Taenia solium vs Taenia saginata: Life Cycle, Cysticercosis, and Key Differences
Why does Taenia solium cause cysticercosis and neurocysticercosis while Taenia saginata does not? Complete comparison of life cycle, morphology, and lab diagnosis — with the egg-infectivity mechanism explained.
A 24-year-old man in rural India is brought to the emergency department after his first seizure. He has no history of head injury, no fever, no family history of epilepsy. A CT scan shows multiple small, calcified lesions scattered through his brain; the unmistakable signature of neurocysticercosis. He has never knowingly eaten undercooked pork. When asked, he reveals that a household member has been passing tapeworm segments in their stool for months.
 This is the central paradox of the genus Taenia that every microbiology and parasitology exam will test: this man's seizures were not caused by eating contaminated pork. They were caused by swallowing eggs — most likely from a household member's contaminated hands or food — even though he may never have eaten pork at all. Understanding why Taenia solium can do this, while its close relative Taenia saginata cannot, is the single most clinically important distinction in this entire topic.
This is the central paradox of the genus Taenia that every microbiology and parasitology exam will test: this man's seizures were not caused by eating contaminated pork. They were caused by swallowing eggs — most likely from a household member's contaminated hands or food — even though he may never have eaten pork at all. Understanding why Taenia solium can do this, while its close relative Taenia saginata cannot, is the single most clinically important distinction in this entire topic.
The Three Human *Taenia* Species
Taeniasis — intestinal infection with the adult tapeworm — is caused by three species, all transmitted to humans through undercooked meat:
| Species | Common name | Intermediate host | Meat source |
|---|---|---|---|
| Taenia solium | Pork tapeworm | Pig | Pork (muscle) |
| Taenia saginata | Beef tapeworm | Cattle | Beef |
| Taenia asiatica | Asian tapeworm | Pig | Pork, specifically liver |
Humans are the only definitive host for all three species — the adult tapeworm lives and reproduces sexually only in the human small intestine. T. solium and T. saginata have worldwide distribution, with higher prevalence in developing regions; T. asiatica is geographically restricted to Asia (Taiwan, South Korea, China, Indonesia, Thailand, the Philippines, Vietnam, and parts of Nepal).
Only T. solium poses a major public health threat. T. saginata and T. asiatica cause mild, usually asymptomatic intestinal taeniasis. T. solium causes the same intestinal disease — but uniquely among the three, it can also cause cysticercosis, including neurocysticercosis, a leading cause of acquired epilepsy in endemic regions. The World Health Organization attributes up to 30% of epilepsy cases in some T. solium-endemic areas to neurocysticercosis.
Life Cycle
Taeniasis (common pathway — all three species)
- The adult tapeworm lives in the human small intestine, attached by its scolex. Gravid proglottids (egg-containing segments) detach and pass in the stool, or eggs are shed directly into the environment.
- The intermediate host (pig for T. solium and T. asiatica; cattle for T. saginata) ingests vegetation contaminated with eggs or proglottids.
- In the animal's intestine, the egg hatches and releases an oncosphere, which invades the intestinal wall and migrates to striated muscle (or, for T. asiatica, preferentially the liver), developing into a cysticercus — a fluid-filled larval cyst containing an immature scolex.
- A cysticercus can survive for years in the intermediate host.
- Humans become infected by eating raw or undercooked meat containing viable cysticerci.
- In the human intestine, the cysticercus evaginates, attaches to the intestinal wall by its scolex, and matures into an adult tapeworm over approximately 2 months. The adult worm can survive for years, continuously producing new proglottids.
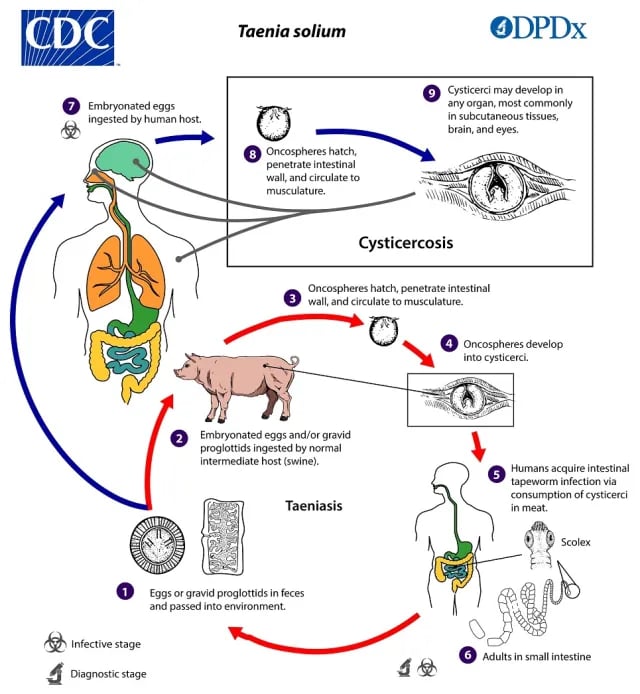 Figure: Life Cycle of Taenia solium (source: CDC)
Figure: Life Cycle of Taenia solium (source: CDC)
Cysticercosis (unique to *Taenia solium*)
This is the pathway that does not exist for T. saginata, and understanding why is the core teaching point of this article.
- A person ingests eggs — not cysticerci, not undercooked pork — typically through fecal-oral contamination: contaminated food or water, poor hand hygiene after contact with a tapeworm carrier's stool, or autoinfection (a person who already has intestinal taeniasis re-ingesting their own eggs via contaminated hands or, rarely, reverse peristalsis carrying proglottids back into the stomach).
- The egg hatches in the human intestine, releasing an oncosphere.
- The oncosphere invades the intestinal wall and migrates through the bloodstream to striated muscle, subcutaneous tissue, the eye, or — critically — the central nervous system, where it develops into a cysticercus.
- In this scenario, the human is acting as an accidental intermediate host — a role normally filled by the pig. The human did not need to eat pork at all; they only needed to ingest eggs shed by someone (possibly themselves) who has intestinal taeniasis.
When cysticerci localize in the brain, the result is neurocysticercosis — the most serious complication of T. solium infection, presenting with seizures and a range of neurological symptoms depending on the number, size, and location of the cysts.
Why Only *T. solium* Causes Cysticercosis
This is the question every student gets wrong on first encounter, and the answer is a single, precise biological fact:
Eggs of Taenia solium are directly infectious to humans. Eggs of Taenia saginata are not.
It is not that T. saginata lacks an intermediate-host stage, or that cattle are somehow "safer" hosts than pigs. The eggs themselves differ in their capacity to infect human tissue. T. saginata eggs, when ingested by a human, simply fail to establish the oncosphere migration and tissue cyst formation that T. solium eggs readily accomplish. The morphology of the two species' eggs is, notably, indistinguishable under the microscope — you cannot tell them apart by looking at an egg. The difference is biological infectivity, not appearance.
This means a person can develop cysticercosis from T. solium eggs without ever eating pork at all — exposure to a tapeworm carrier's contaminated environment is sufficient. Conversely, eating undercooked pork containing T. solium cysticerci causes only intestinal taeniasis (the adult worm), not cysticercosis directly — cysticercosis specifically requires ingesting the eggs.
Whether T. asiatica can cause cysticercosis in humans remains scientifically unclear — unlike the firm "yes" for T. solium and "no" for T. saginata, this is genuinely an open question in the literature.
Complete Comparison Table
| Feature | Taenia solium | Taenia saginata | Taenia asiatica |
|---|---|---|---|
| Common name | Pork tapeworm | Beef tapeworm | Asian tapeworm |
| Definitive host | Human | Human | Human |
| Intermediate host | Pig | Cattle | Pig (liver tropism) |
| Disease in humans | Taeniasis and cysticercosis | Taeniasis only | Taeniasis only (cysticercosis status unclear) |
| Geographic distribution | Worldwide, higher in developing regions | Worldwide | Limited to Asia |
| Adult worm size | 2–7 m | 5 m (occasionally up to 25 m) | 4–8 m |
| Scolex | Armed — rostellum with double row of 25–30 alternating large and small hooklets | Unarmed — no rostellum or hooklets | Similar to T. saginata; rostellar hooks may be present (variable) |
| Number of proglottids | ~1,000 | 1,000–2,000 | Similar to T. saginata |
| Gravid uterus branches | 5–13 lateral branches per side | 15–30 lateral branches per side (densely packed) | Similar to T. saginata |
| Proglottid expulsion | Passively, in chains of 5–6 | Singly, often motile, may actively crawl out | Similar to T. saginata |
| Eggs per proglottid | ~50,000 | Up to 100,000 | Not well characterised |
| Egg morphology | 30–35 μm, bile-stained, indistinguishable from T. saginata | Indistinguishable from T. solium | Indistinguishable from the other two |
| Eggs infectious to humans? | Yes — causes cysticercosis | No | Unclear |
| Source of human infection (taeniasis) | Undercooked measly pork (cysticerci) | Undercooked measly beef (cysticerci) | Undercooked pork, especially liver |
| Cooking temperature to kill cysticerci | 80°C for at least 10 minutes (research-based) | 63°C internal temperature with 3-minute rest | 63°C (similar to T. saginata) |
Clinical Disease
Taeniasis (all three species)
Most infections are asymptomatic or produce only mild gastrointestinal symptoms: abdominal discomfort, epigastric pain, nausea, and occasionally diarrhoea. The most striking clinical feature — and often the only symptom that brings a patient to medical attention — is the passive (or for T. saginata, sometimes active) passage of proglottids in the stool.
Cysticercosis and Neurocysticercosis (*T. solium* only)
Cysticerci can develop in skeletal muscle, subcutaneous tissue, the eye, and the central nervous system. In most peripheral locations, cysts cause minimal symptoms and may spontaneously calcify and degenerate over time without treatment.
Neurocysticercosis — cysticerci in the brain — is the clinically significant form. Presentation depends on the number, size, and location of cysts, and includes seizures (the most common presentation), headache, raised intracranial pressure, and focal neurological deficits. Fewer than half of patients with neurocysticercosis have concurrent intestinal taeniasis (and therefore detectable eggs in stool) — meaning a negative stool examination does not rule out neurocysticercosis in a patient with suggestive neurological symptoms.
Laboratory Diagnosis
Taeniasis
Diagnosis relies on identifying eggs, proglottids, or scolex in the stool, or eggs on a perianal swab.
Eggs: 30–35 μm in diameter, bile-stained, with an internal oncosphere containing six refractile hooks. Eggs do not float in saturated NaCl solution — a relevant point for flotation-based concentration techniques. Critically, eggs of T. solium, T. saginata, and T. asiatica are morphologically indistinguishable from each other. Species identification on stool examination alone is not possible by egg morphology — it requires examining the scolex (armed vs unarmed) or gravid proglottid (lateral branch count) if either is recovered intact, or molecular/PCR methods for definitive speciation.
Caution: Stool specimens from suspected T. solium taeniasis should be handled with extreme care — ingestion of the eggs by laboratory personnel can itself cause cysticercosis.
Cysticercosis and Neurocysticercosis
Diagnosis is primarily clinical and radiological, supported by serology:
- Neuroimaging (CT/MRI): The primary diagnostic tool for neurocysticercosis. Findings include solid nodules, viable cysticerci, calcified cysts, ring-enhancing lesions, or hydrocephalus. Calcified lesions are also visible on plain X-ray in subcutaneous or muscle locations.
- Serology: IgG is the predominant antibody of diagnostic value; IgA, IgE, and IgM contribute little. The CDC immunoblot (EITB) assay using serum or CSF is highly specific and more sensitive than standard ELISA, particularly when more than two CNS lesions are present. Cross-reactions can occur with Echinococcus, filariasis, and T. saginata infections, complicating interpretation.
- Antigen detection: ELISA-based detection of antigen secreted by viable T. solium metacestodes is available and indicates active, viable infection (unlike antibody tests, which can remain positive after cyst death).
- Stool examination: Supportive only — a positive stool result (eggs/proglottids) supports the diagnosis of neurocysticercosis but is not diagnostic on its own, and a negative result does not exclude it, since fewer than half of neurocysticercosis patients have concurrent intestinal taeniasis.
- Histopathology: When cysticerci are surgically removed, microscopic examination for the characteristic scolex with suckers and hooks confirms the diagnosis.
How to Remember
Armed vs Unarmed Scolex: "Solium is armed and dangerous" — T. solium has an armed scolex (rostellum with a double row of hooklets) and is the dangerous species (causes cysticercosis). T. saginata is unarmed and comparatively harmless (taeniasis only).
Why solium but not saginata causes cysticercosis: "It's the egg, not the meat" — cysticercosis is never caused by eating meat (that only gives taeniasis, the adult worm). It is always caused by ingesting eggs. T. solium eggs are infectious to humans; T. saginata eggs are not. Same exposure route (fecal-oral), different biological outcome.
Lateral branch count: "Solium: small number — Saginata: sprawling number" — T. solium has 5–13 lateral uterine branches per side; T. saginata has 15–30. More branches, more eggs per proglottid (saginata up to 100,000 vs solium's ~50,000) — but remember, more eggs does NOT mean more danger, since saginata eggs aren't infectious to humans regardless of quantity.
Where Students Actually Get Confused
1. "T. saginata doesn't cause cysticercosis because it's a different, less dangerous species overall." This framing is wrong and is the single most common misconception in this topic. The reason is mechanistically specific: T. saginata eggs are simply not infectious to human tissue. It has nothing to do with general "danger level" of the species, parasite size, or geography — it is a precise biological property of the egg itself.
2. "Eating undercooked pork causes cysticercosis." No — eating undercooked pork containing cysticerci causes taeniasis (the adult intestinal tapeworm). Cysticercosis requires ingesting eggs, typically via fecal-oral contamination from a tapeworm carrier (who could be the patient themselves, via autoinfection, or someone else in the household). A person who has never eaten pork can still develop cysticercosis.
3. "A negative stool exam rules out neurocysticercosis." Fewer than half of patients with neurocysticercosis have detectable eggs or proglottids in their stool at the time of presentation, since the adult intestinal worm and the tissue cyst infection are not always present together. Neurocysticercosis diagnosis relies primarily on neuroimaging and serology, not stool examination.
4. "Taenia eggs can be told apart under the microscope." They cannot. Eggs of T. solium, T. saginata, and T. asiatica are morphologically identical — same size range, same bile staining, same internal oncosphere with six hooklets. Species differentiation requires examining the scolex or proglottid morphology, or molecular methods (PCR-RFLP, hematoxylin-eosin staining combined with PCR).
5. "Taenia asiatica is just a regional variant of T. saginata." While genetically and morphologically very similar to T. saginata, T. asiatica has a distinct intermediate host preference (pigs, not cattle) and tissue tropism (liver, not muscle) — and crucially, whether it can cause human cysticercosis remains scientifically unresolved, unlike the clear-cut answers for the other two species.
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Definitive host (all 3 species) | Human | Sexual reproduction occurs in human intestine |
| T. solium intermediate host | Pig | Pork = solium |
| T. saginata intermediate host | Cattle | Beef = saginata |
| T. asiatica intermediate host | Pig (liver tropism) | Pork liver = asiatica |
| Causes cysticercosis | T. solium ONLY (T. asiatica unclear; T. saginata NO) | "It's the egg, not the meat" |
| Armed scolex | T. solium | "Solium is armed and dangerous" |
| Unarmed scolex | T. saginata | No rostellum, no hooklets |
| Lateral uterine branches | Solium: 5–13; Saginata: 15–30 | Saginata sprawls more |
| Eggs per proglottid | Solium: ~50,000; Saginata: up to 100,000 | More eggs ≠ more danger |
| Egg morphology | Identical across all 3 species; 30–35 μm, bile-stained | Cannot speciate by egg alone |
| Eggs float in saturated NaCl? | No | Use sedimentation, not flotation |
| Cysticercosis transmission route | Fecal-oral (eggs) — NOT via undercooked meat | Autoinfection possible |
| Accidental intermediate host (cysticercosis) | Human (normally fulfilled by pig) | "Accidental" = not the parasite's intended host |
| Most serious complication | Neurocysticercosis (cysticerci in CNS) | Leading cause of acquired epilepsy in endemic areas |
| % epilepsy attributable to NCC (endemic areas) | Up to 30% (WHO) | Major global health burden |
| Best diagnostic test for taeniasis | Stool microscopy (eggs/proglottids/scolex) | Handle with care — eggs are infectious |
| Best diagnostic test for neurocysticercosis | CT/MRI + serology (CDC immunoblot/EITB) | Stool exam is supportive only, not diagnostic |
| Stool positive in NCC patients | <50% | Negative stool does NOT exclude NCC |
Self-Check Questions
- A patient develops neurocysticercosis but states they have never eaten pork in their life. How is this possible?
- Why can't T. solium and T. saginata eggs be distinguished under the microscope, and what methods are used instead to identify the species?
- A stool examination for a patient with new-onset seizures and brain lesions on CT is negative for Taenia eggs. Does this rule out neurocysticercosis?
- What is the single biological difference that explains why T. solium causes cysticercosis but T. saginata does not?
- Identify the host type assigned to a human who develops cysticercosis, and explain why this host role is called "accidental."
- Which species has an armed scolex, and what is the clinical significance of remembering this distinction?
Answers
- Cysticercosis is acquired by ingesting Taenia solium eggs, not by eating undercooked pork. The patient most likely ingested eggs through fecal-oral contamination — contaminated food, water, or contact with a household member (possibly asymptomatic) who has intestinal taeniasis and is shedding eggs. Eating pork causes taeniasis (the adult worm), not cysticercosis.
- Eggs of all three Taenia species are morphologically identical — 30–35 μm, bile-stained, with an internal oncosphere containing six refractile hooks. Species cannot be distinguished by egg appearance. Identification instead relies on examining the scolex (armed in T. solium, unarmed in T. saginata) or the gravid proglottid's lateral uterine branch count (5–13 for solium, 15–30 for saginata), or molecular methods such as PCR-restriction enzyme analysis when intact specimens are unavailable.
- No. Fewer than half of patients with neurocysticercosis have concurrent intestinal taeniasis with detectable eggs in stool. A negative stool result does not exclude the diagnosis. Neurocysticercosis is primarily diagnosed through neuroimaging (CT/MRI showing characteristic lesions) supported by serology (CDC immunoblot/EITB), not stool examination.
- Eggs of Taenia solium are biologically infectious to human tissue, while eggs of Taenia saginata are not — despite being morphologically identical. This is a specific property of the egg itself, not a difference in general pathogenicity, parasite size, or any other species characteristic.
- The human is classified as an accidental intermediate host. This role is normally fulfilled by the pig, which is the natural intermediate host where T. solium larvae (cysticerci) develop. When a human ingests eggs instead of acting as the definitive host (which requires ingesting cysticerci in meat), they inadvertently take on the pig's biological role — hence "accidental," since this is not the parasite's typical life cycle pathway through humans.
- Taenia solium has the armed scolex (rostellum with a double row of 25–30 alternating large and small hooklets). The clinical significance of this mnemonic ("solium is armed and dangerous") is that it links a memorable morphological feature directly to the species that causes the dangerous complication — cysticercosis and neurocysticercosis — helping distinguish it from the comparatively harmless, unarmed T. saginata.
References
- Harrison, L. J., & Parkhouse, R. M. (1989). Taenia saginata and Taenia solium: reciprocal models. Acta Leidensia, 57(2), 143–152.
- Mayta, H., Talley, A., Gilman, R. H., Jimenez, J., Verastegui, M., Ruiz, M., Garcia, H. H., & Gonzalez, A. E. (2000). Differentiating Taenia solium and Taenia saginata infections by simple hematoxylin-eosin staining and PCR-restriction enzyme analysis. Journal of Clinical Microbiology, 38(1), 133–137. https://doi.org/10.1128/JCM.38.1.133-137.2000
- Sastry, A. S., & Bhat, S. (2014). Essentials of Medical Parasitology. Jaypee Brothers Medical Publishers (P) Ltd. ISBN: 978-93-5152-329-1
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- World Health Organization. (2022). Taeniasis/cysticercosis. WHO Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/taeniasis-cysticercosis
- CDC – DPDx: Taeniasis. Centers for Disease Control and Prevention. https://www.cdc.gov/dpdx/taeniasis/index.html
- CDC – DPDx: Cysticercosis. Centers for Disease Control and Prevention. https://www.cdc.gov/dpdx/cysticercosis/index.html
- Ale, A., Victor, B., Praet, N., et al. (2014). Epidemiology and genetic diversity of Taenia asiatica: a systematic review. Parasites & Vectors, 7, 45. https://doi.org/10.1186/1756-3305-7-45
Frequently Asked Questions
Why does Taenia solium cause cysticercosis but Taenia saginata does not?
Can a person get neurocysticercosis without ever eating pork?
How can Taenia solium and Taenia saginata be distinguished if their eggs look identical?
Why is a negative stool exam not enough to rule out neurocysticercosis?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.