppression make autoinfection dangerous?
- A patient with confirmed intestinal Taenia solium infection is found to have seizures. What complication has occurred and how?
- Name the vector for each: (a) Trypanosoma brucei (b) Trypanosoma cruzi (c) Leishmania donovani (d) Onchocerca volvulus (e) Loa loa
- Which route of transmission does Schistosoma use, and what is the infective stage? Why does wearing footwear not prevent schistosomiasis?
- A woman in the first trimester of pregnancy is diagnosed with primary Toxoplasma gondii infection. How has she most likely acquired this infection, and what is the risk to her fetus?
- Which intestinal helminth does NOT primarily use the feco-oral route? What is its infective stage and actual route of entry?
Answers
1. Enterobius vermicularis (pinworm); external autoinfection — nocturnal perianal egg-laying → scratching → finger-to-mouth; household treatment required because eggs spread on bedding, clothing, and surfaces infecting all members.
2. Strongyloides stercoralis; corticosteroids impair cellular immunity, allowing unchecked internal autoinfection — rhabditiform larvae transform to filariform, penetrate gut wall en masse, carrying enteric bacteria causing fatal sepsis.
3. Neurocysticercosis — the patient ingested T. solium eggs (from their own tapeworm via contaminated hands or reverse peristalsis); eggs hatched and larvae migrated to the brain; the most common cause of acquired epilepsy in LMIC.
4. (a) Tsetse fly (Glossina spp.) (b) Triatomine bugs (reduviid bugs) (c) Sandfly (Phlebotomus spp.) (d) Blackfly (Simulium spp.) (e) Deer fly (Chrysops spp.).
5. Active skin penetration by free-swimming cercariae in freshwater; wearing footwear does not prevent schistosomiasis because cercariae penetrate any exposed wet skin — wading, swimming, or washing.
6. Most likely through eating undercooked meat containing tissue cysts, or contact with cat faeces (changing a litter box); transplacental transmission risk is highest if primary infection occurs in the first trimester — can cause congenital toxoplasmosis (chorioretinitis, intracranial calcifications, hydrocephalus).
7. Hookworm (Ancylostoma/Necator) and Strongyloides — infective stage is filariform (L3) larvae that actively penetrate intact skin when a person walks barefoot on contaminated soil.)
References
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- Sastry, A. S., & Bhat, S. (2014). Essentials of Medical Parasitology. Jaypee Brothers Medical Publishers.
- Bogitsh, B. J., Carter, C. E., & Oeltmann, T. N. (2018). Human Parasitology (5th ed.). Academic Press.
- World Health Organization. (2023). Soil-transmitted helminth infections. WHO Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections
- World Health Organization. (2023). Preventive chemotherapy to control soil-transmitted helminth infections in at-risk population groups. WHO Guidelines. https://www.who.int/publications/i/item/9789240031234
- Pam, D. D., Ogefere, H. O., & Agba, M. I. (2023). Quantitative Buffy Coat (QBC) test and other diagnostic techniques for diagnosing malaria: review of literature. Asian Journal of Medical Sciences, 14(4), 1–8.
- El-Beshbishi, S. N., Ahmed, N. N., Mostafa, S. H., & El-Ganainy, G. A. (2012). Parasitic infections and myositis. Parasitology Research, 110(1), 1–18. https://doi.org/10.1007/s00436-011-2609-8
Frequently Asked Questions
What is the most common mode of transmission of parasitic infections?
Which parasites can be transmitted through blood transfusion?
What is autoinfection in parasitology and which parasites cause it?
Which parasites can be transmitted from mother to fetus?
What is the difference between an obligate and a facultative parasite?
How does Strongyloides stercoralis cause hyperinfection in immunocompromised patients?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.