Glass Pipettes: Types, Handling, and Uses
Glass pipettes transfer mL-scale volumes in microbiology labs. Learn the types (Mohr's, serological, volumetric, Pasteur), how to read the meniscus correctly, and the drain-out vs. blow-out distinction students most often confuse.
In a microbiology practical, a student is performing a tube agglutination test. She needs to transfer exactly 1 mL of patient serum to each tube in a serial dilution series. She picks up a serological pipette, fills it to the 1 mL graduation mark, and dispenses — then moves through the dilution series. At the end, the results are inconsistent: the agglutination pattern doesn't follow the expected gradient. The problem surfaces during review. She had been using a serological pipette correctly — blowing out the last drop — but she had read the meniscus from the top of the curve rather than the bottom. Each "1 mL" delivery was actually 1.05–1.1 mL. Across eight tubes, the dilution factor drifted. The test had to be repeated.
Glass pipette technique comes down to two things that seem minor until they aren't: knowing which type of pipette you are holding (drain-out or blow-out), and reading the meniscus from the correct reference point. Both errors are invisible at the time they happen and only appear in the results.
Pipettes are the calibrated laboratory equipment used to handle liquids. Many kinds of pipettes are used in the laboratory, like micropipette, glass pipette, automated pipette, etc.
Among those, glass pipettes are one of the liquid handling instruments carrying utmost significance due to their precision. These are useful in handling samples with volume in milliliter (ml).
Glass pipettes are of different types, and handling of glass pipettes requires an attached filler (pipette bulb or pipette filler) at the top for filling the liquids. They have uses in various sectors like chemical laboratories, biochemistry laboratories, forensic science, microbiology laboratories, etc.
Why Glass Pipettes Matter in Microbiology
The micropipette has replaced glass pipettes for most microliter-scale work. But glass pipettes remain the instrument of choice whenever volumes in the milliliter range need to be transferred — and in microbiology, this is more common than students expect.
Preparing liquid culture media requires transferring 5 mL, 10 mL, or 25 mL volumes of reagents and supplements with accuracy. Serological tests — tube agglutination, Widal test, VDRL, complement fixation — require serial dilutions in mL volumes where a volumetric pipette delivers the precision needed. Blood culture bottles are inoculated with defined volumes of blood (8–10 mL for adult bottles). Antimicrobial stock solutions are prepared in mL volumes before being diluted to µL-scale working concentrations.
In each of these contexts, choosing the wrong glass pipette type — or using the right type incorrectly — introduces a volume error that propagates through every subsequent step.
Types of Glass Pipettes
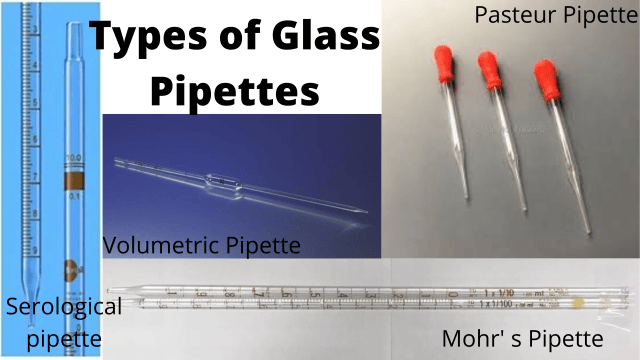 Figure: Types of glass pipette
Figure: Types of glass pipette
The glass pipettes generally used have three types;graduated,non-graduated, and Pasteur pipettes.
Graduated pipettes
Graduated glass pipettes are the type of pipettes that has increments marked along the straight glass tube. Its another name is measuring pipette. It is further classified into two types based on the graduation mark and nominal volume it can pipet;Mohr’s and serological pipette.
- Mohr’s pipette: A Mohr’s pipette is used as a drain-out pipette. It is a straight tube having a graduation mark at each 0.1 ml interval. The first graduation mark begins well past the bottom of the tip. The broken tip can disrupt the precision of handling the liquid.
- Serological pipette: A serological pipette is used as a blow-out pipette. It is a straight tube with a graduation mark near the tip. A slight pressing of the bulb is necessary at the end of dispensation for accuracy.
Mohr's vs. Serological Pipette: The Distinction That Matters Most
These two pipettes look almost identical. The difference is in how the last drop is handled — and confusing them introduces a consistent delivery error.
| Feature | Mohr's Pipette | Serological Pipette |
|---|---|---|
| Delivery type | Drain-out | Blow-out |
| Graduation mark position | Stops above the tip — last section ungraduated | Extends to the tip |
| Last drop | Left in the tip — do NOT blow out | Must be blown out to deliver full volume |
| Identification | No graduation near tip | Blow-out ring at top (near suction end); graduation near tip |
| Risk of confusion | Blowing out a Mohr's over-delivers; not blowing out a serological under-delivers | Same — opposite error |
| Best used for | Partial volume delivery from a measured range | Full nominal volume delivery |
The practical rule: Before using any graduated glass pipette, check the tip. If the graduation marks stop before the tip, it is a Mohr's — do not blow out. If the marks extend to the tip and there is a ring near the top, it is serological — blow out completely.
Likewise, based on construction, pipettes are of three types; type 1, type 2, and type 3.
- Type 1: These have nominal values at the bottom and can deliver liquid samples partially only for all the values.
- Type 2: These have nominal values at the top of the pipette and the highest value below.
- Type 3: These are like type 1 in construction, but they can deliver fluids completely only in nominal value.
Similarly, based on the accuracy, the graduated pipettes are of **class A, class As, and class B. Class A and As are very accurate because they have specified error ranges. In contrast, class B is less accurate because it has double the general error limits.
Non-graduated pipettes
Non-graduated pipettes are the pipettes that lack the increment of graduation mark in the tube. The other denotation of a non-graduated pipette can also be a volumetric pipette, a bulb pipette, or a transfer pipette.
Pasteur pipettes
Pasteur pipettes are called an eye dropper or a dropper. Its construction is either with glass or plastic material. The tip end tapers to a narrow opening in the Pasteur pipette. There is a bulb at the top of the pipette in the case of plastic and glass Pasteur pipette needs a rubber bulb for withdrawing liquid. A teat pipette is the combination of a glass pipette and a rubber bulb.
Parts of Glass Pipettes
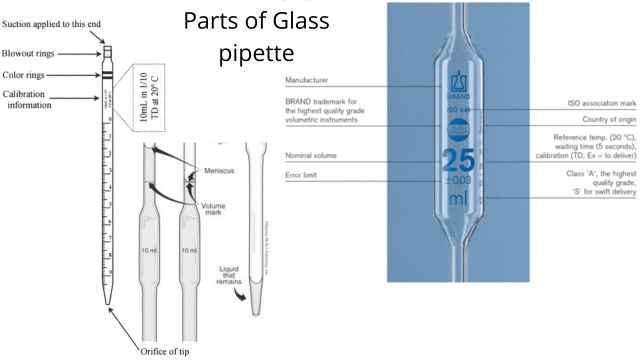 Figure: Parts of glass pipette
Figure: Parts of glass pipette
The parts of glass pipettes are as follows:
- Orifice of the tip: It is the pointed end of the pipette and comes in direct contact with the liquid.
- Calibration details: It is an area in the pipette above the graduation mark. It has the imprinted details about the manufacturer, volume range (measuring) or nominal volume (bulb pipette), tolerance volume, calibration temperature, standard applied for calibration, and waiting time.
- Color rings: Color rings or color bands is a code to identify the nominal volume of the pipette by some companies.
- Suction end: It is the top part of the pipette, where the pipette filler or bulb can attach for aspirating and dispensing the liquids.
- Additional parts: The bulb pipette has a volume mark for pipetting or transferring the correct amount of liquid volume. The blow-out or serological pipette has a blow-out ringnear the topmost or suction part of the pipette.
Handling of Glass Pipettes
While handling glass pipettes, one should never aspirate fluids in the laboratory from the mouth. A pipette bulb, rubber bulb, or filler is used for aspirating.
Reading the Meniscus
The meniscus is the curved surface of liquid at the graduation mark. Reading it incorrectly produces a consistent volume error on every pipetting step.
For colourless and light-coloured liquids (water, saline, most reagents): Read from the bottom of the meniscus curve — the lowest point of the concave surface — with the eye level with the graduation mark. Reading from the top of the meniscus over-reads the volume.
For coloured or opaque liquids (iodine, some dye solutions, mercury): These form a convex meniscus. Read from the top of the curve.
Parallax error: If the eye is above or below the level of the graduation mark when reading, the mark appears to intersect the meniscus at the wrong point. Always position the eye exactly level with the graduation mark — not above, not below.
A simple habit eliminates both errors: before every pipetting step, lower your head until your eye is level with the graduation mark, then read. This takes two seconds and prevents the most common volume error in glass pipette technique.
Pipette Bulb
 Figure: Pipette filler or pipette bulbImage source: Paweena.S, CC BY-SA 4.0https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons
Figure: Pipette filler or pipette bulbImage source: Paweena.S, CC BY-SA 4.0https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons
A pipette bulb is made up of rubber, so it is also called a rubber bulb. It is used to safely fill the pipette with liquid in the laboratory, hence named pipette filler. The generally used pipette filler are general purpose bulbs, three-valve bulbs, and thumb wheel type fillers (made of plastic).
Steps for using three valve pipette bulb:
Filling the Liquid
- Fill the pipette with pipette filler approximately above 5 mm of the mark.
- Then, adjust and bring the liquid to the graduated mark.
- Set the meniscus at the mark (for colorless liquid, the upper meniscus, and the colorful fluid lower meniscus).
- Remove excess liquid from the tip for precise delivery.
Dispensing the Liquid
- Place the tip of the pipette into the container.
- Press the filler to dispense all the liquid.
- Wait for a few seconds when the liquid reaches the tip (based on the company’s guidelines).
- After the wait time, draw the pipette upwards by touching the wall to dispense the remaining liquid. Do not blow out the remaining liquid.
Common Errors in Glass Pipette Use
| Error | Consequence | Prevention |
|---|---|---|
| Blowing out a Mohr's pipette | Over-delivery — the ungraduated tip section adds volume beyond the set amount | Check for blow-out ring; if absent, it is a Mohr's — drain only |
| Not blowing out a serological pipette | Under-delivery — the last drop (which is part of the nominal volume) remains in the tip | Confirm blow-out ring is present; give a final press of the bulb after dispensing |
| Reading meniscus from the top (colourless liquid) | Consistent over-reading — each volume is larger than intended | Read from the bottom of the meniscus, eye level with the mark |
| Parallax error | Volume appears correct but is actually over or under | Eye must be exactly level with the graduation mark, not above or below |
| Mouth pipetting | Ingestion or inhalation of hazardous liquids; biological hazard | Always use a pipette bulb, filler, or mechanical pipetting aid — no exceptions |
| Filling above the mark then over-draining | Imprecise final volume | Fill approximately 5 mm above the mark, then adjust down slowly to the graduation mark |
| Broken tip on Mohr's pipette | Volume delivery is undefined — the ungraduated section is now missing | Discard immediately; a broken-tip Mohr's pipette cannot be used accurately |
| Touching pipette tip to container wall during Mohr's drainage | Drainage stops prematurely; tip contact creates surface tension that holds liquid back | Drain freely into the container; touch the wall only at the end to remove the hanging drop |
Uses of Glass Pipettes
The glass pipette has broad utility in almost all science laboratories. Some fields with the use of glass pipettes are as follows:
- Chemistry laboratory: It is used in transferring liquids during various processes. The volumetric pipette is helpful in different tests relating to volumetric analysis.
- Pharmaceutical industry: Glass pipettes in the pharmaceutical industry have utility in drug production. It is used to transfer measured volume in during quality control as well.
- Microbiology laboratory: Like droppers, glass pipettes transfer different chemicals in milliliter (ml) in various experiments.
- Biochemistry laboratory: The primary uses of glass pipettes in the biochemistry laboratory are as follows:
- For preparing buffer solution.
- To transfer the solution for conducting different biochemical tests.
- For accurate measurements of the chemicals.
For a comparison of all pipette types used in the microbiology laboratory, see Types of Pipettes in the Microbiology Laboratory
How to Remember
Mohr's drains; serological blows — the easiest distinction in pipetting. Mohr's = drain out (like a drain pipe — liquid flows and stops). Serological = blow out (like blowing the last drop out of a straw). If you remember nothing else about glass pipettes, remember this one distinction — it prevents the most common delivery error.
The meniscus rule: "Colourless = bottom; coloured = top." For transparent liquids, read the bottom of the curve. For opaque or coloured liquids, read the top. And always — always — get your eye level with the mark before reading.
Glass pipettes think in mL; micropipettes think in µL. If your volume has a decimal point and the unit is µL, you need a micropipette. If your volume is a whole number in mL (1 mL, 5 mL, 10 mL), glass pipettes are the right instrument. Crossing this boundary — using a glass pipette for µL work — introduces errors large enough to invalidate the result.
Volumetric pipette = one volume, highest accuracy. It has one mark, delivers one volume, and is the most accurate glass pipette for that volume. When precision matters more than flexibility, reach for the volumetric (bulb) pipette.
Key exam facts in one table
| Topic | Key fact |
|---|---|
| Glass pipette volume range | mL scale — not suitable for µL work |
| Graduated pipette synonym | Measuring pipette |
| Mohr's pipette | Drain-out; graduation stops above tip; do NOT blow out last drop |
| Serological pipette | Blow-out; graduation extends to tip; identified by blow-out ring at top; must blow out for full volume |
| Volumetric (bulb) pipette | Non-graduated; one fixed exact volume; highest accuracy; also called transfer pipette or bulb pipette |
| Pasteur pipette | Dropper; approximate transfer only; no graduation; not for accurate volume measurement |
| Class A vs. Class B accuracy | Class A: tighter specified error tolerances; Class B: double the error limits of Class A |
| Meniscus reading — colourless liquid | Read from the BOTTOM of the concave curve, eye level with mark |
| Meniscus reading — coloured/opaque liquid | Read from the TOP of the convex curve |
| Parallax error | Eye above or below mark level causes false high or false low reading |
| Mouth pipetting | Strictly prohibited in all laboratory settings |
| Pipette filler types | General purpose bulb, three-valve bulb, thumb wheel filler |
| Three-valve bulb — fill | Fill ~5 mm above mark, then drain to mark; set meniscus before dispensing |
| Broken tip on Mohr's | Discard — volume is undefined without the intact drain-out tip |
References
- Cheesbrough, M. (2006). District Laboratory Practice in Tropical Countries, Part 2 (2nd ed.). Cambridge University Press.
- ISO 835:2007. Laboratory glassware — Graduated pipettes. International Organization for Standardization.
- Clinical and Laboratory Standards Institute (CLSI). (2016). Clinical Microbiology Procedures Handbook (4th ed.). American Society of Microbiology. https://doi.org/10.1128/9781555818814
- Harvey, D. (2016). Analytical Chemistry 2.1. Community College of DuPage. https://chem.libretexts.org/Bookshelves/Analytical_Chemistry/Analytical_Chemistry_2.1\_(Harvey)
- Mahon, C. R., Lehman, D. C., & Manuselis, G. (2018). Textbook of Diagnostic Microbiology (6th ed.). Elsevier.
Frequently Asked Questions
What is the difference between a Mohr's pipette and a serological pipette?
How do you read the meniscus correctly in a glass pipette?
What is a volumetric pipette and when is it used?
Why is mouth pipetting prohibited in the laboratory?
What are the different accuracy classes of glass pipettes?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.