Varicella-Zoster Virus: How One Virus Causes Two Diseases Decades Apart
How VZV hides in dorsal root ganglia after chickenpox, what triggers reactivation as shingles, and why aspirin is dangerous in children with VZV.
A six-year-old gets chickenpox, recovers completely in two weeks, and is left with lifelong immunity. Sixty years later, the same person develops a burning pain on one side of their chest, followed three days later by a band of blisters in a dermatomal distribution. It's shingles, caused by the exact same virus that infected them in childhood, which has been hiding undetected in their dorsal root ganglia for six decades.
This is one of the most elegant demonstrations of viral latency in human medicine. VZV doesn't do what most viruses do after acute infection; get cleared entirely or cause chronic active disease. Instead, it retreats into sensory neurons, where it exists as a transcriptionally silent provirus, held in check by the host's VZV-specific T-cell immunity for years, sometimes decades. When that T-cell surveillance wanes; as it does naturally with age, or more acutely with immunosuppression — the virus reactivates, travels back down the axon to the skin, and causes disease again in the dermatome served by the ganglion where it has been hiding.
Understanding this latency-and-reactivation cycle is what makes VZV clinically coherent: it explains why shingles occurs specifically in older and immunocompromised patients, why the rash is unilateral and dermatomal (one ganglion reactivating at a time), why postherpetic neuralgia can persist for months after the rash resolves, and why a vaccine exists specifically for older adults to boost their waning VZV T-cell immunity before the virus gets a chance to reactivate.
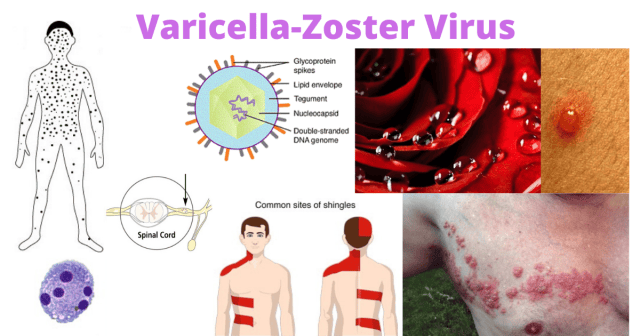 Figure: Varicella-Zoster Virus (VZV)
Figure: Varicella-Zoster Virus (VZV)
Varicella is less contagious than measles, but more contagious than mumps and rubella.
Characteristic Features of VZV
- Double-stranded (ds) DNA virus.
- Member of the herpesvirus (human α-herpesvirus family).
- Single serotype (one attack of chickenpox gives lifelong immunity).
- Humans are the only known reservoir hosts.
Chickenpox
Transmission
Mode of transmission of chickenpox is direct contact with skin lesions, inhalation of aerosols from vesicular fluid of skin lesions of acute varicella or zoster, or aerosols of infected respiratory secretions. Person is contagious 1-2 days before the appearance of the rash until all blisters are crusted.
Pathogenesis
Varicella-zoster virus enters through the upper respiratory mucosa or the conjunctiva. VZV infects macrophages and pneumocytes in the respiratory mucosa. Virus spreads to the reticuloendothelial system, replicates in the regional lymph nodes, and enters the bloodstream (primary viremia). From the hematogenous route, it reaches the liver, and spleen and multiplies there. Secondary viremia occurs, and the VZV present in the infected mononuclear cells are transported to skin, respiratory tract, and neurons.
- Skin: Virus replication in the epithelial cells leads to the development of typical rashes. Swelling of epithelial cells, ballooning degeneration, and accumulation of tissue fluids result in the formation of vesicles.
- Respiratory tract: VZV is shed in the respiratory secretions of the infected individuals leading to the transmission of infection to other individuals.
- Neurons: VZV gains access to neurons and undergoes latency in dorsal root ganglia.
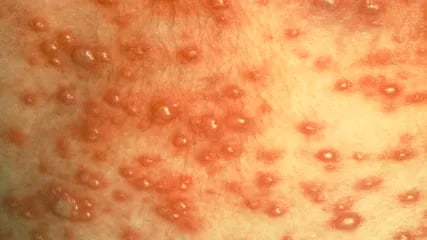 Figure: Vesicular rashes in chickenpox (Image source: CDC/PHIL)Three types of lesions are most often seen in varicella-zoster infections;maculopapular lesions (lesions with a raised red bump), vesicular lesions (blister-like or fluid-filled lesions), and scabbed or crusted lesions.
Figure: Vesicular rashes in chickenpox (Image source: CDC/PHIL)Three types of lesions are most often seen in varicella-zoster infections;maculopapular lesions (lesions with a raised red bump), vesicular lesions (blister-like or fluid-filled lesions), and scabbed or crusted lesions.
Clinical Manifestations
The incubation period of varicella is 10-21 days.
- Characteristics vesicular rash *(chickenpox vesicle surrounded by an erythematous halo is described as a dewdrop on a rose petal)*appears in about 10-23 days of VZV infections.
- Rashes are centripetal in distribution; the greatest concentration of lesions are seen on the trunk and the fewest lesions on distal extremities.
- Bilateral and diffuse in distribution.
- Rashes appear in multiple crops; lesions in various stages of evolution, such as maculopapular, vesicles, and scabs can be found in one area at the same time.
- Fever appears with each crop of rashes.
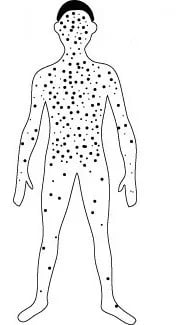 Figure: Distribution of chickenpox rashes
Figure: Distribution of chickenpox rashes
Chickenpox is a disease of childhood. If occurs in adults, it is more severe with bullous and hemorrhagic rashes.
If a pregnant mother develops primary VZV infection, the fetus may be affected. Congenital varicella syndrome is most serious when maternal infection occurs between weeks 8 and 20 of gestation, and can cause limb hypoplasia, cutaneous scarring in a dermatomal distribution, eye abnormalities (microphthalmia, chorioretinitis), and neurological damage (brain atrophy, intellectual disability). Infection near term (within 5 days before to 2 days after delivery) can cause severe neonatal varicella, as the infant is born before maternal antibodies have transferred and has no immune defence against the virus.
Complications
Complications are more common in adults and in immunocompromised individuals. Secondary bacterial infection of the skin is the most common complication. Other complications include pneumonia, CNS involvement (cerebellar ataxia, encephalitis, and aseptic meningitis), myocarditis, nephritis, corneal lesions, and arthritis.
Reye's syndrome is a rare but life-threatening complication involving acute hepatic failure and encephalopathy, associated with aspirin use in children during viral illnesses including chickenpox. Aspirin must never be given to children with chickenpox (or any viral illness). Paracetamol or ibuprofen are used for fever management instead.
Shingles
Zoster or shingles is the recurrent form of varicella-zoster virus infection, which usually occurs later in life when the virus gets reactivated under stress or with immune suppression.
 Figure: Shingles rash (Image source: CDC/PHIL)
Figure: Shingles rash (Image source: CDC/PHIL)
- Chicken pox-like lesions occur in restricted areas (dermatome) that are innervated by a single ganglion;
- The vesicles appear in a dermatomal distribution, almost always unilaterally
- Skin lesions: Usually in the thorax.
- Shingles of an intercostal nerve produces vesicular eruptions and burning pain in the affected dermatome
- Postherpetic neuralgia (PHN): Persistent burning, aching, or shooting pain in the affected dermatome lasting weeks to months after the rash has resolved. PHN is caused by virus-induced damage to sensory neurons and ganglion cells during reactivation, leading to persistent sensitisation of peripheral and central pain pathways. It occurs in approximately 10–18% of shingles patients and is significantly more common in those aged over 60. Early antiviral treatment (within 72 hours of rash onset) reduces but does not eliminate the risk of PHN.
- Maculopapular with an erythematous base, and usually heal in about two weeks.
- Zoster ophthalmicus: Reactivation involving the ophthalmic branch (V1) of the trigeminal nerve can affect the eye, causing keratitis, uveitis, and potentially vision loss. Vesicles on the tip of the nose (Hutchinson's sign) indicate involvement of the nasociliary branch of V1 and signal risk of ocular complications; ophthalmology referral and urgent antiviral therapy are indicated.
- Ramsay Hunt syndrome: Reactivation at the geniculate ganglion of the facial nerve (CN VII) causes a clinical triad of ear pain, vesicles in the external auditory meatus (or on the pinna), and peripheral facial nerve palsy. Hearing loss and vertigo may occur due to proximity of CN VIII, but the primary lesion is in the CN VII ganglion, not CN VIII itself.
- In immunocompromised life-threatening disseminated pneumonia may occur
Diagnosis
The characteristic appearance of lesions both in primary varicella and zoster allows for a presumptive clinical diagnosis. Definitive diagnosis in the laboratory can be achieved by using samples from lesions or blood and testing by the following methods;
Virus culture: Virus can be isolated from the lesions using cell lines. VZV produces HSV-like cytopathic effects such as diffuse rounding and ballooning of infected cells. Virus-specific antigens can be detected in the culture fluids.
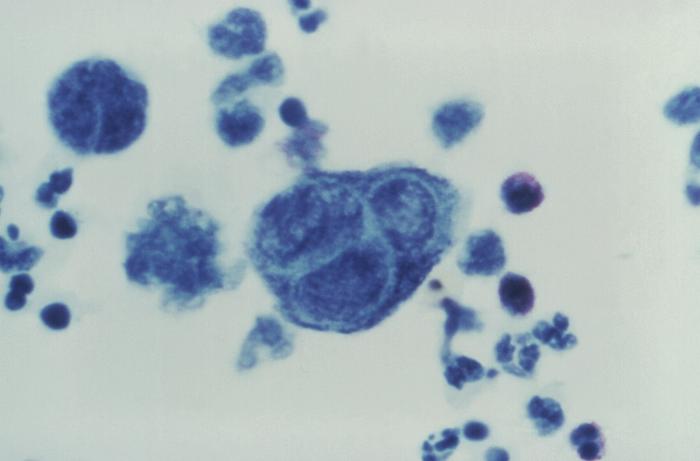 Figure: Tzanck test: Note the presence of a multinucleated giant cell (Tzanck cell) in the center. (Image source: CDC PHIL)
Figure: Tzanck test: Note the presence of a multinucleated giant cell (Tzanck cell) in the center. (Image source: CDC PHIL)
Cytopathology: Giemsa staining of scrapings from the ulcer base (Tzanck smear) reveals cytopathological changes similar to HSV infections, such as the formation of multinucleated giant cells.
Antigen detection
Specific viral antigens can be detected using direct immunofluorescence staining.
Serology
Primary VZV infection elicits immunoglobulin G (IgG), IgM, and IgA antibodies. Raise antibody titer can be detected using various serological methods. It is useful to diagnose varicella but less useful in the case of zoster.
Molecular Methods
Polymerase chain reactions (PCR) can be used to detect VZV-specific genes. The presence of the virus DNA can be demonstrated in tissues, vesicular fluid, maculopapular lesions, or crusts from lesions.
Treatment
Chickenpox (Varicella)
In healthy children, chickenpox is generally self-limiting and treatment is supportive — antipyretics, antipruritic agents (e.g. calamine lotion), and good skin hygiene to prevent secondary bacterial infection. Aspirin must never be given to children with chickenpox or any other viral illness, due to the risk of Reye's syndrome (see the "Where Students Get Confused" section below for the full mechanism).
Antiviral treatment with acyclovir (an inhibitor of viral DNA polymerase) is indicated when:
- Adolescents and adults with chickenpox (at higher risk of severe disease and pneumonia)
- Immunocompromised patients of any age
- Neonates with perinatal VZV exposure
- Pregnant women (particularly in the second and third trimesters)
- Patients with severe or complicated disease
Shingles (Herpes Zoster)
Antiviral therapy with valacyclovir or famciclovir (preferred over oral acyclovir for shingles due to better bioavailability and simpler dosing) should be started within 72 hours of rash onset to reduce viral shedding, shorten the duration of illness, and — most importantly — reduce the incidence and severity of postherpetic neuralgia. Antivirals started after 72 hours have limited benefit unless new lesions are still forming. Pain management is a central part of shingles care, particularly in older adults where postherpetic neuralgia can persist for months.
Prevention and Vaccination
Varicella vaccine (for children) A live attenuated vaccine based on the Oka strain of VZV. Two doses are recommended in most national immunization programs: the first at 12–15 months and the second at 4–6 years. Vaccination has dramatically reduced childhood chickenpox hospitalizations and deaths in countries where it is widely used.
Zoster vaccine (for older adults) The recombinant subunit zoster vaccine (Shingrix) is recommended for adults aged 50 and older in high-income settings. Unlike older live attenuated zoster vaccines, Shingrix contains VZV glycoprotein E (the major target antigen) plus an adjuvant system, and is more than 90% effective at preventing shingles and postherpetic neuralgia in older adults. The mechanism is straightforward: it boosts waning VZV-specific T-cell immunity before it falls low enough for reactivation to occur.
Post-exposure prophylaxis Varicella-zoster immunoglobulin (VZIG) is available for post-exposure prophylaxis in high-risk non-immune individuals — including immunocompromised patients, pregnant women, and neonates born to mothers with active varicella — given within 96 hours of exposure.
How to Remember
Primary vs. reactivation disease in one image: the same virus, two completely different patterns. Chickenpox is centripetal (trunk more than extremities), bilateral, multiple crops in various stages simultaneously, and appears all over the body because viremia seeds the skin widely. Shingles is unilateral, dermatomal, and follows one nerve's territory exactly — because the virus isn't spreading through the blood this time, it's traveling back down one specific axon from one specific ganglion. The distribution difference directly maps onto the biological difference between hematogenous spread (primary) and axonal transport (reactivation).
The "dewdrop on a rose petal" is the single most memorable chickenpox finding. A small, clear, fluid-filled vesicle on an erythematous base — if you can picture a dewdrop on a red petal, you can picture a chickenpox lesion. This description is so specific that recognising it immediately suggests VZV in a clinical or exam context.
"Crops" means different stages simultaneously — the most characteristic chickenpox finding. Unlike many viral rashes that progress uniformly, chickenpox appears in multiple crops over several days, so at any one time you can see maculopapules, vesicles, and crusted lesions all on the same skin area. This simultaneous multi-stage presentation is not seen in smallpox (all lesions the same stage simultaneously) — the distinction was historically important for differentiating the two diseases.
Latency is held in check by T-cells, not antibodies. This is worth anchoring explicitly because it's the opposite of what drives vaccine-preventable antibody-mediated diseases. VZV antibodies don't prevent reactivation; it's the cell-mediated immune response that keeps the latent virus suppressed. This is why immunocompromised states that primarily affect T-cell function (HIV, post-transplant immunosuppression, corticosteroid therapy) dramatically increase shingles risk, even in individuals with plenty of circulating anti-VZV antibodies.
Hutchinson's sign: vesicles on the nose tip = eye in danger. When shingles involves the ophthalmic branch of the trigeminal nerve (zoster ophthalmicus), involvement of the nasociliary branch — which supplies both the tip of the nose and the eye — signals risk of corneal and ocular involvement. Vesicles on the tip of the nose are Hutchinson's sign, an urgent flag to involve ophthalmology and start systemic antivirals. The mnemonic is simple: "nose tip, eye tip" — if the tip of the nose is involved, the eye may follow.
Key Exam Facts Table
| Feature | Detail |
|---|---|
| Family / Genus | Herpesviridae / Varicellovirus (α-herpesvirus) |
| Genome | dsDNA, ~125 kb |
| Envelope | Present |
| Serotypes | One only; lifelong immunity after infection |
| Reservoir | Humans only |
| Primary infection | Varicella (chickenpox) — generalised, bilateral, centripetal rash in multiple crops |
| Latency site | Dorsal root ganglia (all levels of neuroaxis); trigeminal ganglia |
| Latency mechanism | Transcriptionally silent in sensory neurons; held in check by VZV-specific T-cell immunity |
| Reactivation trigger | Waning cell-mediated immunity (age, immunosuppression, stress) |
| Reactivation disease | Herpes zoster (shingles) — unilateral, dermatomal, follows axonal route |
| Classic chickenpox lesion | "Dewdrop on a rose petal" — clear vesicle on erythematous base |
| Classic chickenpox feature | Multiple crops; all lesion stages simultaneously |
| Contagious period (chickenpox) | 1–2 days before rash until all lesions crusted |
| Contagious period (shingles) | While vesicles are present (lower transmission risk than chickenpox) |
| Tzanck smear finding | Multinucleated giant cells (Tzanck cells) — also seen in HSV, not specific to VZV |
| Zoster ophthalmicus | Ophthalmic branch V1; vesicles on nose tip = Hutchinson's sign = risk of corneal involvement |
| Ramsay Hunt syndrome | Geniculate ganglion of CN VII; ear pain + facial palsy + auricular vesicles |
| Postherpetic neuralgia | Persistent burning pain after rash resolves; due to nerve damage from viral replication in ganglion |
| Aspirin contraindication | Absolute in children with VZV (and any viral illness) — Reye's syndrome risk |
| Treatment (chickenpox) | Supportive in healthy children; acyclovir for adults, immunocompromised, neonates |
| Treatment (shingles) | Valacyclovir or famciclovir within 72 hours of rash onset |
| Varicella vaccine | Live attenuated Oka strain; 2 doses (12–15 months, 4–6 years) |
| Zoster vaccine | Recombinant subunit (Shingrix); recommended ≥50 years; >90% effective |
Where Students Get Confused
"Aspirin is fine to give to a feverish child with chickenpox." It is not — this is one of the most clinically dangerous misconceptions a student can carry into practice. Aspirin given to children with viral illnesses (particularly VZV and influenza) is associated with Reye's syndrome: a rare but life-threatening condition causing acute hepatic failure and encephalopathy, with a mortality rate historically around 20–40%. The mechanism involves mitochondrial dysfunction triggered by the combination of salicylates and viral illness. Paracetamol (acetaminophen) or ibuprofen are used instead. This contraindication extends to all children under 16 with any viral illness, not just chickenpox.
"VZV antibodies prevent shingles." They don't. Antibody titers against VZV remain high for life in previously infected individuals, but shingles still develops because its prevention depends on cell-mediated immunity, specifically VZV-specific T-cell surveillance in dorsal root ganglia. The waning of T-cell immunity with age is why shingles incidence increases sharply after age 50, despite stable antibody levels. The zoster vaccine (Shingrix) works by boosting T-cell immunity, not antibody titers.
"Shingles can spread to contacts and cause shingles." Not directly. A person with active shingles can transmit VZV to a non-immune contact via direct contact with vesicular fluid, but the contact would develop chickenpox (primary VZV infection), not shingles. Shingles is always the result of reactivation of a person's own latent virus, not a new infection from someone else.
"The Tzanck smear differentiates VZV from HSV." It does not. Both VZV and HSV produce multinucleated giant cells (Tzanck cells) on Giemsa-stained smears. The Tzanck smear confirms a herpesvirus infection but cannot distinguish which one. PCR or direct immunofluorescence with virus-specific antibodies is required to differentiate VZV from HSV definitively.
"Shingles only occurs in very elderly patients." In immunocompetent individuals, shingles incidence does increase sharply with age (reflecting waning T-cell immunity). However, shingles can occur at any age in immunocompromised patients — people with HIV, patients on prolonged corticosteroid therapy, chemotherapy recipients, and organ transplant recipients are all at significantly elevated risk regardless of age.
References and further readings
- Gershon, A. A., Breuer, J., Cohen, J. I., Cohrs, R. J., Gershon, M. D., Gilden, D., Grose, C., Hambleton, S., Kennedy, P. G., Oxman, M. N., Rall, G., & Silverstein, S. J. (2015). Varicella zoster virus infection. Nature Reviews Disease Primers, 1, 15016. https://doi.org/10.1038/nrdp.2015.16
- Laing, K. J., Ouwendijk, W. J. D., Koelle, D. M., & Verjans, G. M. G. M. (2018). Immunobiology of varicella-zoster virus infection. Journal of Infectious Diseases, 218(Suppl 2), S68–S74. https://doi.org/10.1093/infdis/jiy403
- De Paschale, M., & Clerici, P. (2016). Microbiology laboratory and the management of mother-child varicella-zoster virus infection. World Journal of Virology, 5(3), 97–124. https://doi.org/10.5501/wjv.v5.i3.97
- Nair, P. A., & Patel, B. C. (2023). Herpes zoster. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK441824/
Frequently Asked Questions
Why does shingles only affect one side of the body in a band-like pattern?
Why is aspirin dangerous in children with chickenpox?
Can a person get shingles from contact with someone who has chickenpox or shingles?
Why doesn't the VZV vaccine prevent shingles the way it prevents chickenpox?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.