Enterococcus faecalis: Properties, Pathogenesis, Lab Diagnosis
Enterococcus faecalis virulence factors, intrinsic antibiotic resistance, and the salt tolerance, bile esculin, and PYR tests used for lab diagnosis.
Enterococci are catalase-negative, Gram-positive cocci in chains. Initially grouped under Group D Streptococcus, they were later reclassified into their own genus, Enterococcus, under family Enterococcaceae. E. faecalis and E. faecium are the two most common species involved in human infection, and increasingly important agents of hospital-acquired disease. E. faecalis is a major cause of hospital-acquired UTIs and endocarditis.
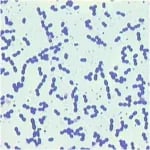 Figure: Enterococcus in gram-stain
Figure: Enterococcus in gram-stain
Habitat and Transmission
Enterococci are found in soil, food, water, and as normal flora of animals, birds, and humans. Enterococcus faecalis and Enterococcus faecium are normal flora of the human gastrointestinal tract (colon) and female genitourinary tract.
Transmission frequently occurs when endogenous strains gain access to sterile sites. For example; they may enter the bloodstream during gastrointestinal (GI) or genitourinary tract procedures and may infect other sites (e.g., endocarditis). Person-to-person transmission, directly or by contaminated medical equipment, allows nosocomial spread and colonization with multi-drug resistant strains. Once colonized, immunocompromised patients are at risk of developing infections.
Virulence Factors
Enterococci exhibit a number of virulence factors such as:
- Cytolysin/hemolysin: They lyse the sheep and human RBCs.
- Aggregation substances or pheromones: They help in the clumping of adjacent cells to facilitate plasmid exchange (transfers drug resistance).
- Extracellular surface protein (ESP): It helps in adhesion to the bladder mucosa.
- Common group D lipoteichoic acid antigen: It induces cytokine release such as tumor necrosis factor-α (TNF-α).
- Coccolysin: It inactivates endothelin, a vasoactive peptide.
How to Remember
Don't memorize the survival conditions and the identification tests as two separate lists, they're the same list. Enterococcus is, in the words of the primary literature on it, "a micro-organism that can survive extreme challenges." It grows in 6.5% NaCl, 40% bile, pH 9.6, temperatures from 10°C to 45°C, and survives 60°C for 30 minutes. Every one of your identification tests is just a deliberate attempt to kill it with one of those conditions and watch it shrug it off:
- Salt tolerance test = throwing 6.5% NaCl at it
- Bile esculin test = throwing 40% bile at it (plus checking esculin hydrolysis)
- Heat tolerance test = throwing 60°C at it
If you remember "this organism survives everything," the tests stop being arbitrary biochemistry and become obvious, of course the test for an organism defined by toughness is a toughness test.
One genuinely useful trap to know: PYR-positive is shared with S. pyogenes. Both GAS and Enterococcus give a positive PYR reaction, so PYR alone never finishes an identification. Catalase-negative, chains, PYR-positive, salt-tolerant gets you to Enterococcus, catalase-negative, chains, PYR-positive, beta-hemolytic, bacitracin-sensitive gets you to GAS. Same single test, different supporting cast.
For treatment, picture it as penicillin opening the door and the aminoglycoside walking through. Enterococci are intrinsically resistant to aminoglycosides alone because the drug can't penetrate the cell wall. Penicillin (or vancomycin) weakens that wall just enough for the aminoglycoside to get in, the synergy, not either drug alone, is what makes the combination bactericidal for serious infections like endocarditis.
Clinical manifestations
Because of their intrinsic and increased drug resistance, Enterococci are mostly responsible for nosocomial infections. Enterococci cause various infections such as:
- Urinary tract infections (cystitis, urethritis, pyelonephritis, and prostatitis).
- Bacteremia and mitral valve endocarditis. Endocarditis is rare but life-threatening.
- Intra-abdominal, pelvic, and soft tissue infections
- Ocular infections
- Rarely, meningitis and respiratory tract infections.
Laboratory Diagnosis
Gram-stained smear and culture. Alpha, beta, or nonhemolytic colonies on blood agar. Grows in 6.5% NaCl and hydrolyze esculin in the presence of 40% bile. Serologic tests are not useful. Enterococci show the following characteristics that help in their identification:
 Figure: Gamma-hemolytic colonies of Enterococcus faecalis. (Imagesource)
Figure: Gamma-hemolytic colonies of Enterococcus faecalis. (Imagesource)
- Enterococci are gram-positive oval cocci arranged in pairs; cocci in a pair are arranged at an angle to each other (spectacle-eyed appearance).
- Blood agar: It produces smooth, gray, non-hemolytic translucent colonies (rarely produces α or β hemolysis).
- MacConkey agar: It produces minute magenta pink colonies.
- Nutrient agar: It grows poorly.
- They can grow in presence of extreme conditions such as-6.5% NaCl, 40% bile, pH 9.6, 45°C, and 10°C.
- Heat tolerance test: They are relatively heat resistant, and can survive 60°C for 30 minutes.
- Groups: Enterococci can be divided into five groups-group I to V based on mannitol fermentation and arginine hydrolysis. E.faecalis and E. faecium belong to group II, which can be further differentiated by several biochemical properties.
Biochemical tests
Following biochemical tests are important for the differentiation and identification of Enterococcus faecalis.
| Name of the test | Enterococcus faecalis | Notes |
|---|---|---|
| Catalase test | Negative | To differentiate enterococci from staphylococci. |
| Hemolysis | Non-hemolytic | |
| Motility test | Non-motile | E. gallinarum and E. casseliflavus are motile. |
| Pyrrolidonyl-β-naphthylamide (PYR) test | Positive | Presumptive identification of group A beta-hemolytic streptococci and enterococci. |
| Esculin and bile-esculin test | Positive (Growth, black precipitate) | To differentiate enterococci and non-enterococcus group D streptococci. |
| Bile solubility test | Insoluble | S. pneumoniae is bile soluble. |
| LAP test | Positive | Identification of catalase-negative, gram-positive cocci. |
| Pyruvate broth | Positive | To differentiate E. faecalis (positive) from E. faecium (negative). |
| Salt tolerance test | Positive | To differentiate enterococci from non-enterococci. |
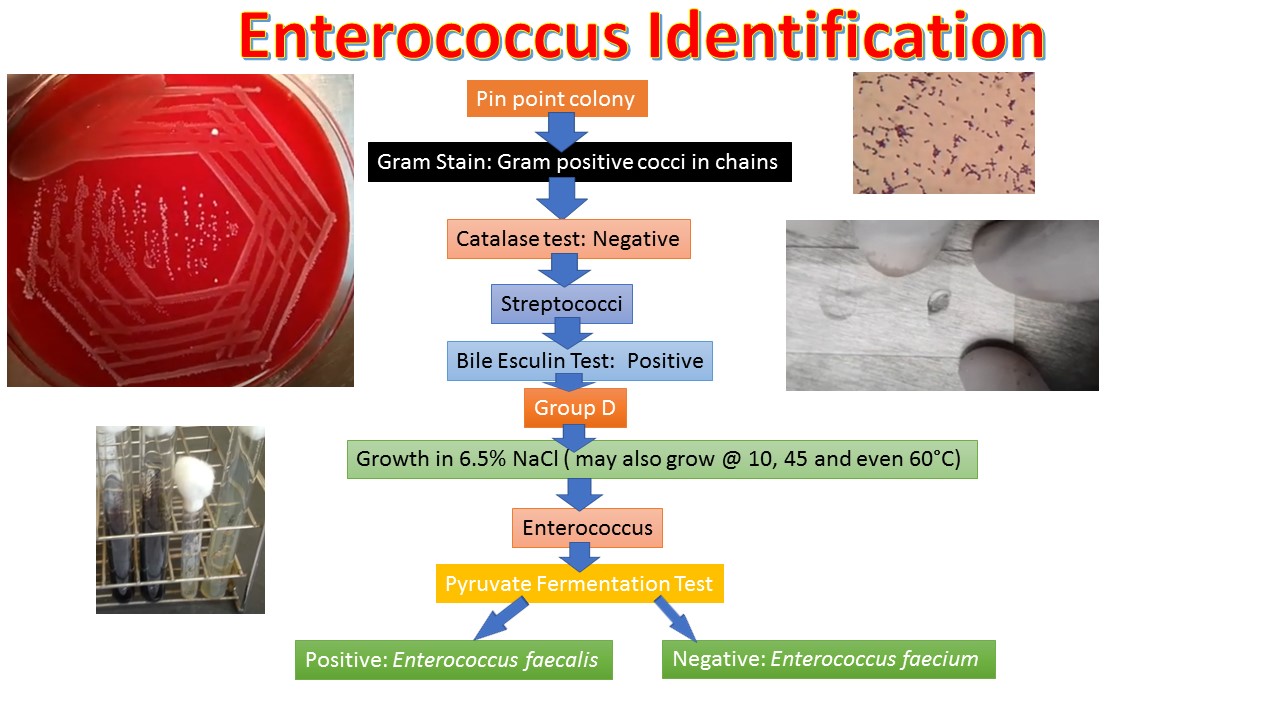 Figure: Flow chart for the identification of Enterococcus
Figure: Flow chart for the identification of Enterococcus
Where students actually get confused
- Catalase-negative does not mean Streptococcus. Enterococcus is catalase-negative too. The "spectacle-eyed" paired arrangement (oval cocci at an angle to each other) plus salt and bile tolerance are what actually separate it from true Streptococcus, not catalase.
- PYR-positive alone doesn't confirm Enterococcus. S. pyogenes is also PYR-positive. Salt tolerance and bile esculin are the tests that close the loop.
- Aminoglycoside resistance doesn't mean aminoglycosides are useless against Enterococcus. It means they're useless as monotherapy. Combined with a cell-wall-active agent, the synergy overcomes the penetration problem, this is the standard approach for serious enterococcal infections, not a contradiction.
- VRE doesn't mean untreatable. Vancomycin-resistant strains (more often E. faecium than E. faecalis) still respond to linezolid and other agents. Resistance to one drug class isn't the end of the treatment conversation.
Where students actually get confused
- Catalase-negative does not mean Streptococcus. Enterococcus is catalase-negative too. The "spectacle-eyed" paired arrangement (oval cocci at an angle to each other) plus salt and bile tolerance are what actually separate it from true Streptococcus, not catalase.
- PYR-positive alone doesn't confirm Enterococcus. S. pyogenes is also PYR-positive. Salt tolerance and bile esculin are the tests that close the loop.
- Aminoglycoside resistance doesn't mean aminoglycosides are useless against Enterococcus. It means they're useless as monotherapy. Combined with a cell-wall-active agent, the synergy overcomes the penetration problem, this is the standard approach for serious enterococcal infections, not a contradiction.
- VRE doesn't mean untreatable. Vancomycin-resistant strains (more often E. faecium than E. faecalis) still respond to linezolid and other agents. Resistance to one drug class isn't the end of the treatment conversation.
Self-check questions
- Why does a positive PYR test alone not distinguish Enterococcus from S. pyogenes?
- What do the salt tolerance, bile esculin, and heat tolerance tests have in common as identification strategies?
- Why is aminoglycoside monotherapy ineffective against Enterococcus, and why does adding penicillin change that?
- A catalase-negative coccus grows in 6.5% NaCl. What does this rule in, and what would you still need to confirm the species?
Treatment
Enterococci show intrinsic resistance to cephalosporins and cotrimoxazole. Most strains of enterococci are resistant to penicillins, aminoglycosides, and sulfonamides. Resistance is overcome by combination therapy with penicillin (or ampicillin) and aminoglycoside such as gentamicin (due to synergistic effect) and this remains the standard therapy for life-threatening enterococcal infections. Aminoglycoside alone is ineffective because it cannot penetrate. Penicillin or vancomycin weakens the cell wall, allowing the aminoglycoside to penetrate.
Vancomycin is usually indicated in resistant cases but resistance to vancomycin has also been reported. Linezolid can be used to treat vancomycin-resistant enterococci (VRE).
Prevention
Penicillin and gentamicin should be given to patients with damaged heart valves prior to intestinal or urinary tract procedures. No vaccine is available.
References
- Madigan Michael T, Bender, Kelly S, Buckley, Daniel H, Sattley, W. Matthew, & Stahl, David A. (2018). Brock Biology of Microorganisms (15th Edition). Pearson.
- Georges, M., Odoyo, E., Matano, D., Tiria, F., Kyany’a, C., Mbwika, D., Mutai, W. C., & Musila, L. (2022). Determination of Enterococcus faecalis and Enterococcus faecium Antimicrobial Resistance and Virulence Factors and Their Association with Clinical and Demographic Factors in Kenya. Journal of pathogens, 2022, 3129439. https://doi.org/10.1155/2022/3129439
- Kayaoglu, G., & Ørstavik, D. (2004). Virulence factors of Enterococcus faecalis: relationship to endodontic disease. Critical reviews in oral biology and medicine : an official publication of the American Association of Oral Biologists, 15(5), 308–320. https://doi.org/10.1177/154411130401500506
Frequently Asked Questions
Why isn't a positive PYR test enough to identify Enterococcus faecalis?
Why are aminoglycosides ineffective against Enterococcus when used alone?
Does vancomycin-resistant Enterococcus (VRE) mean the infection can't be treated?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.