Bacteroides fragilis: Properties, Pathogenesis, Lab Diagnosis
Bacteroides fragilis: Properties, Pathogenesis, Lab Diagnosis
General Characteristics
- Gram-negative, non-spore-forming, non-motile, pleomorphic bacilli; appearing as slender rods or coccobacillus forms.
- Obligate anaerobe
- It is also probably the most frequent anaerobe isolated from clinical specimens.
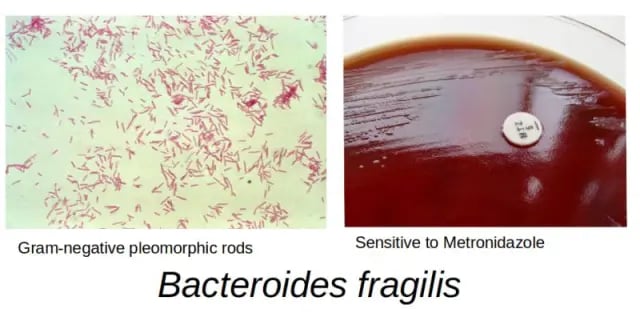 Figure: Bacteroides fragilis
Figure: Bacteroides fragilis
Habitat
It is the most common commensal in the human intestine. Members of the Bacteroides fragilis group make up a significant proportion of the normal microbiota of the GI tract (10^11 to 10^12 CFU/g feces).
Virulence Factors
Members of the Bacteroides fragilis group are responsible for a variety of clinical infections, but the species B. fragilis has the highest incidence. A number of virulence factors have been demonstrated to explain the enhanced virulence and pathogenicity of this particular species:
- agglutinins and fimbriae provide adhesion ability;
- the capsule protects against the host immune response by evading phagocytosis;
- mechanisms to ameliorate oxygen toxicity; and,
- destruction of host tissue via production of histiocytic enzymes.
Disease
B. fragilis causes peritonitis following bowel injury and pelvic inflammatory disease (PID). It is also implicated in abdominal infections, brain abscesses, and empyema (pyothorax or purulent pleuritis). Enterotoxigenic strains can cause diarrhea.
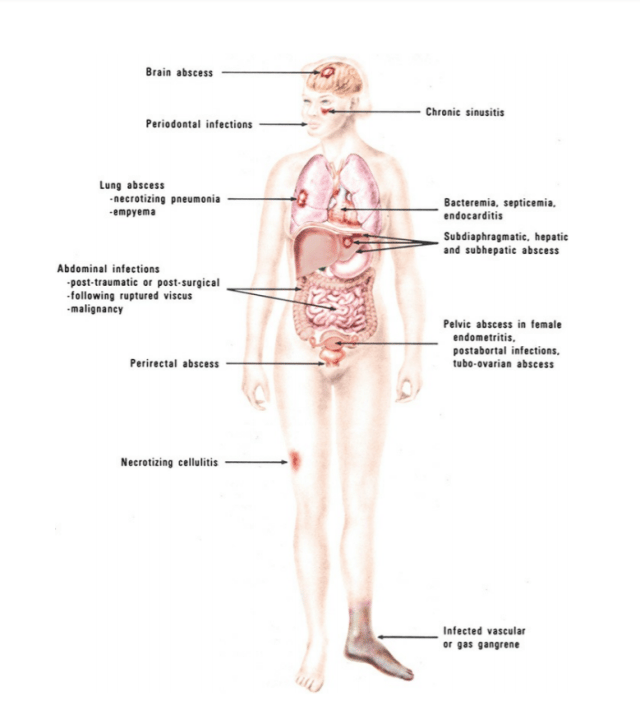 Figure: Common locations of infections involving anaerobic bacteria(Image source: Koneman, Ref-1)
Figure: Common locations of infections involving anaerobic bacteria(Image source: Koneman, Ref-1)
As members of the B. fragilis group constitute a significant proportion of the microbiota of the GI tract; breaks in the GI mucosa by trauma or GI or GU surgery allows entry of these bacteria and consequent intra-abdominal infections, if appropriate prophylaxis is not commenced. B.fragilis is most commonly responsible for intra-abdominal abscesses and sepsis but is also involved in gynecological abscesses, skin and soft tissue infections, pericarditis (as a result of hematogenous spread to the heart), bacteremia often associated with malignancies or in postsurgical infections, and rare instances of endocarditis, meningitis, and septic arthritis.
Laboratory Diagnosis
All clinical specimens must be handled meticulously as brief exposure to oxygen may kill obligate anaerobes and result in failure to isolate them in the laboratory.
Accepted specimens
- Tissue bits
- Necrotic materials
- Aspirated body fluids
- Pus in syringes
Unacceptable specimen for anaerobic culture
- gastric washings,
- all swabs
- midstream urine,
- prostatic secretions collected transurethrally,
- feces (except for the recovery of Clostridioides difficile),
- throat, nose, or other oropharyngeal specimens (except specimens obtained from the deep tissue during oral surgery),
- superficial skin, and environmental cultures
Transport
Specimens should be immediately put into RCM broth or other anaerobic transport media and brought to the laboratory as soon as possible.
Gram Stain
All clinical specimens from suspected anaerobic infections should be Gram stained and examined for characteristic morphology.
 Figure: Gram-negative, Bacteroides fragilis subsp.fragilis(Image source: CDC/ Don Stalons)
Figure: Gram-negative, Bacteroides fragilis subsp.fragilis(Image source: CDC/ Don Stalons)
Many times in clinical laboratories, anaerobic gram-negative bacilli that grow on Bacteroides fragilis selective media (like Bacteroides bile esculin) may be reported out as “B. fragilis group”; so it is difficult to know how common some of the other members are in infections. With the increased use of molecular methods and MALDI-TOF in the future, we should expect to be able to better determine what species really are involved in clinical infections.
Culture & Identification
Samples should be processed immediately under anaerobic conditions which can be created by various methods. Anaerobic cultures should be performed routinely only on tissues or aspirated fluid/pus.
Never perform anaerobic cultures on specimens from sites that may be contaminated with mucosal flora or feces
Various culture media can be used for the isolation of anaerobes, such as:
- Anaerobic blood agar
- Neomycin blood agar
- Egg yolk agar
- Phenlethyl agar (PEA)
- BHIS agar: Brain-Heart infusion agar added with supplements, such as vitamin K and hemin
- Bacterioides bile esculin agar (BBE agar)
Isolates are identified on the basis of
- Colony morphology,
- Gram staining characteristics
- Biochemical tests
- Susceptibility to antibiotic disks
- Gas-liquid chromatography etc.
Antimicrobial Susceptibility
B. fragilis group isolates produce β-lactamases and consequently are resistant to penicillin (ampicillin, amoxicillin) and most cephalosporins, but are usually susceptible to ampicillin-sulbactam and piperacillin-tazobactam. They are uniformly susceptible to metronidazole and carbapenems, but increasingly resistant to clindamycin.
References and Further Readings
- Procop, G. W., & Koneman, E. W. (2016). Koneman’s Color Atlas and Textbook of Diagnostic Microbiology(Seventh, International edition). Lippincott Williams and Wilkins.
- Tille, P. (2017). Bailey & Scott’s Diagnostic Microbiology (14 edition). Mosby.

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.